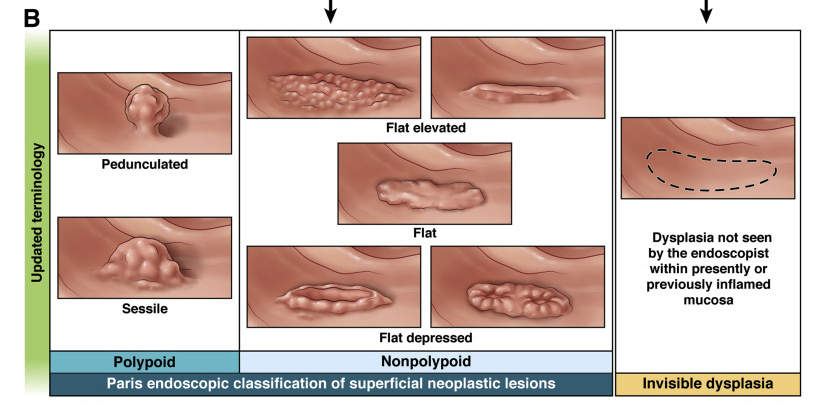
Best Practice Advice 1: Precancerous colorectal lesions in inflammatory bowel disease should be described as either polypoid (≥2.5 mm tall), nonpolypoid (<2.5 mm), or invisible (detected on nontargeted biopsy), using a modified Paris Classification. The older terms dysplasia-associated lesion or mass, adenoma-like mass, and flat dysplasia (when referring to dysplasia detected in nontargeted biopsies) should be abandoned.
Best Practice Advice 3: Initial colonoscopy screening for dysplasia should be performed at 8–10 years after disease diagnosis in all people with colonic inflammatory bowel disease, and immediately on diagnosis of primary sclerosing cholangitis. Staging biopsies should be taken from multiple colonic segments to assess histologic disease activity and extent and to help guide future surveillance intervals.
Best Practice Advice 8: Extensive nontargeted biopsies (roughly 4 adequately spaced biopsies every 10 cm) should be taken from flat colorectal mucosa in areas previously affected by colitis when white light endoscopy is used without dye spray chromoendoscopy or virtual chromoendoscopy. Additional biopsies should be taken from areas of prior dysplasia or poor mucosal visibility. Nontargeted biopsies are not routinely required if dye spray chromoendoscopy or virtual chromoendoscopy is performed using a high-defintion endoscope, but should be considered if there is a history of dysplasia or primary sclerosing cholangitis.
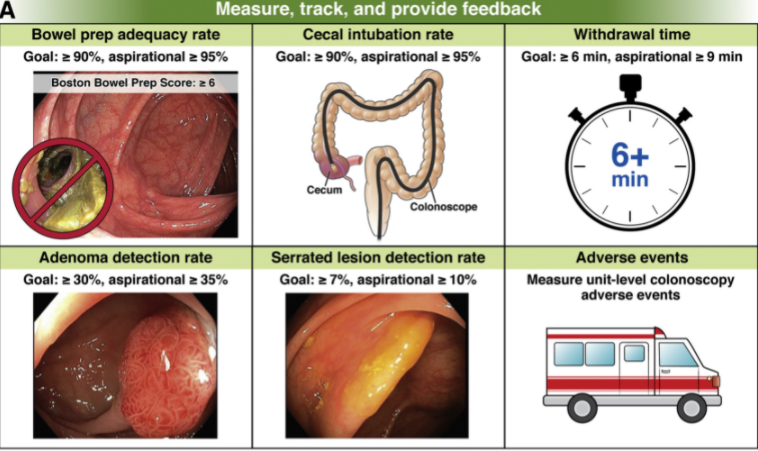
While these guidelines are geared towards adult gastroenterologists for colorectal cancer screening, some advice is universally applicable
tracking quality metrics: good prep, cecal intubation rate, and adverse events
good bowel preparation instructions
detailed endoscopy reports
appropriate followup: All patients with advanced adenomas should have repeat colonoscopy in 3 years. Average-risk patients with normal screening colonoscopies or those with only small distal hyperplastic polyps should not undergo repeat examinations before 10 years
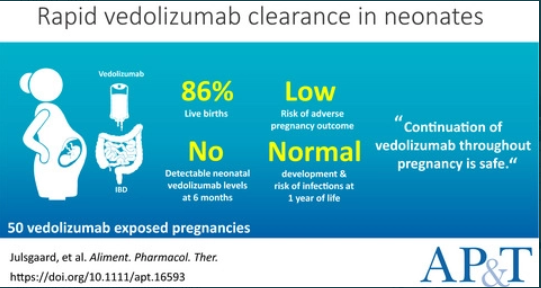
In 50 vedolizumab-exposed pregnancies, we observed 43 (86%) live births, seven (14%) miscarriages, no congenital malformations and low risk of adverse pregnancy outcomes
The mean time to vedolizumab clearance in infants was 3.8 months (95% CI, 3.1-4.4)
No infant had detectable levels of vedolizumab at 6 months of age
Developmental milestones at 12 months were normal or above average
Neither vedolizumab exposure in the third trimester (RR 0.54, 95% CI, 0.28-1.03) nor combination therapy with thiopurines (RR 1.29, 95% CI, 0.60-2.77) seemed to increase the risk of infections in the offspring
My take: Given the good safety profile of vedolizumab, this small study provides additional reassurance regarding use of vedolizumab during pregnancy.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
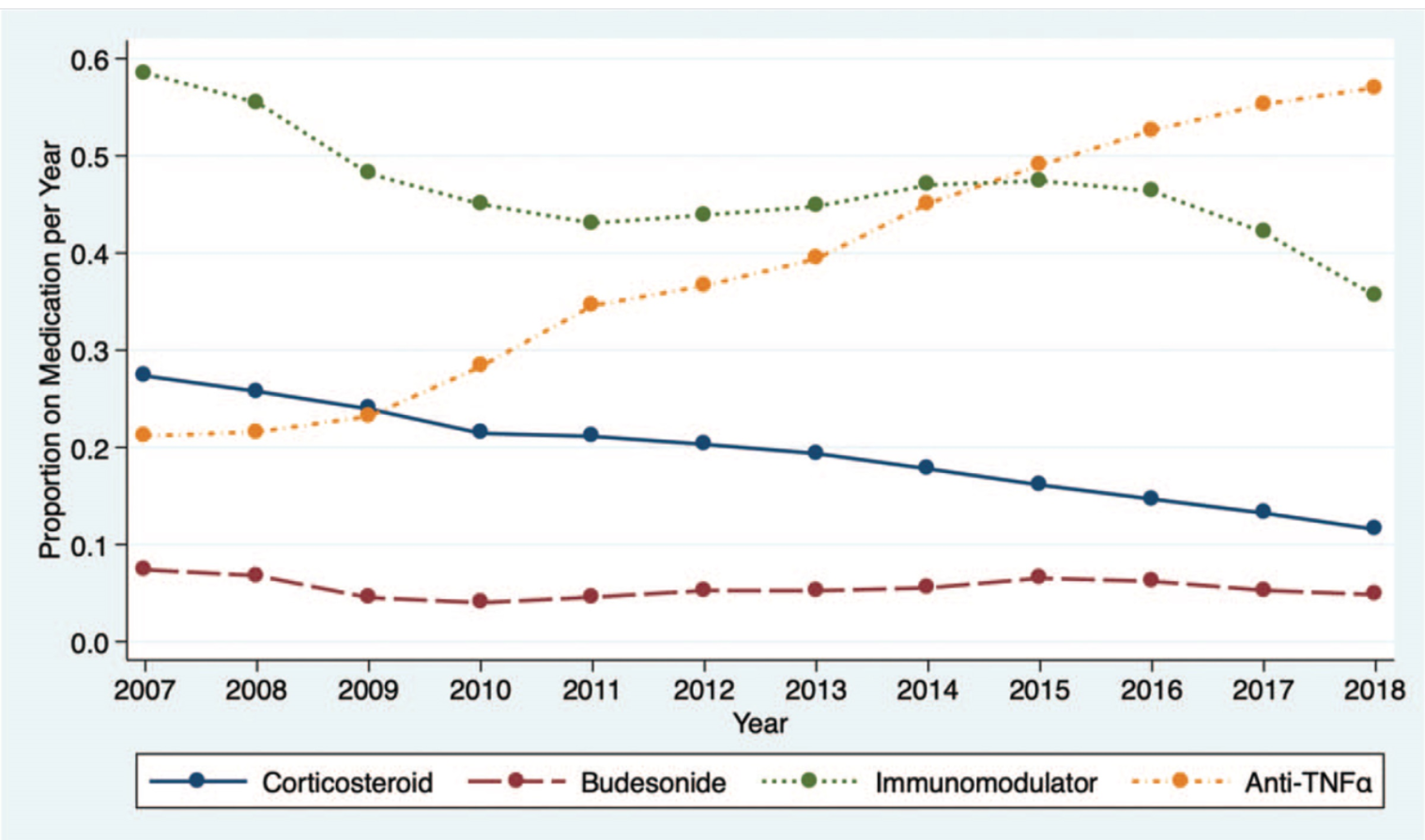
In this study of 27,321 patients enrolled in the ImproveCareNow (ICN) learning health system, key findings:
Corticosteroid use decreased from 28% (2007) to 12% (2018)
Black patients received corticosteroids more commonly than white patients. This disparity improved as corticosteroid use decreased in both groups
Anti-tumor necrosis factor-alpha medication use <120 days after diagnosis was associated with a reduction in corticosteroid use
As corticosteroid use decreased, steroid-sparing therapy use increased and height and weight z scores improved, particularly among children with Crohn disease
27 centers (31%) had a significant reduction in steroid use, 5 (6%) had a significant increase, and 45 (52%) had variability in steroid use. 9 centers (11%) had <2 years of data.
My take: These findings are expected but nice to see. Patients in the ICN are using less steroids and growing better. Given the variation in care among centers, there is more work needed.
There are a lot of articles that have been published regarding bowel preparations prior to colonoscopy, especially in adults. One of the key advances has been split-prep dosing, which is not utilized much in the pediatric age group.
Nevertheless, a recent pediatric study (S Kumar et al. JPGN 2021; 73: 325-328. Inadequate Bowel Preparation in Pediatric Colonoscopy—Prospective Study of Potential Causes) shows that inadequate bowel preparation in their prospective cohort (n=334) was less prevalent than that noted from typical adult data. Their bowel preparation assessmetn was based on Boston Bowel Preparation Scale (BBPS).
Key finding: Inadequate bowel preparation (IBP) was noted in 12.8% (41/321); there were no age, gender, obesity, race, or insurance type associated with IBP. (IBP was defined by BBPS <5)
Their preparation instructions:
If <25 kg, “119 g of PEG 3350 mixed in 32 oz of sport drink” and then “additional 32 oz of a sports drink without PEG 3350”
If 26-49 kg, “238 g of PEG 3350 mixed with 64 ounces of fluids” and then “additional 64 oz of a sports drink without PEG 3350”
If >50 kg, “238 g of PEG 3350 mixed with 64 ounces of fluids” and then “64 ounces of a sports drink and four bisacodyl tablets”
My take: If you are seeing a high rate of IBP, the prep instructions in this study could be replicated (given their good results), split preps could be given for teens, and better instructions (visual aids) could be needed.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Zen Magnets Recall (from Twitter feed/Bryan Rudolph):
Link now updated with an FAQ “#Recall: Zen Magnets & Neoballs magnets. Ingestion hazard to children & teens, risk of injury or death. Get refund. https://zenmagnets.com/CPSC-Recall” – @USCPSC Mandated Message #3
This article is a proof-of-concept study describing the use of “3D-Transit system” to provide information on regional gastrointestinal motility. This study examined 20 healthy children who ingested a electromagnetic capsule (21.5 mm x 8.3 mm) which was tracked by a vest detector.
Key findings:
Median whole gut transit time was 33.6 (range 10.7–80.5) hours
Median gastric emptying time was 1.9 (range 0.1–22.1) hours
Median small intestinal transit time was 4.9 (range 1.1–15.1) hours
Median colonic transit time was 26.4 (range 6.8–74.5) hours.
Table 1 provides the median values along with 5%, and 95% values.
Limitations: small sample size, and this system requires manual analysis. In addition, the capsule itself due to its size and viscosity may influence transit times.
My take: This capsule motility study suggests that whole GI tract transit averages 34 hrs. This system could provide some objective data on motility in children and it is probably more useful than the corn test (though not as tasty); however, I doubt its use will be more helpful than Sitz markers for the majority.
This image shows the capsule in lower left corner and the vest with the white detector panel.
A couple of interesting recommendations in this updated position paper on the use of percutaneous endoscopic gastrostomy (PEG) include the following:
Feeding can be initiated as early as3 hours post-procedure in a stable child with no complications.
“Iso-osmolar feeds of the standard polymeric formula are the best type of foodto start with after the PEG insertion” and ” bolus feeding is more physiological and should be the first choice… in some children, small boluses during the day could be combined with the overnight continuous feeding via enteral pump.”
“Replacing the initial tube with a gastric balloon/button should be recommended to the families/children who will need long term enteral nutrition to improve quality of life.”
“Gastric balloons should be replaced every 6 months, but non-balloon PEGs can be replaced annually.”
The full article provides a rationale/nuance for these recommendations. Use of feeds starting at 3 hrs post-op has been found to be safe. And, there is no evidence available that suggests routine use of a clear fluid test or dilute or hypotonic feed after the procedure. In fact, it has been suggested that these measures delay the time to full enteral intake and prolong hospital stay.
With regard to balloon button Gtube changes, the authors note that while manufacturers recommend changing every 3 months, “in the majority, these are safe to replace less frequently.”
The authors clearly favor low-profile buttons and state that changing to them earlier after initial Gtube placement (after 1 month) under general anesthesia should be safe (if no issues with healing like diabetes, and systemic corticosteroids); “however, the physician should give the parents/child the possibility of choice whether to perform the replacement or not.” Also, “the primary device can stay in place for one year or even more. In a German study, 85% of parents answered that the GB is advantageous over primary gastrostomy tube due to mobility, patient comfort at physiotherapy, swimming or night-time sleep, and higher parent satisfaction.”
My take: This article provides a good summary of PEG indications/contraindications, complications, and advise for clinicians
www.feedingtubeawareness.com This site contains a terrific PDF download which explains enteral tubes in an easy to understand style along with good graphics. “What You Need to Know Now, A Parent’s Introduction to Tube Feeding is the guidebook that every parent wished they had when they were first introduced to feeding tubes.”
Shelburne Farms, VT
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
The panel agreed that reactive TDM should be used for all biologics for both primary nonresponse and secondary loss of response
It was recommended that treatment discontinuation should not be considered for infliximab or adalimumab until a drug concentration of at least 10–15 mg/mL was achieved
Consensus was also achieved regarding the utility of proactive TDM for anti–tumor necrosis factor therapy. It was recommended to perform proactive TDM after induction and at least once during maintenance.
More data are needed with regard to proactive TDM for biologics other than anti-TNF agents
There are no differences in interpreting TDM between originator biologics and biosimilars
When considering switching within drug class in case of secondary loss of response to a first anti-TNF drug because of the development of antidrug antibodies, an immunomodulator should be added to a subsequent anti-TNF therapy
Low-titer antidrug antibodies can be overcome by treatment optimization (dose escalation, dose interval shortening, and/or addition of an immunomodulator)
My take: This article should help support the practice of proactive TDM and discourage stopping anti-TNF agents until an adequate therapeutic level is achieved.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Methods: A multicampus, retrospective cohort evaluation was conducted among patients aged ≤18 years with any history of clinical CDI and receiving systemic antibiotics in a subsequent encounter from 2013–2019. This study identified 30 and 44 patients received oral vancomycin prophylaxis (OVP) and no OVP, respectively. Eligible patients had to be >12 months of age and having at 3 unformed stools everyday.
OVP dosing: “vancomycin doses of 10 mg/kg (up to 125 mg per dose) every 12 hours during concomitant antibiotic use. OVP duration was intended to continue while on systemic antimicrobial agents and for 5 days after completion of antimicrobial agents (extended prophylaxis tail), but practice varied, and duration was ultimately left to the discretion of the provider.”
Key finding:
The incidence of CDI recurrence within 8 weeks of antibiotic exposure was significantly lower in patients who received OVP (3% vs 25%; P = .02) despite this group having notably more risk factors for recurrence. After adjustment in a multivariable analysis, secondary OVP was associated with less risk of recurrence (odds ratio, 0.10; 95% confidence interval, 0.01–0.86; P = .04).
This study is in agreement with studies in adults (Brown CC, et al. Oral Vancomycin for Secondary Prophylaxis of Clostridium difficile Infection. Ann Pharmacother. 2019 Apr;53(4):396-401). In this review, the authors state: “Variable dosing regimens and lack of safety data are limitations.. clinicians can consider vancomycin 125 mg orally once or twice daily in high-risk patients receiving broad-spectrum antibacterial agents.”
My take: In patients at high risk of recurrent CDI, OVP should be considered as secondary prophylaxis when receiving systemic antibiotics.
A recent study (MT Dolinger et al. Inflamm Bowel Dis 2021; 27: 1210-1214) and the associated editorial (D Geem, S Kugathasan. Inflamm Bowel Dis 2021; 27: 1361-1362) describe the use of multiple therapies (biologics and small molecule therapy) to target refractory pediatric inflammatory bowel disease. Since the term “combination therapy” is already in broad use for those receiving a biologic agent and an immunomodulator, I plan to refer to these new combinations as ‘dual immunotherapy’ for IBD.
Dolinger et al (Dual Biologic and Small Molecule Therapy for the Treatment of Refractory Pediatric Inflammatory Bowel Disease) described 16 children with dual immunotherapy. Nine (56%) were treated with vedolizumab/tofacitinib, 4 (25%) with ustekinumab/vedolizumab, and 3 (19%) with ustekinumab/tofacitinib. Twelve (75%; 7 ulcerative colitis/IBD-unspecified, 5 Crohn’s disease ) achieved steroid-free remission at 6 months. One patient on 30 mg of vedolizumab/tofacitinib and prednisone daily developed septic arthritis and a deep vein thrombosis.
Except for “anti-TNF medications (infliximab and adalimumab), no other biologic therapies are FDA-approved for children with IBD”
“Clinical disease remission is achieved in only 40-60% of patients on anti-TNF medications”
With ustekinumab, “limited pediatric data reveal that in patients who have failed at least 1 biologic therapy, 38.6-58% achieve clinical remission by week 52…[And] vedolizumab …demonstrated steroid-free remission in 20% by week 22 in a single-center prospective observational cohort study.”
The response to dual immunotherapy is most likely due to the synergistic effects of two medications rather than the start of a new medication. The authors note a prior study which showed a positive experience of adding ustekinumab in 5 children who developed severe paradoxical psoriasis with infliximab and in another subset of pediatric patients, there was improvement with combination vedolizumab/infliximab (Paediatr Drugs 2020; 22: 409-416)
My take (borrowed from editorial): “Given the phenotypic heterogeneity of pediatric IBD and the multiple inflammatory immune pathways implicated in its pathogenesis, the approach of biologic monotherapy–may not be suitable for all patients…patients may require specific combinations…to quell multiple arms of their dysregulated immune response.” More trials are needed to determine the safety of these regimens (especially with regard to malignancy and infections).