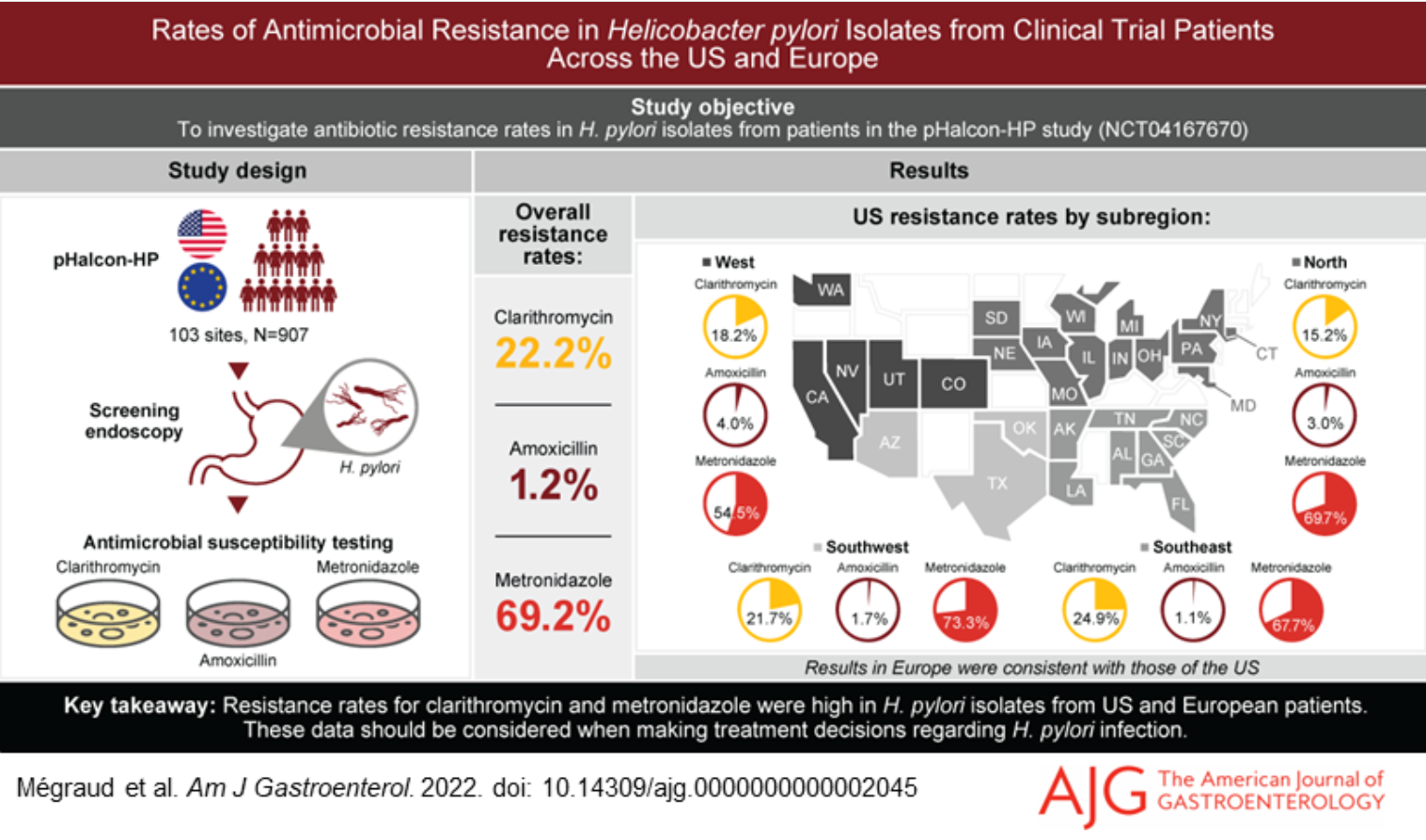
F Megraud et al. AJG 2022; doi: 10.14309/ajg.0000000000002045 Open Access: Rates of Antimicrobial Resistance in Helicobacter pylori Isolates From Clinical Trial Patients Across the US and Europe. Resistance rates were established in isolates from 907 participants. Overall, 22.2% were resistant to clarithromycin, 1.2% to amoxicillin, and 69.2% to metronidazole.
O Atia et al. Lancet Gastroenterol Hepatol 2022; DOI:https://doi.org/10.1016/S2468-1253(22)00307-7. Outcomes, dosing, and predictors of vedolizumab treatment in children with inflammatory bowel disease (VEDOKIDS): a prospective, multicentre cohort study
Methods: VEDOKIDS was a paediatric, multicentre, prospective cohort study done in 17 centres in six countries. We report the 14-week outcomes as the first analyses of the planned 3-year follow-up of the VEDOKIDS cohort
Key findings:
- 32 (42%) of 77 children with ulcerative colitis and 21 (32%) of 65 children with Crohn’s disease were in steroid-free and exclusive enteral nutrition-free remission at 14 weeks.
- In children who weighed less than 30 kg, the optimal drug concentration associated with steroid-free and exclusive enteral nutrition-free clinical remission was 7 μg/mL at week 14, corresponding to a dose of 200 mg/m2 body surface area or 10 mg/kg

USAToday 11/14/22: More teens are getting weight loss surgery but some experts think more needs to be done
And of course, an important story from The Onion: Arsonist Worried He Forgot To Turn Stove On Before Leaving House

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.