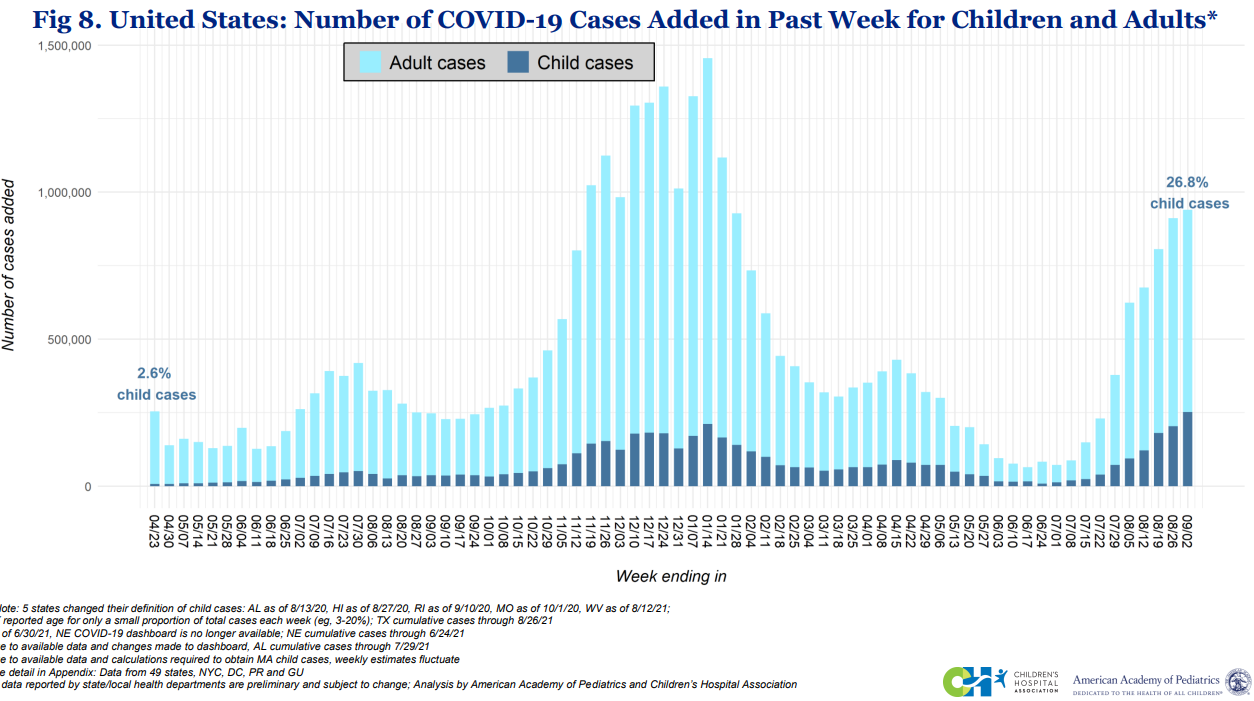
Here is a link to report from AAP and Children’s Hospital Association: Children and COVID-19: State Data Report (37 pages of data)
Situation is most problematic in the South.



Here is a link to report from AAP and Children’s Hospital Association: Children and COVID-19: State Data Report (37 pages of data)
Situation is most problematic in the South.
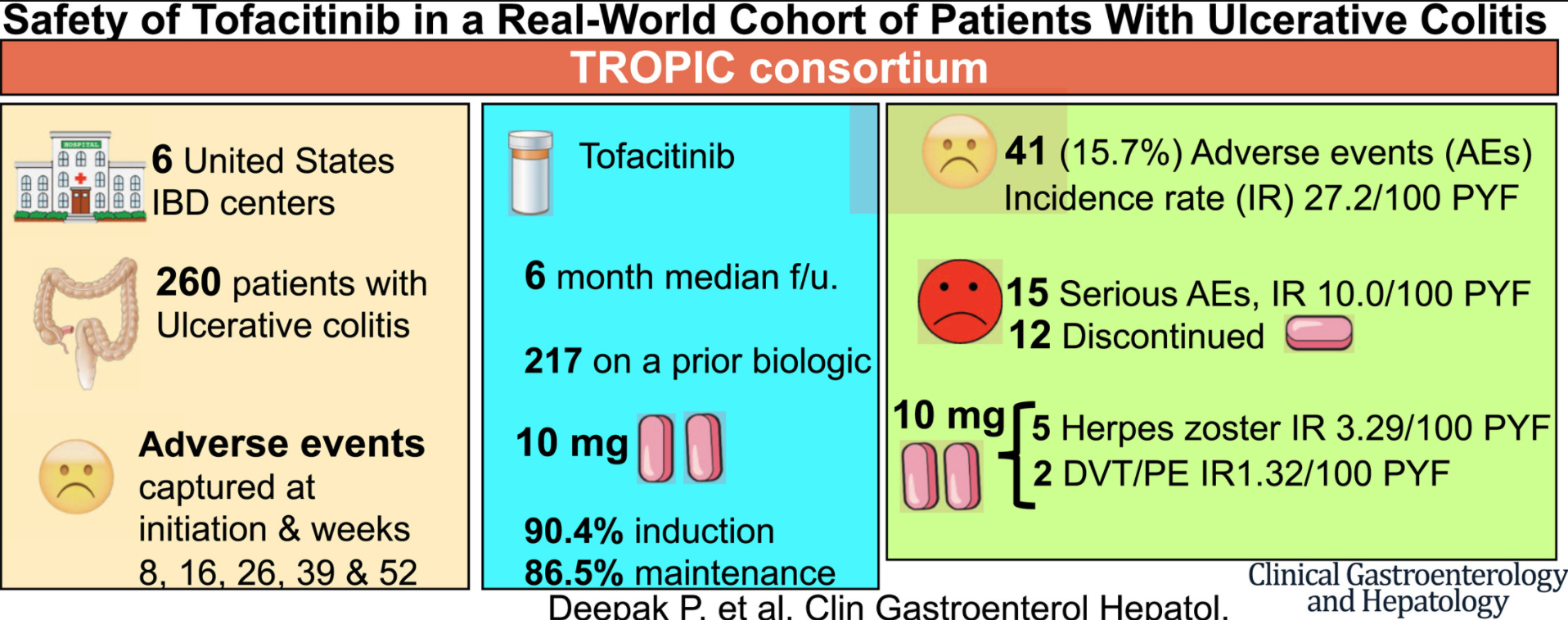
P Deepak et al. Clin Gastroenterol Hepatol 2021; 19: 1592-1601. Full Text: Safety of Tofacitinib in a Real-World Cohort of Patients With Ulcerative Colitis
This study described a ‘real-world’ experience with tofacitinib for Ulcerative Colitis in 260 adults; five patients developed HZ infection and 2 developed VTE (all receiving 10 mg tofacitinib, twice per day).
Related blog posts -Tofacitinib:
JR de Bruyn et al. Clin Gastroenterol Hepatol 2021; 19: 1573-1582. Full Text: High-Dose Vitamin D Does Not Prevent Postoperative Recurrence of Crohn’s Disease in a Randomized Placebo-Controlled Trial
Methods: Patients with CD after ileocolonic resection with ileocolonic anastomosis were assigned randomly to groups given weekly 25,000 IU oral vitamin D (n = 72) or placebo (n = 71) for 26 weeks, at 17 hospitals in The Netherlands and Belgium, from February 2014 through June 2017
Key finding: The cumulative rate of clinical recurrence did not differ significantly between the groups (18.1% in the vitamin D group vs 18.3% in the placebo group; P = .91). Though, the Vit D group achieved higher levels at week 26 (81 vs 43 of 25-OH Vit D)
GP Ramos et al. Inflamm Bowel Dis 2021; 27: 1270-1276. The Impact of Vedolizumab on Pre-Existing Extraintestinal Manifestations of Inflammatory Bowel Disease: A Multicenter Study
Key findings (n=201, retrospective study):
Related blog post: Vedolizumab and Extraintestinal Manifestations of IBD
In an observational prospective longitudinal study of with newly diagnosed Crohn’s disease in 156 adults followed for nearly 1.5 years, Yanai et al found that 52 patients (33.3%) had an indolent course of CD, 29 (18.5%) required hospitalizations, and 75 (48%) were recommended to start steroid, immunomodulator, or biologic therapies. An “indolent course” indicated a lack of needing steroids, immunomodulators, anti-TNF agents, hospitalization or surgery. Key findings:
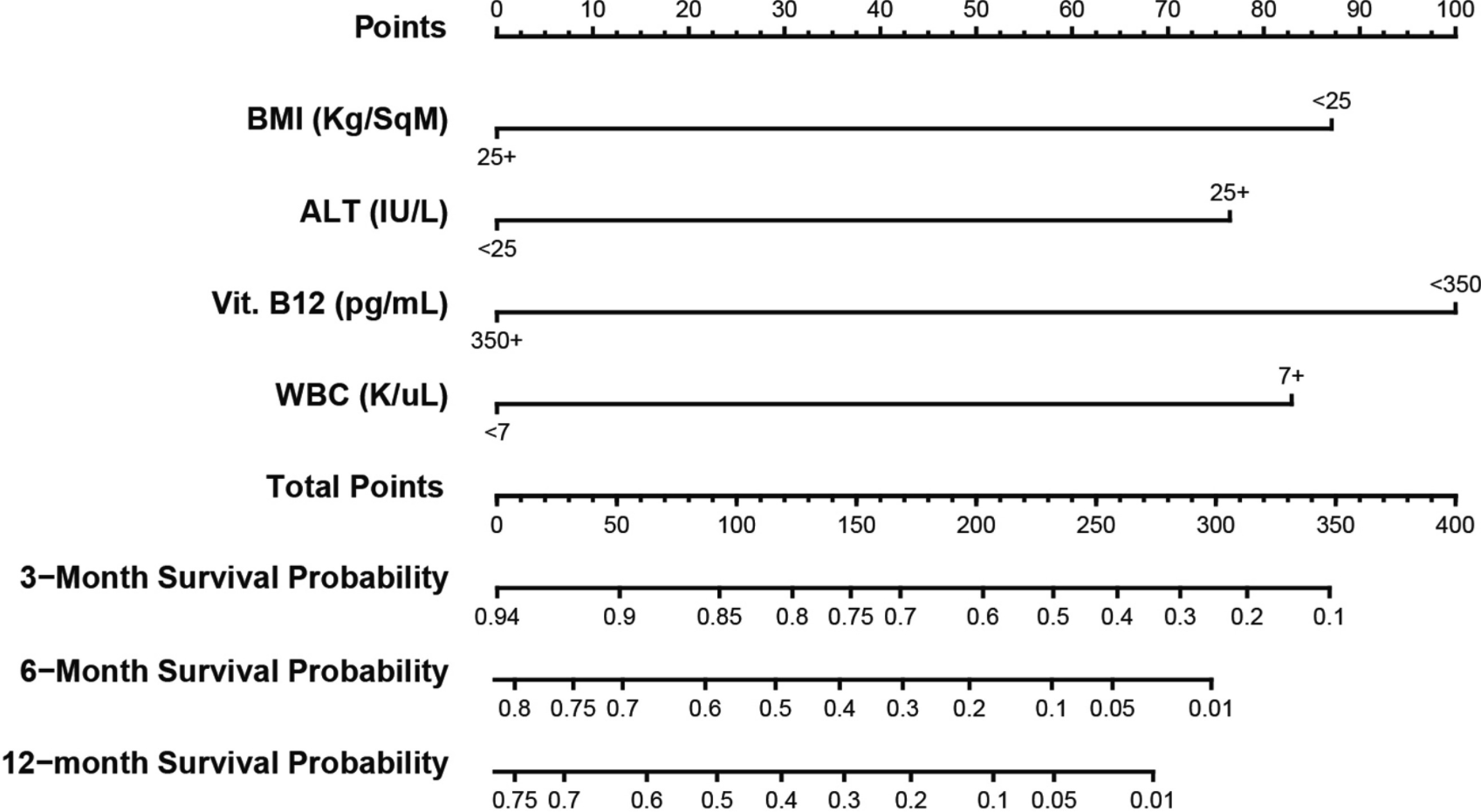
My take: In this study, low BMI, low Vit B12, high wbc, and high ALT were associated with a more complicated course. These particularly risk factors do not seem intuitive to me. These findings need to be looked at in the pediatric age group, which likely has a lower rate of an indolent course.
G Le Baut et al. Clin Gastroenterol Hepatol 2021; 19: 1602-1610. A Scoring System to Determine Patients’ Risk of Colectomy Within 1 Year After Hospital Admission for Acute Severe Ulcerative Colitis
In this retrospective study of 270 consecutive adult patients with acute severe ulcerative colitis (ASUC) (2002-2017), the cumulative risk of colectomy was 12.3% (95% CI, 8.6–16.8). Key findings:
My take: These findings confirm other studies in patients with ulcerative colitis which have shown that each of these criteria were predictors of severe disease.
Related blog posts:
It’s been nearly two years since the start of the NASPGHAN Bowel Sounds Podcast.
They are really good. While I am more of a visual learner, I like listening to the hosts banter at the beginning and then their capable interviews. The Podcasts have chosen terrific guests. You can read about and listen to all of the episodes at the NASPGAN website (link below), or listen on the go on Apple Podcasts, Spotify, Google Podcasts, or wherever else you listen to podcasts.
Here’s the NASPGHAN link: Bowel Sounds: The Pediatric GI Podcast
The two most recent podcasts (Dr. Martin and Dr. Vartabedian) exemplify the wide range of information available.
Dr. Martin Martin reviews the topic of congenital diarrheas and enteropathies (CODEs). Some key points:
Links:
Related blog posts:
Dr. Vartabedian, in his episode, discusses the importance of “owning your online identity as a physician, something “Dr. V” has written and spoken about extensively, including on his blog at 33charts.com” (from NASPGHAN website). He explains that everyone has a presence online and physicians can influence the content. At the very least, most physicians should make sure that their institutional profile looks good and that they take advantage of placing a profile on LinkedIn.
Other key points:
Links:
Related blog posts:

In a nationwide retrospective cohort from The Netherlands (pop. ~17 million), a recent study (RM de Voer et al. Clin Gastroenterol Hepatol 2021; 19: 1642-1651. Full Text: Clinical, Pathology, Genetic, and Molecular Features of Colorectal Tumors in Adolescents and Adults 25 Years or Younger) characterizes the clinical and genetic features of colorectal cancer (CRC) in individuals <26 years of age (aka AYA group) from 2000-2017.
Key findings:
Related blog posts:

NY Times (8/22/21), Sarah Kliff: How to Look Up Prices at Your Hospital, if They Exist
This article describes how to look up hospital prices which is being mandated (by Jan 2022) with new federal regulations. Currently the process is not easy because it is not consumer-friendly.
An excerpt:
Before you start looking for prices, you’ll want to know what kind of health insurance you have — both the name of your insurer and also details like whether you picked an H.M.O. plan during open enrollment or went with a P.P.O. option…
For most hospitals, the data is posted on a page labeled “price transparency.” Many researchers say they begin looking for price files through a search on Google for that phrase and the hospital’s name.
The hospital’s price transparency site will probably have multiple sections and links, and the labeling of the price files isn’t always clear. You’ll want to look for something like a “comprehensive machine-readable file” or “negotiated price list.”
It’s also worth opening up files that are described as containing “standard charges” or a “chargemaster.”
When you open the files, you see it actually has the hospital’s negotiated rates and cash prices, too.
The government has not created a standard format for hospitals to report their price data, and each hospital seems to take a slightly different approach.
Some health care experts say the large data files will become more useful after third-party data companies clean and organize the information, so that patients can search across multiple hospitals and health care services.
One data transparency company, Turquoise Health, has already created a free price lookup tool.
My take: Many hospitals are starting to comply with price transparency requirement; however, it is will be cumbersome and I expect that 3rd parties (like Turquoise Health) will be needed for most people to access this data.
Related blog posts:

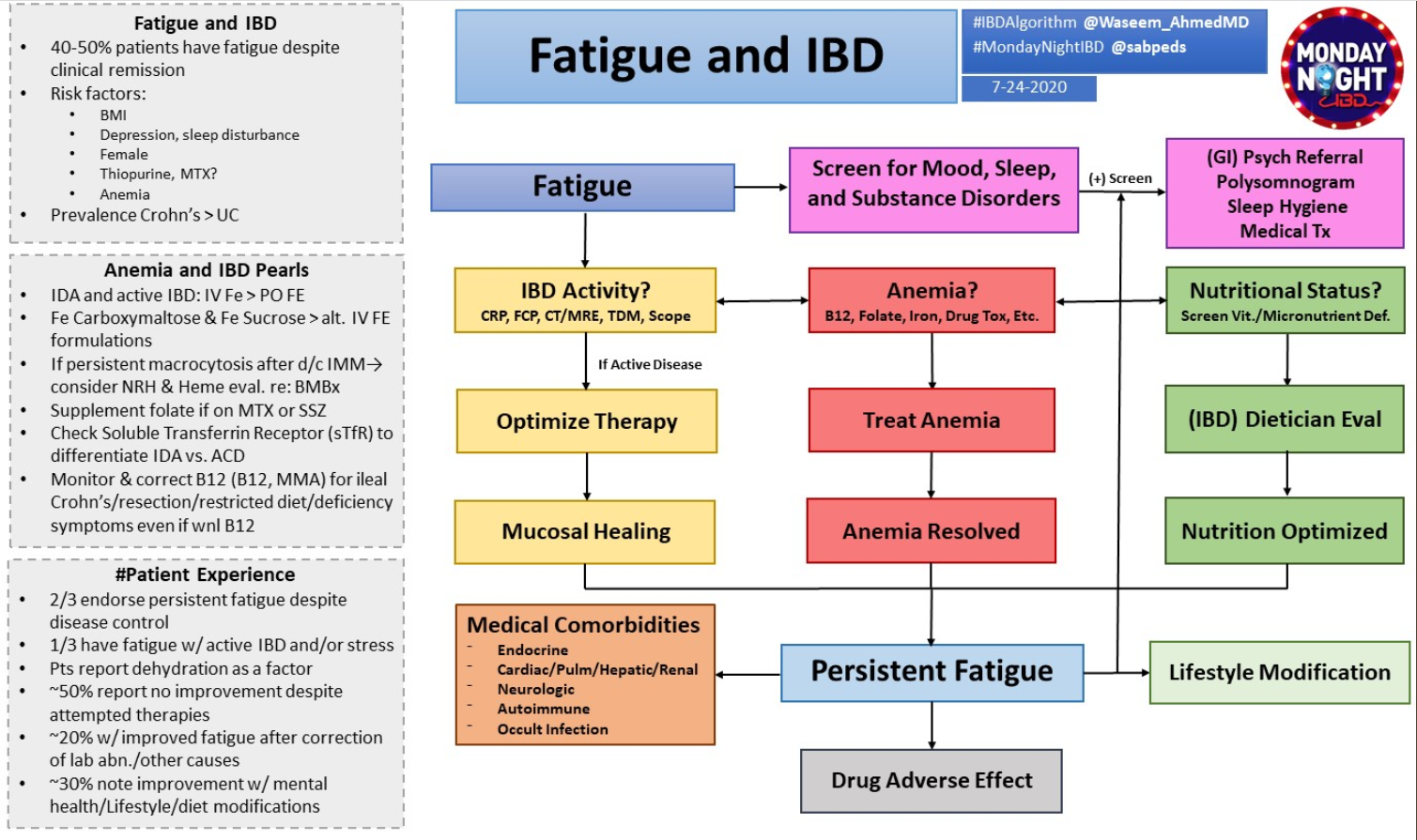
#MondayNightIBD is an open access learning forum on twitter. It was recently highlighted in Gastroenterology and Endoscopy News: A #MondayNightIBD Conversation: Fatigue, a Frustrating, Multifactorial Manifestation of IBD (requires login)
For the issue of fatigue and IBD, besides active IBD and anemia, the authors recommend considering medication side effects (especially from immunomodulators/corticosteroids and cannabis), mental health, sleep disorders, and nutritional concerns (?role for thiamine supplementation). Even when all these issues are addressed, many times fatigue persists.
Here is the proposed algorithm from July 24, 2020.
#MondayNightIBD has a lot of topics that they have covered including functional medicine, COVID, sexual health, utilizing social medicine, grief and pharmacology.
Medpage Today (Sept 1, 2021), Full text: FDA Slaps Restrictions on JAK Inhibitors Over Serious Safety Risks
— Use for inflammatory conditions limited to those who fail on TNF blockers
An excerpt:
The FDA has finished its review of a large postmarketing safety study of tofacitinib (Xeljanz, Xeljanz XR), and its conclusions do not bode well for the popular drug and the larger class of JAK inhibitors.
Data from the trial revealed increased risks for serious heart-related events — including myocardial infarction (MI) and stroke — as well as a higher risk for cancer, blood clots, and death. Even the lower 5-mg dose of tofacitinib turned up an increased risk of blood clots and death in the final analysis, the agency noted.
FDA is requiring new and updated warnings for tofacitinib, as well as two other arthritis medicines in the JAK inhibitor class — baricitinib (Olumiant) and upadacitinib (Rinvoq)…
Treatment with the JAK inhibitor was associated with an increased risk for major adverse cardiac events (MACE), including MI, cardiovascular death, and stroke (HR 1.33, 95% CI 0.91-1.94), which missed criteria for non-inferiority, as well as a higher risk for cancer (HR 1.48, 95% CI 1.04-2.09).
Related blog posts -Tofacitinib:

Here’s a link: AGA says stay the course, despite the Delta variant
An excerpt:
“AGA suggests against re-instituting routine pre-procedure testing prior to elective endoscopy. The downsides (delays in patient care, burden, inaccurate results) outweigh potential benefits. Infection and transmission of SARS-CoV2 from asymptomatic individuals is rare especially among vaccinated health care workers using personal protective equipment (PPE), even with the emergence of the Delta variant.”
“If PPE is available, AGA recommends using N95 masks” for both upper endoscopy and colonoscopy”
M Ghisa et al. Clin Gastroenterol Hepatol 2021; 19: 1554-1563. Achalasia and Obstructive Motor Disorders Are Not Uncommon in Patients With Eosinophilic Esophagitis
In this study with 109 adults who were newly diagnosed with eosinophilic esophagitis (EoE), the authors consecutively performed high-resolution manometry (HRM). Key findings:
These findings are important because the diagnosis of EoE could result in a diagnostic delay of concurring achalasia and because the presence of esophageal eosinophilia could perhaps play a role in the pathogenesis of achalasia (or vice versa). The finding of achalasia in 7.3% of this population is exponentially higher than the estimated prevalence of achalasia in the general population (10-16 cases per 100,000).
My take: In patients with EoE, further diagnostic workup is indicated if there are persistent symptoms.
Related blog posts:

