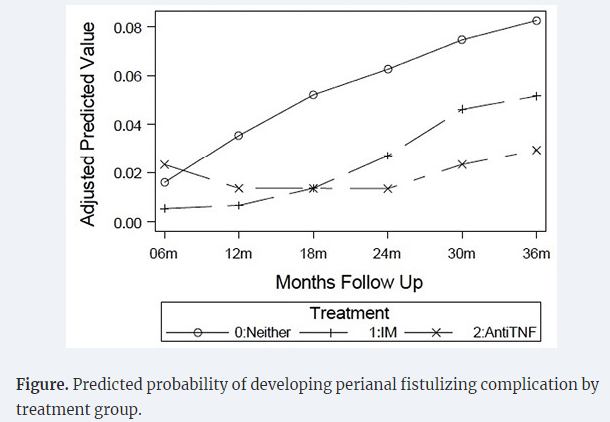
The authors utilized the prospectively-enrolled RISK cohort to assess the effect of early ANTI-TNF therapy and the development of perianal fistulizing complications (PFCs); this included 621 propensity-matched pediatric patients without PFCs at enrollment. ”The study included a moderately ill population, including 21% with growth delay, 43% with deep ulcers, and 70% with weighted pediatric Crohn’s disease activity index (wPCDAI) >30.”
Key findings:
Anti-TNF therapy was associated with 79% reduced odds of developing PFCs
The presence of perianal lesions increased the risk of PFCs more than 3-fold
My take: This study, in agreement with others (see below), shows that early treatment with effective therapy reduces the risk of disease complications like perianal fistulas.
A Berkwitt et al. NEJM 2024; 390: 358-366.Case 3-2024: An 8-Week-Old Male Infant with Inconsolable Crying and Weakness
This case report describes an 8 week old who been well until 7 days before the current presentation, when irritability, less frequent stooling and frequent crying developed. He was seen by his primary care clinic and symptoms were attributed to gas. Several days later, he presented to the emergency department with persistent crying but he had developed lethargy and weakness.
This case report details potential reasons for irritability in infants:
Infections
Neurologic causes including hydrocephalus
Ocular/skin such as a corneal abrasion and hair tourniquet
Cardiopulmonary causes such as heart failure and myocarditis
Gastrointestinal causes like colic, constipation gas, and reflux
Genitourinary like hernia and torsion
Musculoskeletal like fractures
Cancer including neuroblastoma and leukemia
Metabolic causes
Ingestions/Toxins
Then, the authors turn their attention to potential reasons for hypotonia:
CNS disease -accounts for 60 to 80% of cases of hypotonia, specifically hypoxic–ischemic encephalopathy and cerebral palsy
PNS disease -need to be considered in those with normal neuroimaging. To have an acquired PNS disease, the authors considered mainly botulism and Guillain-Barre syndrome.
Ultimately, the authors concluded that the infant likely had botulism which was in fact the correct diagnosis, confirmed by a stool test for Clostridium botulinum toxin type A (generally available only through local public health departments). Also, “On further interviewing, the patient’s family members reported that he typically had hard stools every 2 to 3 days. Two days before admission, the infant appeared to have abdominal discomfort, which his family members presumed was from constipation or gas. Honey was given to try to soothe him.”
Teaching points:
Don’t give honey or corn syrup to a baby, though “clearly defined food exposures, such as exposures to honey or corn syrup, account for only a minority of cases.8..Often, there is a history involving rural living, dust production, or nearby soil perturbation.9“
Give Baby BIG (infant botulism immune globulin) while waiting for results.
Try to ascertain dietary exposures when obtaining a history.
Of patients not achieving clinical response during 12-week induction, 53.7% achieved response following extended induction (additional 3 doses of IV infusion every 4 weeks)
With “extended induction,” total of 80.3% mirikizumab-treated patients achieved clinical response by W24
Methods: A network meta-analysis (NMA) was conducted to evaluate comparative efficacy of licensed biologics. Phase 3 randomized controlled-trials (RCTs) evaluating biologics approved by the European Medicines Agency or United States Food and Drug Administration as of 31 March 2023 for maintenance treatment of adult patients with moderate-to-severe CD were included, i.e. infliximab (IFX) intravenous (IV) and SC, adalimumab (ADL) SC, vedolizumab (VDZ) IV and SC, ustekinumab (UST) SC, and risankizumab (RZB) SC.
Key findings:
Among 8 comparator arms, IFX SC 120 mg every 2 weeks (Q2W) showed the highest odds ratio (95% credible interval) vs. PBO for clinical remission during the maintenance phase (3.52 [2.18–5.65]).
My take: This meta-analysis shows a favorable response for IFX SC; however, head-to-head trials are needed to really determine which biologic has the highest efficacy.
In this cross-sectional study with 104 children (24 with fatigue), biological parameters (CRP, fecal calprotectin) did not discriminate fatigued from non-fatigued patient
In this multicenter prospective study with 117 patients, the authors examined the success rate of adalimumab (ADA) in patients with CD with an intra-abdominal abscess resolved without surgery.
Key findings:
At W24, the survival rate without abscess recurrence or surgery was 74% (n=87)
Abscess drainage was significantly associated with ADA failure at W24 (odds ratio, 4.18)
My take (borrowed from authors): Provided that the abscess was carefully managed before initiating medical treatment, this study showed the high efficacy of ADA in the short and long term in biologic-naïve patients with CD complicated by an intra-abdominal abscess
There is little evidence that we are reducing diagnostic errors despite more lab testing and more imaging. “One of the important reasons for these errors is failure to consider the diagnosis when evaluating the patient.” This, in turn, may be related to brief office visits.
AI support to radiologists for a large mammography study “showed improvement in accuracy with a considerable 44% reduction of screen-reading workload.” The cancer detection rate was 6.1 per 1000 compared to 5.1 per 1000 in the control group.
In difficult NEJM CPC cases, large language AI model (LLM) outperformed clinicians (see slide below).” The LLM was nearly twice as accurate as physicians for accuracy of diagnosis, 59.1 versus 33.6%, respectively.”
“Likewise, the cofounder of OpenAI, Ilya Sutskever, was emphatic about AI’s future medical superintelligence: ‘If you have an intelligent computer, an AGI [artificial general intelligence], that is built to be a doctor, it will have complete and exhaustive knowledge of all medical literature, it will have billions of hours of clinical experience.’ “
My take (borrowed from Dr. Topol): “We are certainly not there yet. But in the years ahead, …it will become increasingly likely that AI will play an invaluable role in providing second opinions with automated, System 2 machine-thinking, to help us move toward the unattainable but worthy goal of eradicating diagnostic errors.”
Seven pediatric patients with perianal Crohn’s disease were treated with mesenchymal stem cells. Key finding: At 6 months, 83% had complete clinical and radiographic healing. This healing rate is higher than “the 50% efficacy reported by the only completed randomized control phase III clinical trial.[ADMIRE study].”
MA Baarslag et al. NEJM 2023; 389: 1790-1796. Severe Immune-Related Enteritis after In Utero Exposure to Pembrolizumab
This case report details severe immune-related gastroenterocolitis after in utero exposure to pembrolizumab, an anti–PD-1 agent; the infant presented at 4 months of life. Extensive testing did not identify any underlying causes of VEO-IBD. This infant required TPN for a short period, but subsequently responded to treatment with glucocorticosteroids and infliximab (with plans to continue until at least 3 years of age). Both programmed death 1 (PD-1) and cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) immune checkpoint inhibitors are negative regulators of T-cell immune function. Inhibition of these targets, resulting in increased activation of the immune system and can result in medication-induced colitis in the patients who take them and potentially in infants exposed to these agents in utero.
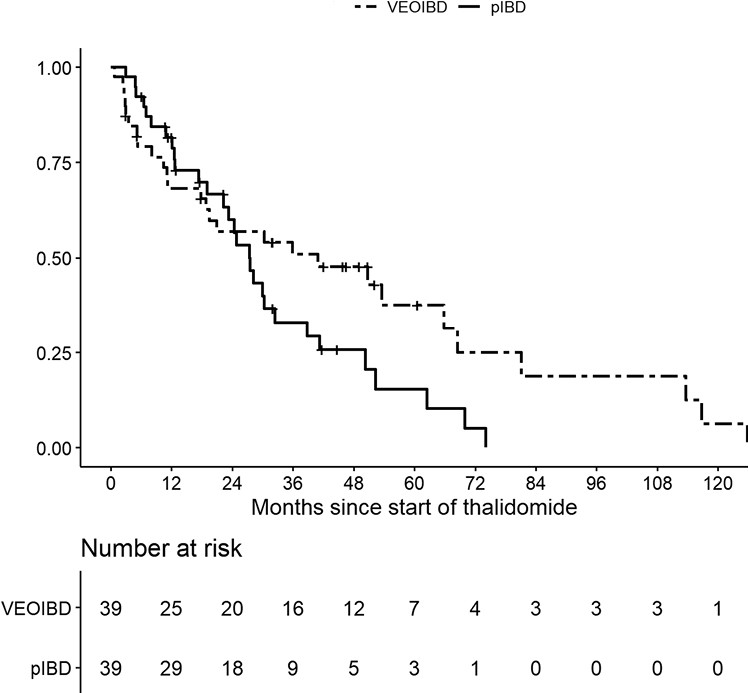
M Bramuzzo et al. Inflamm Bowel Dis 2024; 30: 20-28. https://doi.org/10.1093/ibd/izad018. Efficacy and Tolerance of Thalidomide in Patients With Very Early Onset Inflammatory Bowel Disease
This retrospective study with 39 patients with VEO and 39 patients with pediatric IBD.
Key findings:
The treatment persistence at 1, 2, and 3 years was 68.2%, 57.0%, and 50.9% for VEOIBD patients and 81.7%, 60.0% and 33.0% for pIBD patients, respectively
A significantly higher proportion of VEOIBD patients discontinued therapy due to lack of efficacy (48.2% vs 17.2%; P = .03), while AEs were the main reason for discontinuation in pIBD patients
A significatively lower number of VEOIBD patients experienced AEs compared with pIBD patients (14 [35.9%] vs 30 [76.9%]; P = .0005).
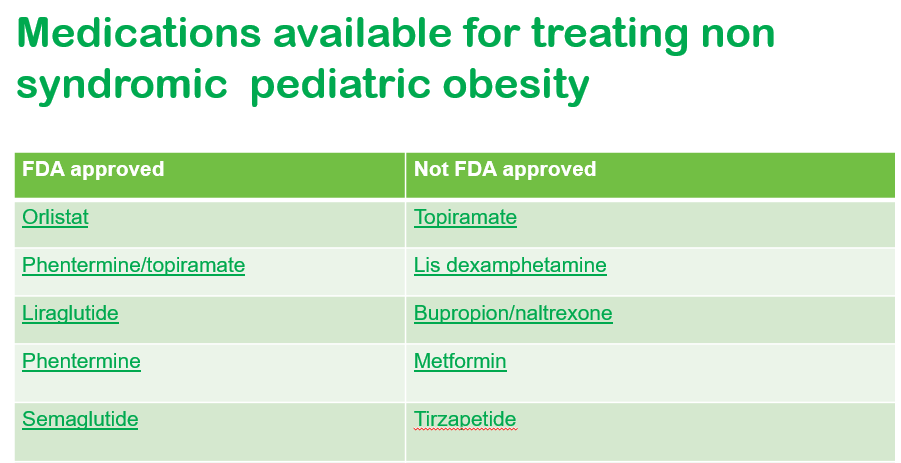
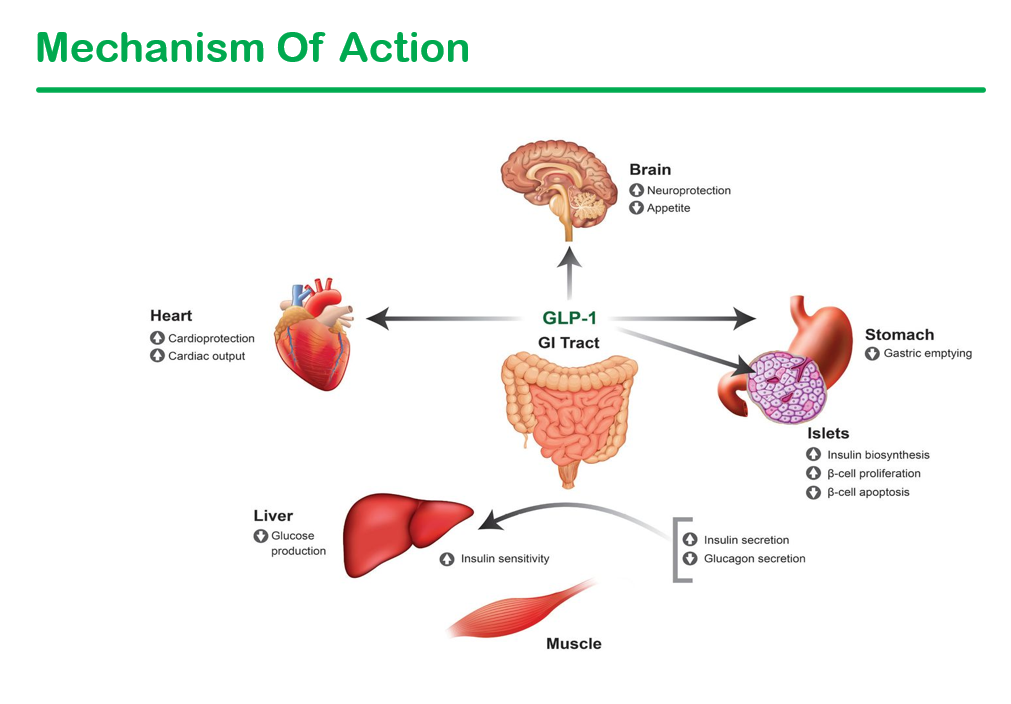
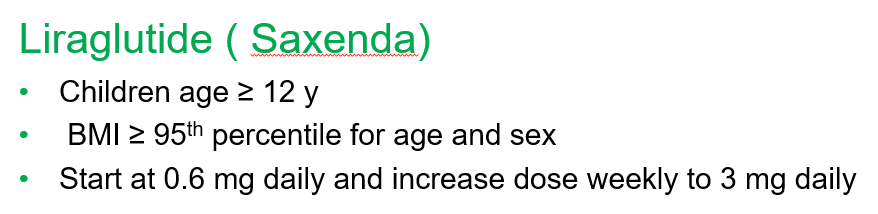
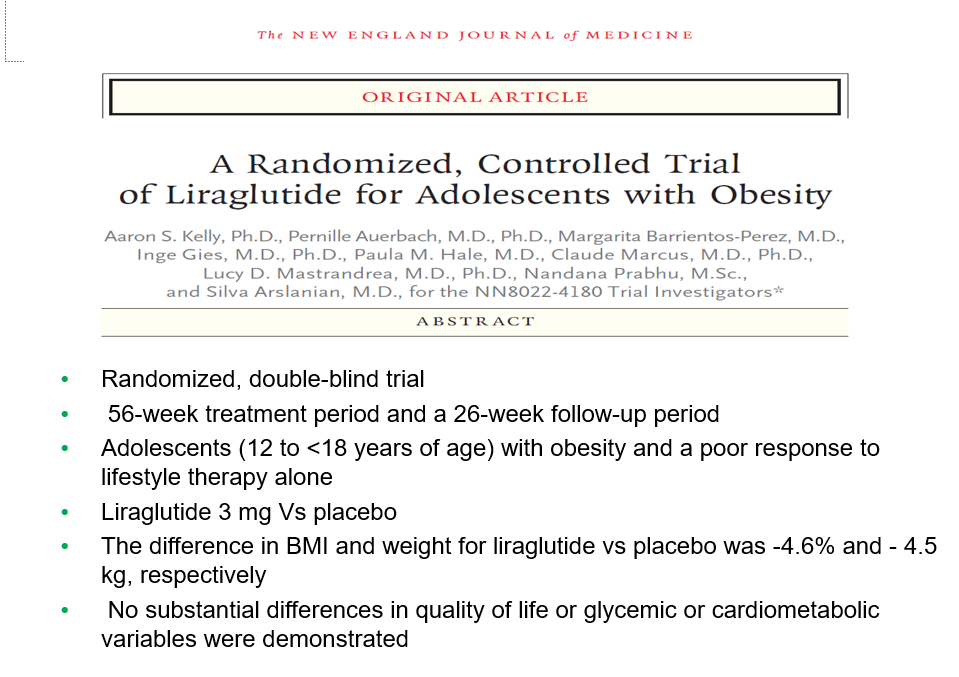
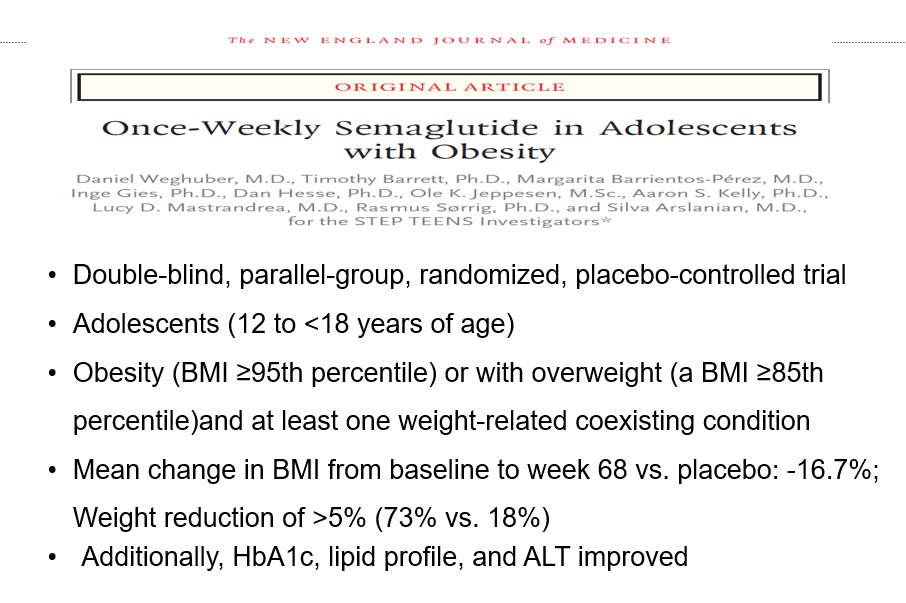
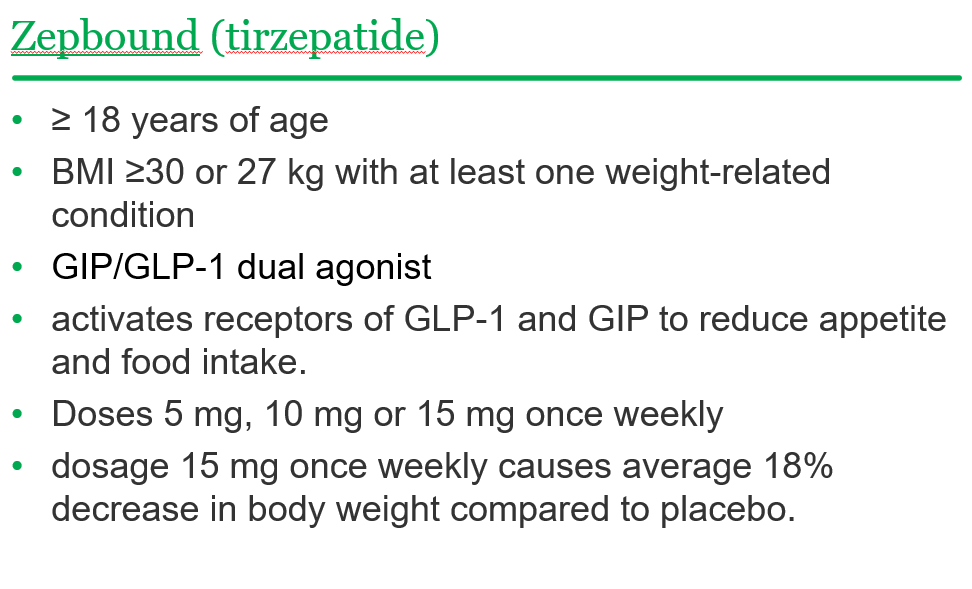
Recently, Dr. Shruthi Arora, an Emory Pediatric Endocrinologist and part of CHOA’s Strong4Life team, provided a terrific review of pediatric obesity pharmacology for our group.
Here are a few slides from Dr. Arora’s lecture:
General points from this lecture:
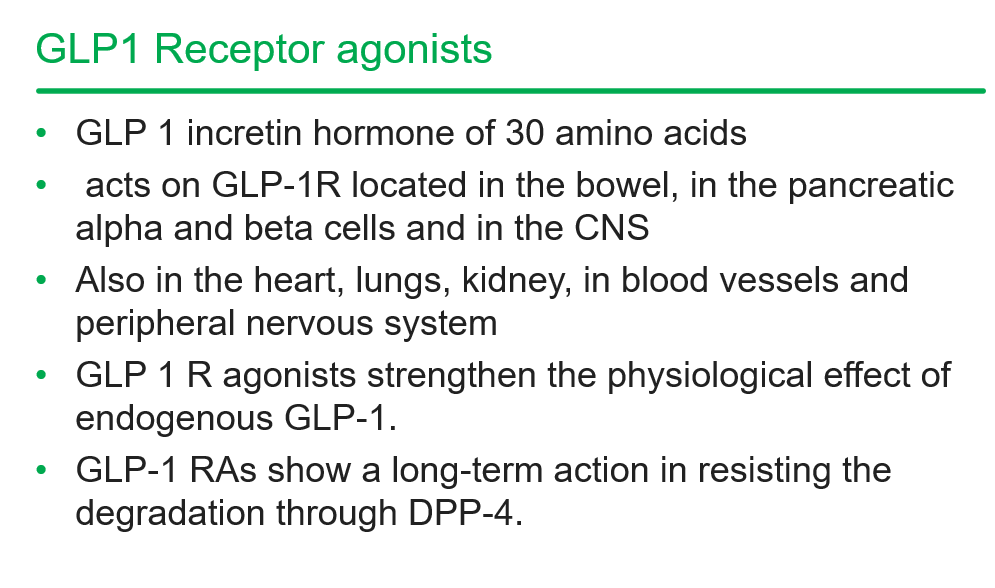
GLP-1 agents are a huge advance but currently limited by affordability (frequently there is a lack of insurance coverage if there is not T2DM) and availability. In addition, most individuals will regain weight loss when these agents are stopped.
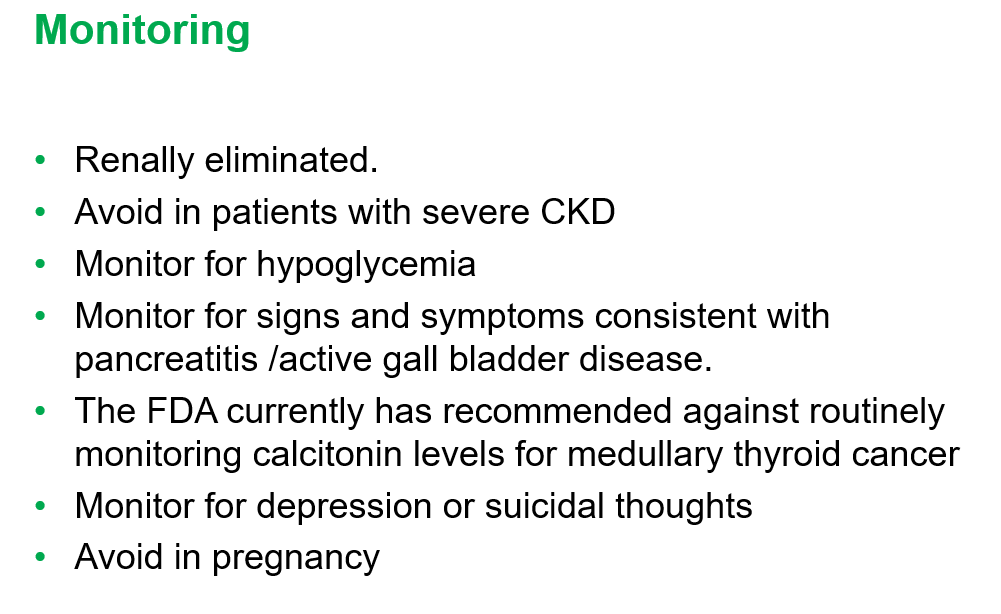
GLP-1 agents are not recommended in the following: patients with gastroparesis, and patients with a personal or family history significant for MEN 2 A /MEN 2 B/ Medullary thyroid cancer
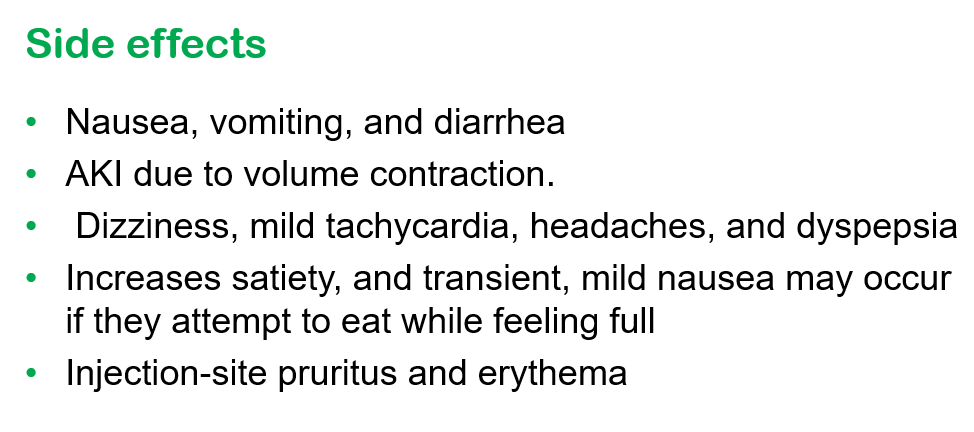
Long-term data is still needed. These agents have been associated with muscle and bone loss; thus, working to assure a good diet is still very important
——————————————————————————
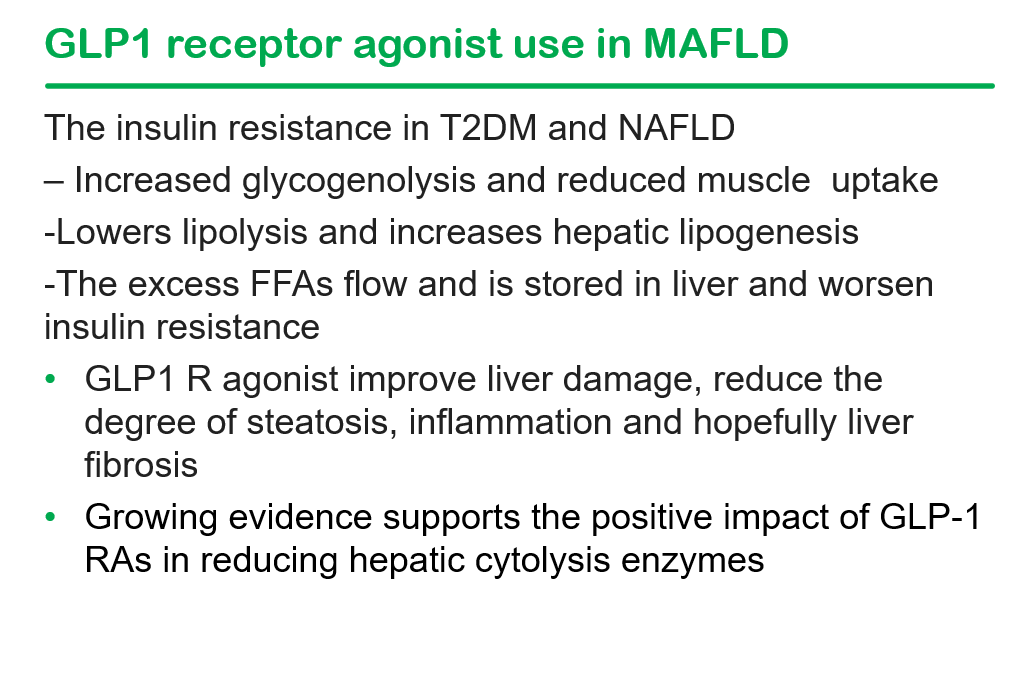
NASPGHAN has a good review/webinar on this topic as well: Pediatric MASLD in the Current Era of Pharmacological and Surgical Obesity Treatment Options. For members, after sign in, you can register and login to this webinar (look under clinical practice tab). This webinar made a lot of useful points (many covered by Dr. Arora too).
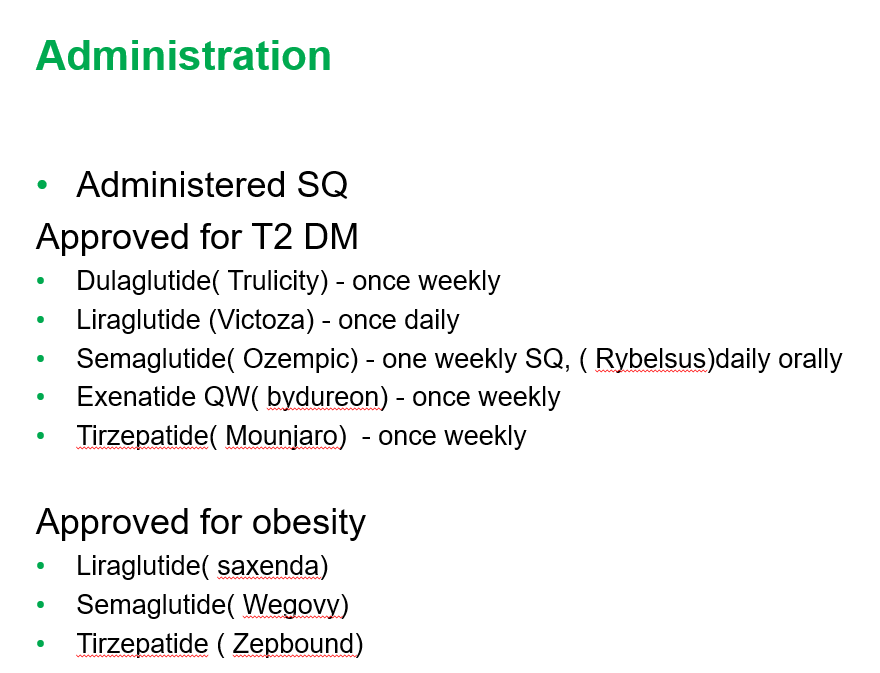
For GLP-1 agents, due to effects on gastric emptying, they are generally held prior to anesthesia. If they are given weekly, then hold 1 week prior to anesthesia. If it is a daily medication, hold for 1 day prior to anesthesia.
Surgery definitely helps improve MASH -though variable responses in patients. SLEEVE gastrectomy is currently the most frequent bariatric surgery
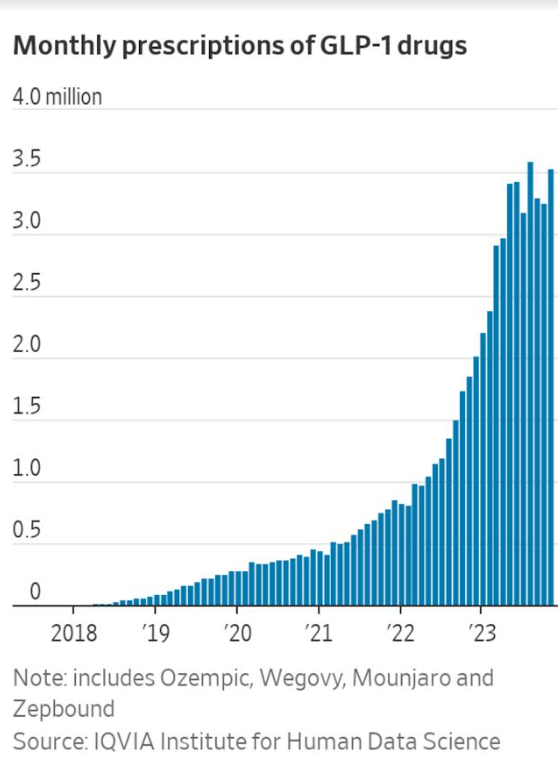
There is trouble getting GLP-1 medications.
Limited knowledge regarding long-term effects of cycling of GLP-1 agents.
Obesity is a long-term disease –>anticipate long-term treatment
The Wall Street Journal recently published a personal account of using the newer obesity medications. Bradley Olson, 1/12/24: A Weight-Loss Drug Changed My Life. Will It Solve My Problem? (behind a paywall). This article discusses the dramatic improvement experienced by the writer along with his concerns about the cost of the medication and potential for rebound when he can no longer afford it. Two of the figures:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
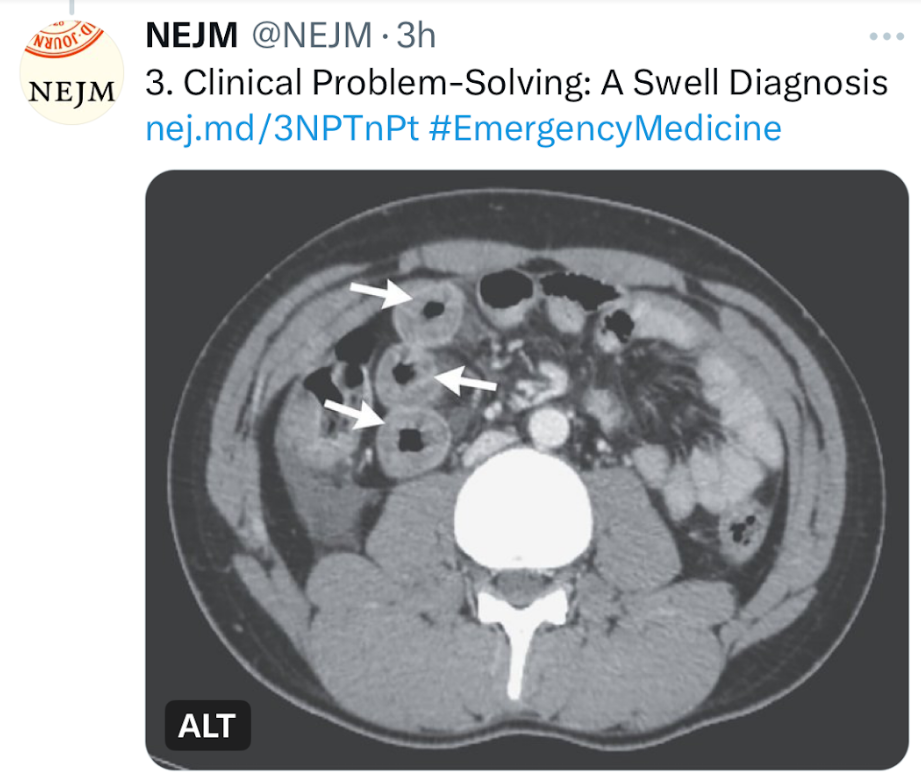
J Allam et al. NEJM 2024; 390-71-76.A Swell Diagnosis
This clinical problem-solving case report describes a previously healthy 19 yo male with sudden-onset severe diffuse abdominal pain. His ED evaluation was unremarkable (including labs [CBC/d, CMP, Lipase, CMP, thryotropin, ESR, CRP and UA], and EKG). He was discharged after 3 hours. Over the next 10 years, he presented to the ED on numerous occasions with the same symptom complex and normal labs/mostly CT scans. One CT scan showed small-bowel thickening thought to be due to AGE. Ultimately, his symptoms increased to every 2 weeks. Extensive evaluations (multiple panendoscopies, MRCP, MRE, U/S, and infectious workup) were undertaken and numerous treatments were given without benefit. Ultimately, a CT scan showed remarkable circumferential wall thickening in the jejunum (see below). This led to evaluation for hereditary angioedema.
The article serves as a good review of this disorder and of the differential diagnosis.
Key points:
Background: Hereditary angioedema, which is due to a deficiency of functional C1 inhibitor protein, is a rare autosomal dominant genetic disorder that affects approximately 1 in 50,000 persons worldwide.1
Mean age of onset : 8 to 12 years, and symptoms often worsen during puberty.1
Presentation: The disease is characterized by recurrent episodes of swelling in various parts of the body and can be severely debilitating. The hallmark symptom of hereditary angioedema is localized swelling of the skin and submucosal tissues (in the face, lips, throat, hands, feet, or genitalia) that is nonpitting, nonpruritic, and not accompanied by urticaria. Triggers include emotional stress, physical trauma, infections, physical exertion, and surgery and other medical procedures.
Abdominal pain: In a series of 149 patients with hereditary angioedema who had 521 attacks, 49% of the episodes were characterized by isolated abdominal pain.5 Abdominal attacks are generally not associated with fever, peritoneal signs, or leukocytosis.
Laryngeal edema occurs in approximately 0.9% of all attacks7 and may be life-threatening, leading to asphyxiation and death.
Differential Diagnosis: Some of the rare diagnosis that were discussed: acute intermittent porphyria, familial Mediterranean fever (FMF), mastocytosis, and eosinophilic gastroenteritis.
Pathophysiology: Deficiency of C1 inhibitor protein: The majority of cases of hereditary angioedema are caused by either decreased levels (type I) or reduced functionality (type II) of C1 inhibitor. A third subtype (type III) that is associated with different mutations but the same clinical features is characterized by normal quantitative and functional C1 inhibitor levels.2
The best screening test: measurement of the level of C4 (which is exhausted as a result of uncontrolled activation of the complement pathway when C1 inhibitor is deficient or dysfunctional); results may be normal in 10% of patients between attacks. Quantification of C1 inhibitor levels can then be performed to differentiate between the low levels in hereditary angioedema type I and the normal levels in hereditary angioedema type II.
Treatment: Food and Drug Administration–approved agents include human plasma–derived C1 inhibitor concentrate, recombinant human C1 inhibitor, icatibant (bradykinin B2 receptor antagonist), and ecallantide (kallikrein inhibitor).9 Each has been shown in randomized, controlled trials to decrease the median time to symptom relief.10-14 The first three therapies may be administered by the patient, whereas ecallantide requires support from a health care professional for management of possible anaphylaxis, which is reported in up to 4% of patients.9 Most treatments are used on-demand, though some patients benefit from long-term prophylaxis.
Preprocedure prophylaxis: Preprocedural prophylaxis is recommended for patients undergoing procedures that may trigger an attack (e.g., dental surgery, endotracheal intubation, or an endoscopic procedure). C1 inhibitor concentrate can be administered intravenously before the procedure, or treatment with an anabolic androgen (e.g., danazol or stanozolol) can be started 5 days before and continued for 2 to 5 days after the procedure9; …Fresh frozen plasma may be used as a second-line therapy when these therapies are not available
My take: This case “highlights the importance of maintaining a high clinical suspicion for hereditary angioedema in patients with episodic severe abdominal pain and negative workup for other illnesses” even in patients without other manifestations.
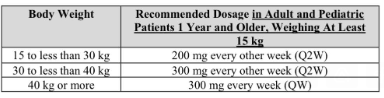
“Regeneron Pharmaceuticals, Inc. (NASDAQ: REGN) and Sanofi today announced that the U.S. Food and Drug Administration (FDA) has approved Dupixent® (dupilumab) for the treatment of pediatric patients aged 1 to 11 years, weighing at least 15 kg, with eosinophilic esophagitis (EoE).”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
After performing a systematic literature review, the authors identified randomized controlled trials (RCTs) recruiting adults with IBS, comparing probiotics with placebo were eligible; this included 82 eligible trials, containing 10,332 patients. However, only 24 RCTs were at low risk of bias across all domains.
Key findings:
There was some evidence to support the use of some probiotics for global IBS symptoms, abdominal pain, and abdominal bloating or distension (highly detailed analysis of the studies in article –Figures 1-3 and Tables 1-3)
There was moderate certainty in the evidence for a benefit of Escherichia strains, low certainty for Lactobacillus strains and L. plantarum 299V, and very low certainty for combination probiotics, LacClean Gold S, Duolac 7s, and Bacillus strains
For abdominal pain, there was low certainty in the evidence for a benefit of S. cerevisiae I-3856 and Bifidobacterium strains, and very low certainty for combination probiotics, Lactobacillus, Saccharomyces, and Bacillus strains
For abdominal bloating or distension, there was very low certainty in the evidence for a benefit of combination probiotics and Bacillus strains
The relative risk of experiencing any adverse event, in 55 trials, including more than 7000 patients, was not significantly higher with probiotics
My take: This study shows that it is difficult to confidently recommend specific probiotics for IBS as the certainty in the evidence for efficacy by GRADE criteria was low to very low. In addition, the quality control of production of most probiotics is uncertain.
The authors retrospectively utilized the University of Manitoba IBD Epidemiology Database includes all Manitobans diagnosed with IBD between 1984 and 2018 (n=5920). Key findings:
Rates of PPI use in control subjects increased gradually from 1.5% to 6.5% over 15 years
Persons with IBD had a higher rate of PPI use, peaking up to 17% within 1 year of IBD diagnosis with a rate ratio (RR) of 3.1
The authors noted an abrupt increase in PPI use within 6 months of an IBD diagnosis which could indicate that IBD-related symptoms are being mistakenly treated with a PPI or that IBD may increase reflux-related symptoms. Given the higher rate of PPI use in pre-IBD diagnosis patients, compared to controls, the authors note that “it is possible that their [PPI] use enhances the likelihood of an IBD diagnosis by their role in altering the gut microbiota.” In addition, they note that “a case-control study found that PPIs were associated with an increased risk of pediatric IBD” (NR Schwartz et al. J Pediatr Pharmacol Ther 2019; 24: 489-496).
My take: PPIs are being used more frequently. Whether PPIs are detrimental before or after a diagnosis with IBD is not clear.