In a recent commentary (K Grumbach et al. NEJM 2021; 385: 1156-8. Revitalizing the U.S. Primary Care Infrastructure), it’s clear a day of reckoning is coming due to a depletion of primary care physicians.
Scope of the problem:
“High-quality primary care is vital but undersupported in the United States. In communities with more primary care resources, people live longer, health care costs are lower, and there is greater health equity”
“Primary care physicians make up only 30% of the physician workforce…research on primary care garners just 1% of federal agency research awards”
“Primary care physicians earn 30% less than other physicians, on average, and they have among the highest rates of physician burnout”
“The situation is worsening…between 2005 and 2015, the number of primary care physicians in the United States decreased from 46.4 to 41.4 per 100,000 people, and the proportion of nurse practitioners and physician assistants who work in primary care is dropping”
Currently, the number of physician training to become family physicians is “well below the level needed to replace retiring family physicians. Less than one in five internal medicine residency graduates pursue careers in primary care, down from half of such graduates 25 years ago”
The authors propose a government council to develop and implement a plan to address the looming crisis.
My take: Virtually nothing has been done in 25 years to address this problem and I doubt anything substantive will emerge in the near future; though, it would be good policy to incentivize more physicians to go into primary care.
“Issue-attention cycle” problem. “This pattern occurs when initial public alarm over the discovery of a problem and optimism about its quick resolution are replaced by the realization that solving the problem will require some public sacrifice and will displace powerful societal interests.”from Weight of the Nation | gutsandgrowth
National Cathedral, Washington D.C. Scaffolding due to earthquake damage in 2011.
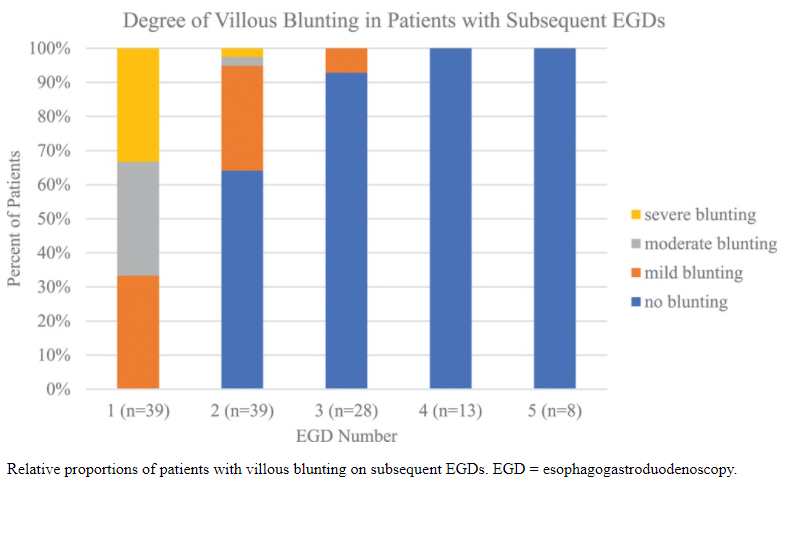
Background: “Current standard of care in the management of uncomplicated CD is not to undergo multiple esophagogastroduodenoscopies (EGDs)… In this study, patients with both CD and eosinophilic gastrointestinal disorders (EGID) …) were identified to explore [the mucosal response to a gluten-free diet], as it is standard for patients with EGID to undergo repeat EGDs for disease surveillance.”
Key findings in this retrospective study from CHOP:
At second biopsy, 44% (17/39) of patients showed no histologic evidence of active CD and 36% (14/39) of patients had negative tTG-IgA values
9/15 (60%) of patients with no evidence of CD on biopsy had abnormal tTG-IgA levels
8/14 (57%) of patients with normal tTG-IgA levels had evidence of active disease on biopsy
Among the 18 who had been on a GFD for at least 2 years, 94% (17/18) had normal duodenal biopsies after 2 years, and 83% (15/18) had normal tTG-IgA values after 2 years
Of the patients with elevated tTG-IgA and normal duodenal biopsies, 66% (6/9) had inflammation elsewhere in the upper gastrointestinal tract, including 4 patients with active EOE and 2 patients with gastritis
My take: This study confirms that tTG-IgA levels are not optimal for monitoring. Current guidelines recognize this and recommend repeat biopsy in patients with persistent or relapsing symptoms even with negative serology
In this retrospective review (1998-2018), the authors identified 39 patients with esophageal Crohn disease (ECD) who met inclusion criteria.
Key findings:
35 (92%) had a clinical response to treatment and 21 (55%) went into clinical remission
ECD seems to be associated with more disabling intestinal CD phenotypes. Of the 39 patients, 10 (26%) had stricturing phenotype and 21 (54%) had penetrating phenotype; 19 (49%) had perianal disease
“Initial treatment after diagnosis with anti-TNFalpha agents compared to other biologics was associated with greater improvement in clinical (97% vs 71%; P=0.02) and endoscopic response (95% vs. 40%; P<0.01) and in clinical remission (64.5% vs. 14.2%; P=0.01).”
Initial treatment with an anti-TNFalpha agent was initial treatment in 18 patients with ECD; 14 had an inflammatory, 3 had a stricturing, and 1 had a fistulizing phenotype.
While this study showed better response to anti-TNFalpha agents compared to other biologics (eg. anti-IL-12/IL-23 agents), this may be due to a selection bias as other biologics are often used as a second-line treatment and are selected more often in refractory disease.
My take: Esophageal Crohn’s disease is a rare diagnosis and appears associated with more severe disease.
Chesapeake and Ohio Canal National Historic Park (near Washington D.C.)
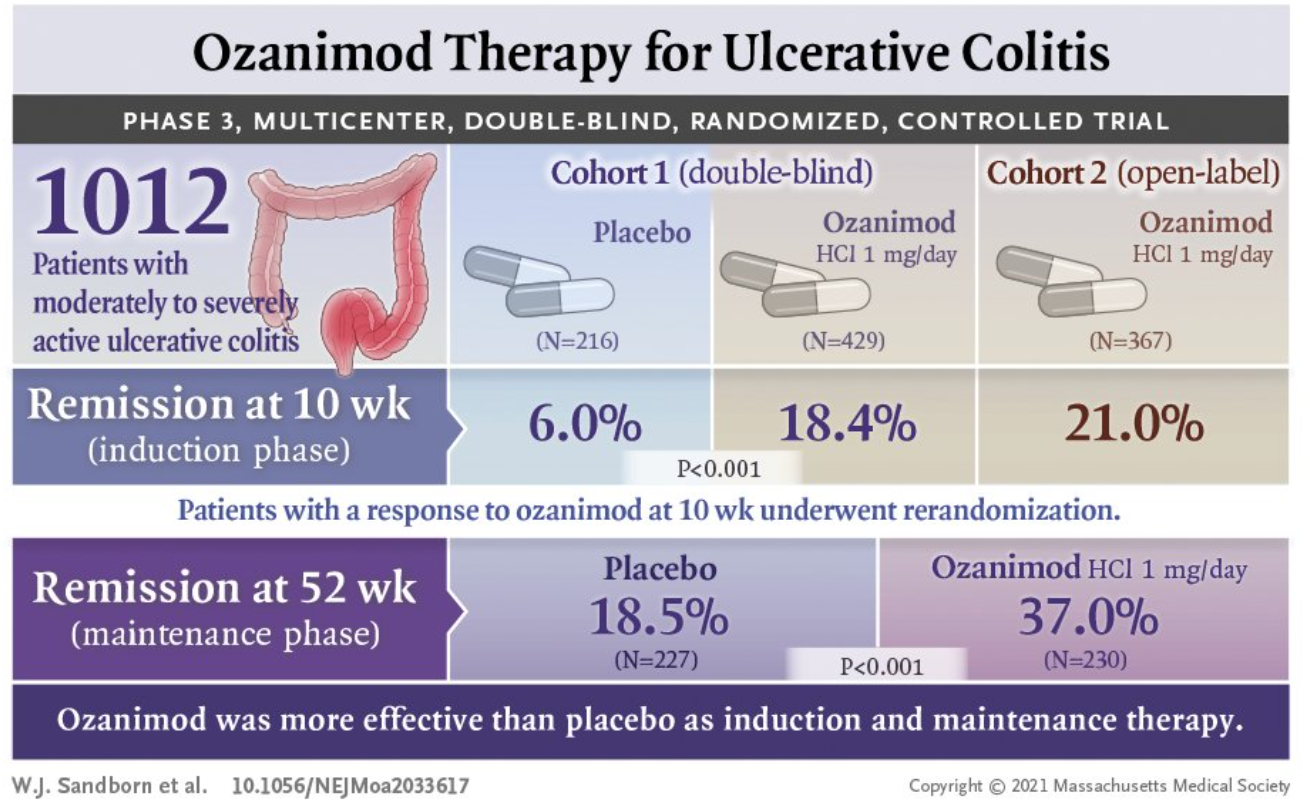
Mechanism of Action: Ozanimod is a selective sphingosine-1-phosphate receptor modulator which leads to internalization of S1P1 receptors in lymphocytes and the prevention of lymphocyte mobilization to inflammatory sites.
Design: There were two initial cohorts of adults with moderately to severely active ulcerative colitis. The first cohort (n=645) of this 52-week multicenter, randomized, double-blind, placebo-controlled trial (285 sites, 30 countries) of ozanimod as induction and maintenance therapy received either 1 mg of ozanimod hydrochloride once a day or placebo. A second cohort (n=457) received open-label ozanimod and was designed to assure that there would be adequate numbers of patients for the maintenance phase. The design allowed up to 30% of the first cohort to have received prior anti-TNF therapy and up to 50% of the second cohort to have received prior anti-TNF therapy. Ozanimod-treated patients with a clinical response during the 10-week induction were randomized again to a treatment group (n=230) or a placebo group for maintenance (n=227). Placebo-treated patients with a clinical response continued to receive placebo.
Approximately 97% of both cohorts had received prior aminosalicylate treatment and ~20% had received prior vedolizumab therapy.
As a safety measure (due to concerns of bradycardia), there was a 7-day period at the start of treatment with dose escalation, starting at 0.25 mg on days 1-4, 0.5 mg on days 5-7, then to 1 mg thereafter.
Key findings:
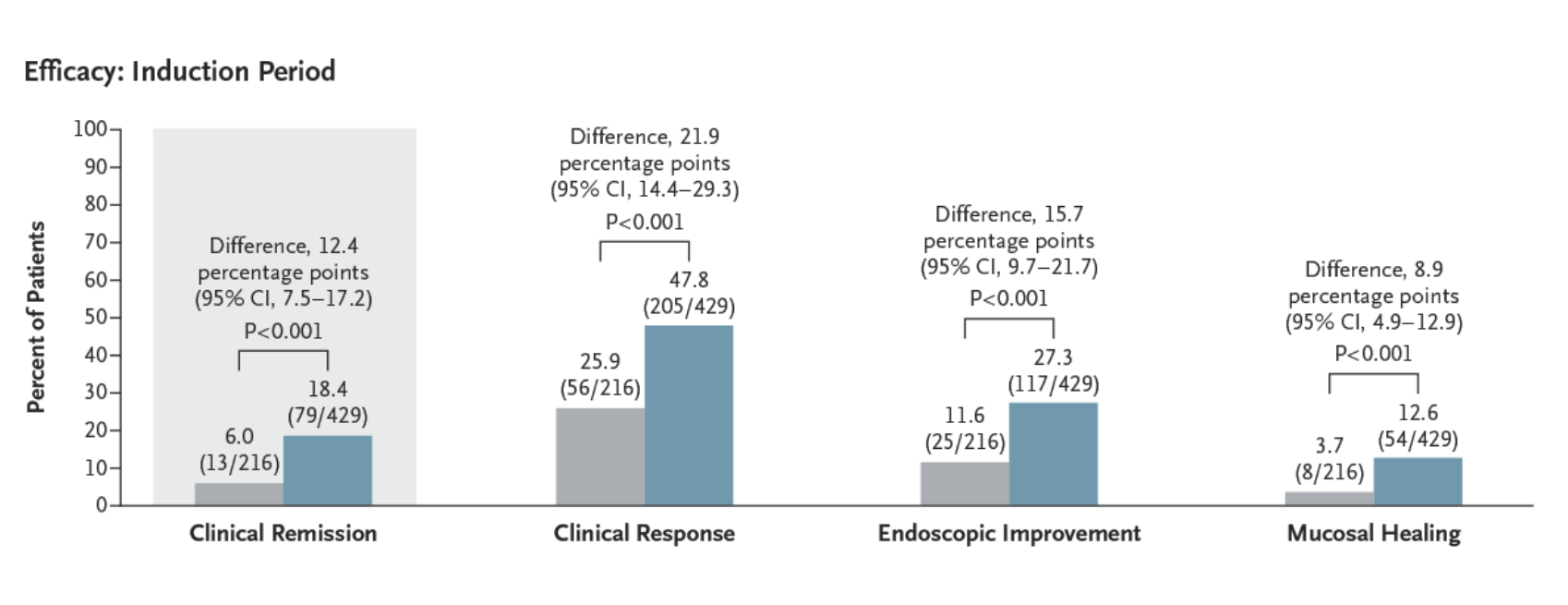
The incidence of clinical remission was significantly higher among patients who received ozanimod than among those who received placebo during both induction (18.4% vs. 6.0%, P<0.001) and maintenance (37.0% vs. 18.5% [among patients with a response at week 10], P<0.001).
The incidence of clinical response was also significantly higher with ozanimod than with placebo during induction (47.8% vs. 25.9%, P<0.001) and maintenance (60.0% vs. 41.0%, P<0.001).
Histologic remission during induction, ozanimod vs placebo: 15.% vs 5.8%.
A post hoc analysis showed decreases in the rectal-bleeding and stool-frequency subscores by week 2 (1 week after the completion of dose adjustment).
From NEJM Twitter Feed
Safety Concerns:
Serious adverse events attributed to ozanimod or placebo occurred in 4 (0.5%) and 2 (0.9%) during induction respectively and none and 1 (0.4%) respectively during maintenance.
Overall alladverse events during induction occurred in 40% of ozanimod-treated patients and 38% of placebo recipients; during maintenance, adverse events were 49% and 37% respectively.
Absolute lymphocyte count (ALC) decreased by a mean of ~54% from baseline to week 10 in ozanimod-treated patients; ALC was <200 in 1.1% (both cohorts) in induction and 17 patients during maintenance. None of the patients with ALC <200 experienced a serious or opportunistic infection.
Serious infections associated wtih ozanimod or placebo occurred in 10 (1.3%) and 1 (0.5%) during induction respectively and 2 (0.9%) and 4 (1.8%%) respectively during maintenance.
Common infections like nasopharyngitis and upper respiratory tract infections in 3-4% of ozanimod-treated patients compared to ~2% of placebo-treated patients
Cancer: during induction there was one ozanimod-treated patient who had a basal cell carcinoma and during maintenance there was one ozanimod-treated patient who had a basal cell carcinoma. In the placebo group, during maintenance there was one patient who developed adenocarcinoma of the colon and one who developed breast cancer.
Among ozanimod-treated patients, bradycardia was evident in 5 (~0.6%) during induction and none during maintenance. (Patients with significant cardiovascular history were excluded from trial)
Among ozanimod-treated patients, hypertension occurred in 13 (~1.6%) during induction and 4 (1.7%); in the placebo group, none in the induction period and three (1.3%) in the maintenance had hypertension.
Prior to entry, the trial required documented varicella zoster IgG antibody or completion of vaccination. Still, HSV occurred in 3 during induction (~0.5%) and 5 (2.2%) during maintenance (only 1 placebo patient (0.4%) had an HSV infection during maintenance.
Elevated liver tests associated wtih ozanimod or placebo occurred in 42 (5.3%) and 2 (0.9%) during induction respectively and 32 (13.9%) and 1 (5.3%%) respectively during maintenance.
Macular edema was noted in 2 ozanimod-treated patients during induction and 1 during maintenance.
My take: This study shows that ozanimod was more effective than placebo in adults with moderately to severely active ulcerative colitis. It will probably be years before we have adequate pediatric data.
MM Mello, WE Parmet. NEJM 2021; 385: 1153-5. Open Access: Public Health Law after Covid-19 This commentary describes changes in public health law as a result of the COVID-19 pandemic.
Key points:
“More than 1000 suits challenged orders shuttering businesses, banning indoor worship services, restricting travel, and mandating mask wearing.”
“In 1905 in Jacobson v Massachusetts, the Supreme Court upheld a vaccination mandate…Judicial review, the Court found is limited to …’arbitrary and oppressive in particular cases”
“Most courts..have …granted considerable deference to health officials…Courts have been more receptive, however, to challenges relating to religious liberty and the scope of executive authority.”
“The court in an unsigned opinion ruled that the CDC had overstepped its authority [with an eviction ban] under the Public Health Service Act (PHSA)…Congress…must pass legislation to impose one or to clarify that the CDC may impose one.”
“The decisions with regard to free exercise of religion suggest that health orders will face strict scrutiny if they regulate religious practices more strictly than any secular activity that courts deem similar.”
My take: This article makes clear that “while emergencies can lead to abuses of authority, …in their [Courts] zeal to protect religious liberty and constrain executive action, courts may be leaving officials with fewer tools to fight Covid-19 and the next pandemic.”
Mr. Ayer was a U.S. attorney and principal deputy solicitor general in the Reagan administration and deputy attorney general in the George H.W. Bush administration.
An excerpt:
[The Supreme Court’s] recent history suggests that it lacks a majority of justices with sufficient concern about the basic continuity and integrity of the law or the ability of government to function…it seems ready to cast aside certain constitutional rights, the court today regularly gives sweeping new interpretations to other rightsand invokes them to radically narrow certain government powers that were until quite recently uncontroversial, including, for example, powers related to public safety or our democratic process...
Perhaps most unexpected and disturbing were decisions elevating rights of religious assembly over local public-safety rules related to Covid-19 that limited the ability to gather. Yet throughout our history, in matters of public health, the powers of local government have usually been at their apex. That did not matter here — nor did the fact that Chief Justice Roberts was among the dissenters.
“Major changes to the Georgia WIC Program effective today, announced by the @GaDPH & @GAChapterAAP, most importantly, a new WIC Request for Medical Formulas & Supplemental Foods (RMF) form replacing the MDF.”
I want to recognize Dr. Bess Schoen. Bess is a colleague at Emory. I met her when I was a 4th year medical student. Since we work at different hospitals, I do not see her often but greatly respect her and her work.
From one of my colleagues, Tanya Hofmekler:
This month, we are celebrating Dr. Bess Schoen’s retirement and her long career in academic medicine. She will be greatly missed. Dr. Schoen has always modeled the best characteristics of a well-rounded academic physician. On top of those, she is smart, an excellent teacher and is an overall wonderful person. She has trained and impacted many residents and fellows that have passed through Emory. Her trainees walk away with practical medical knowledge and an example of compassionate care. As one of her trainees, I find myself from time to time asking: “What would Dr. Schoen do?”
Dr. Schoen has also dedicated herself to improve the care of pediatric patients with Inflammatory Bowel Disease through her leadership of Improve Care Now at Emory. This year, she will be honored by the Crohn’s and Colitis Foundation of America for her commitment and passion.
This first-hand account of the challenges of IBD care for black patients comes from the first IBD specialist recruited to Grady Hospital (Atlanta) which has a predominantly Black patient population.
Key points:
“The clinical, endoscopic, and histologic end points…on treatment in this patient population are all largely unknown…Black people account for 13% of the U.S. population but only 1% of the patients in nearly 200 outcome-based IBD studies [and] less than 5% of the patients participating in clinical trials of IBD therapeutics.” This is important as “we just do not know how they work for Black people.” Treatment response could be much worse (author notes that prior treatments for Hepatitis C were much less effective in Black patients).
Yet, “the most severe forms of Crohn’s –peri-anal and fistulizing disease– are more common in Black patients.”
Review of emergency visits of IBD children “showed that Black children received less medication and had more repeat emergency room visits than white children.” (Inflamm Bowel Dis 2019; 25: 194-203)
Because IBD is not perceived to occur frequently in Black patients, the author states that some patients are not accommodated by their employers and patients are less comfortable with support groups.
“However, the incidence of Crohn’s disease …in Black people has risen sharply over the past 3 decades…now approaches that of non-Hispanic whites.”
My take: Inflammatory bowel disease is definitely a disease that affects Black people; it is often more severe and requires careful treatment.
Billy Goat Trail, Chesapeake and Ohio Canal National Historic Park (outside Washington D.C.). Yes, we made it to the top!
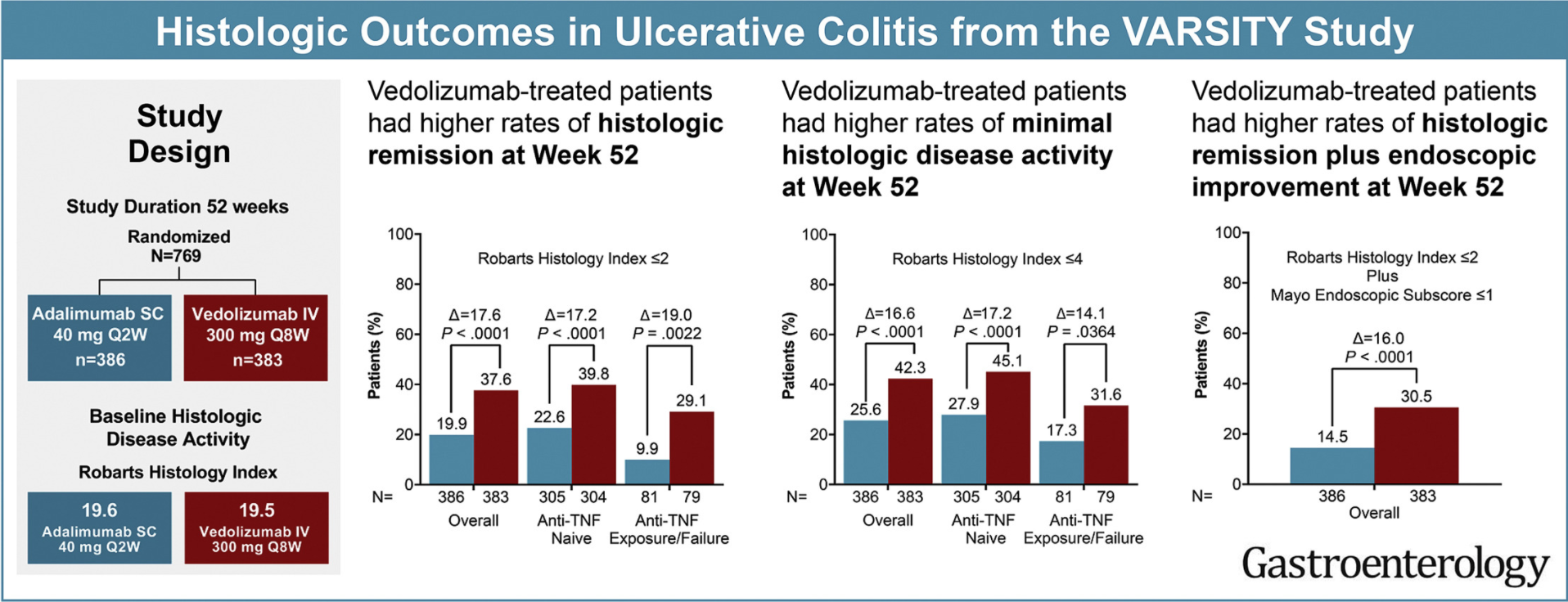
In total, 769 patients received vedolizumab (n = 383) or adalimumab (n = 386). Geboes Index and Robarts Histopathology Index (RHI) scores were used to assess prespecified histologic exploratory end points of histologic remission (Geboes <2 or RHI ≤2) and minimal histologic disease activity (Geboes ≤3.1 or RHI ≤4) at weeks 14 and 52.
Key findings:
Vedolizumab induced greater histologic remission than adalimumab:
week 14: Geboes: 16.7% vs 7.3%, RHI: 25.6% vs 16.1%
week 52: Geboes: 29.2% vs 8.3%, RHI: 37.6% vs 19.9%
Histologic outcomes were generally better in anti–TNF-naïve vs -failure patients
My take: This study shows that histologic outcomes with vedolizumab, similar to clinical outcomes, were better than with adalimumab. Some of this difference could be due to the trail design which did not allow optimization of adalimumab dosing.