A recent study (below) reminded me of a joke. First the joke (better with the visual effect):
A guy goes to his doctor. The patient says, “Doctor when I touch here on my shoulder (with index finger) it hurts, when I touch here on my leg (with index finger) it hurts, and when I touch here on my stomach (with index finger) it hurts.”
In this cross-sectional study of 7-17 year olds (n=406) with Rome III functional abdominal pain disorder (FAPD), the authors examined the frequency of pain outside GI tract over a 2 week study period. Patients were recruited from both a large academic pediatric GI practice and general pediatric offices in same hospital system.
Key findings:
In total, 295 (73%) children endorsed at least 1 co-occurring nonabdominal pain, thus, were categorized as having multisite pain with the following symptoms: 172 (42%) headaches, 143 (35%) chest pain, 134 (33%) muscle soreness, 110 (27%) back pain, 94 (23%) joint pain, and 87 (21%) extremity (arms and legs) pain
In addition, 200 children (49%) endorsed 2 or more nonabdominal pain symptoms
Participants with (vs without) multisite pain had significantly higher abdominal pain frequency (P < .001) and severity (P = .03), anxiety (P < .001), and depression (P < .001). Similarly, children with multisite pain (vs without) had significantly worse functional disability (P < .001) and health-related quality of life scores (P < .001).
The authors note that due to the design of their study, they cannot establish a causal association between pain symptoms and psychosocial functioning.
My take: A lot of kids with stomach pain have multisite pain as well as anxiety and depression. This study reminds us to ask about them.
In this retrospective study of 65 healthy infants (<3 months of age, median age 2 months) who had CT scans performed due to trauma, the authors investigated the frequency of a fatty liver.
Key findings:
Depending on the criteria used, 23% or 26% of infants had evidence of fatty liver on CT scan
The prevalence of maternal obesity and/or diabetes was 11% (of the 65 pregnancies) but there was no significant difference in maternal risk factors between infants with and without evidence of steatosis
My take: Whether the fatty liver seen on CT scans in this infant cohort persists and evolves to adolescent and adult fatty liver disease is unknown but intriguing.
“According to the study in Pediatrics, one of every 168 American Indian/Alaska Native children, one of every 310 Black children, one of every 412 Hispanic children, and one of every 612 Asian children have lost a caregiver, compared to one in 753 white children.”
This study which encompassed 397,395 total serum bilirubins provides an updated normogram for serum bilirubins in the first days of life. The data for this nomogram is based on 140 times the number of subjects and is derived from 15 years of universal bilirubin screening (Intermountain Healthcare Hospitals).
Key points:
The authors state that this study is one step “toward evidence-based phototherapy decision-making”
“We are currently using this nomogram [figure below] routinely in our hospitals in Utah for phototherapy initiation (when a neonate has a TSB exceeding the 95th percentile) and for discharge risk stratification.”
“This reduces phototherapy usage…to about 5% of well babies, whereas we had previously been administering phototherapy in 8-10% of well babies.”
“Newborns with TSB>75 percentile…receive a recommendation for follow-up within 24 hours.”
The authors acknowledge the limitations of their study and caution that more long term outcome data are needed in evaluation of their approach.
My take: Overall, the data is fairly similar to prior data but adoption of these slightly higher values would likely reduce the number of infants requiring phototherapy.
This huge collaborative study with 130 patients provides a great deal of information about familial intrahepatic cholestasis type 1 (FIC1). Key findings:
Survival analysis showed an overall native liver survival (NLS) of 44% at age 18 years. NLS was comparable among FIC1-A, FIC1-B, and FIC1-C (% NLS at age 10 years: 67%, 41%, and 59%, respectively; P = 0.12)
The number of predicted protein truncating mutations did not correlate with natural history or prognosis
In this study, the researchers 834 patients with CHB previously treated with TDF for ≥12 months who were switched to TAF in routine practice at 13 US and Asian center. Key findings:
“Overall, we observed continued improvement in virologic response, ALT normalization, and no significant changes in eGFR following switch to TAF from TDF.”
HBV DNA suppression increased from 88% to 92% at 48 weeks post-switch, and then 95% at 96 weeks postswitch
Improved renal function: “By week 96, 21% (55/267) of patients with CKD stage 2 at switch improved to stage 1 and 35% (30/85) of CKD stage 3-5 patients improved to stage 2 and 1.2% (1/85) to stage 1.”
This practice guidance (with 276 references) is an update from similar guidelines published in 2012.
Key Points For Children:
Children with cirrhosis and ascites should be referred for evaluation for LT
Children undergoing LVP should receive 25% albumin infusion of 0.5-1.0 g/kg, or 6-8 g per liter of ascites removed.
Diagnostic paracentesis should be performed in children with ascites and fever, abdominal pain, or clinical deterioration. The risks and benefits of this procedure for use in all children with new ascites but without these symptoms have not been defined.
Design: 2016-2020: paediatric gastroenterologists prospectively replied to the international Safety Registry, monthly indicating whether they had observed a VTE case in a patient <19 years with IBD. n=24,802 PIBD patients
Key findings:
Twenty cases of VTE were identified (30% Crohn’s disease)
The VTE incidence was 3.72 [95%CI 2.27 – 5.74] per 10,000 person-years, 14-fold higher than in the general pediatric population (0.27 [95%CI 0.18-0.38], p<0.001)
All but one patient had active IBD, 45% were using steroids and 45% hospitalized.
Cerebral sinus venous thrombosis was most frequently reported (50%) VTE
My take: The absolute risk of VTE is low in the pediatric population. In those with active disease, the presence of CVC and use of steroids are known risk factors and require consideration of, at minimum, nonpharmacologic interventions.
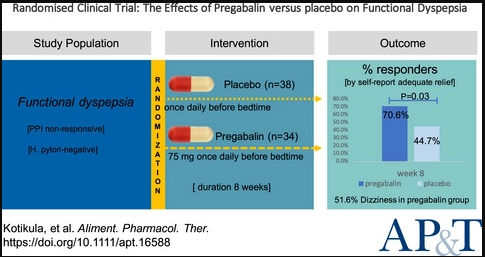
The self-reported adequate relief rates in the pregabalin and placebo groups were 70.6% and 42.1% at week 4 (P = 0.02), and 70.6% and 44.7% at week 8 (P = 0.03), respectively
Pregabalin improved the overall quality of life (P = 0.03)
The most common adverse event with pregabalin was dizziness, occurring in 51.6% of patients
My take: In this study, pregabalin led to significant alleviation of dyspeptic symptoms, especially in patients with predominant epigastric pain.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
While pediatric gastroenterologists typically are not coordinating the management pediatric patients with Type 2 Diabetes Mellitus (T2DM), we certainly see many with T2DM and often are involved in some aspects of their care (eg. fatty liver disease).
This “TODAY2” study annually followed 500 participants from the TODAY trial (2011). The age of the participants was 26.4±2.8 years, and the mean time since the diagnosis of diabetes was 13.3±1.8 years.
Key definitions:
Hypertension: At 95% or greater for age (at least SBP 130 or DBP 80) on 3 consecutive visits and/or needing medical therapy
Dyslipidemia: Consecutive LDL values of at least 130, consecutive triglycerides of at least 150, or values requiring medical therapy
Albuminuria: ratio of urine albumin to creatinine of at least 30
Diabetic Nerve Disease: based on scores of Michigan Neuropathy Screening Instrument -consecutive values of at least 2 or more (scores range from 0 to 8)
Diabetic Eye Disease: based on a grade of at least 20 according to criteria of Early Treatment Diabetic Retinopathy Study criteria (grades range from 10 to 85)
Key findings:
The cumulative incidence of hypertension: 67.5%
The incidence of dyslipidemia: 51.6%
The incidence of diabetic kidney disease:54.8%
The incidence of nerve disease: 32.4%.
The prevalence of retinal disease: 13.7% (2010 to 2011) and 51.0% (2017 to 2018)
The authors note that the high incidence of complications is “most likely related to extreme metabolic phenotype (which includes severe insulin resistance and rapid worsening of beta-cell function) and to challenging socioeconomic circumstances.”
Study strengths: 15 years of prospective, extensive data and population representative of U.S.
My take: “Taken together, these data illustrate the serious personal and public health consequences of youth-onset” T2DM by age 26 years!! Unless medical therapies improve further, these consequences argue for careful consideration of bariatric surgery.
After expending a great deal of time and effort on prior authorizations lately, this recent satirical explanation on prior authorizations and the purpose of insurance companies hits the target. Though, insurance companies do make money off interest, I think the main goal of PA is to limit care costs. Some patients will not get the care their doctor recommends due to stalling by the insurance company. Many times it takes a physician hours in order to get approvals. If a patient’s physician is not willing to do this, many times the patient will not get the treatment.