S Bonilla et al. JPGN 2021; 73: 178-183. Low Adherence to Society Guidelines for the Management of Helicobacter Pylori Among Pediatric Gastroenterologists
This retrospective study with 250 patients determined that clinicians at this large center (Boston Children’s) have a low rate of adherence to the NASPGHAN/ESPGHAN H pylori guidelines (JPGN 2017; 64: 991-1003).
Key findings:
- Patient outcomes: 107/186 (58%) had resolution of symptoms after treatment; abdominal pain was the most common presenting symptom (67%)
- 131 (62%) had documented followup visit and an eradication test
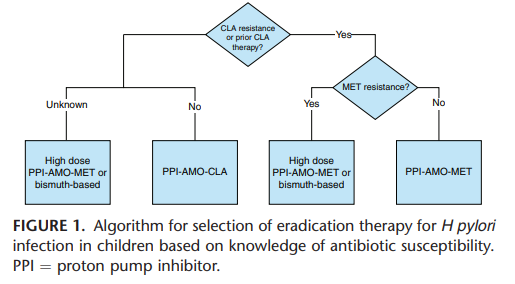
- First-line treatment was most commonly amoxicillin, clarithromycin, and PPI (69%) (in those without sensitivity information, amoxicillin, metronidazole, and PPI are recommended in the guidelines)
- Biopsy culture was sent in 3% of patients
In their discussion, the authors make a number of points:
- Both pediatricians and gastroenterologists “are utilizing a ‘test and treat’ strategy rather than endoscopy-based diagnostic testing.” This along with low followup and low biopsy culture deviate from NASPGHAN guideline.
- 77 of 256 patients had non-invasive testing prior to referral and in this subset, more than two-thirds of patients received a clarithromycin-based triple therapy before being referred; “this has a high likelihood of failure.”
- The authors advocate endoscopy over empiric treatment but acknowledge some reasons why families may want to avoid endoscopy (interestingly the authors do not mention the cost of the procedure). They also note that H pylori culture is not widely available.
My take: There are several reasons why there is low adherence to NASPGHAN/ESPGHAN guidelines
- Treatment recommendations for initial triple therapy does not align with adult guidelines for quadruple therapy. Even the “rescue” therapies (Table 5), these pediatric guidelines do not recommend quadruple therapy. Yet, there is no indication that H pylori is more susceptible to treatment in children.
- Recommendations for susceptibility/antibiotic resistance testing (Table 1, #11) makes no sense if susceptibility testing is not available. Fortunately, PCR-based assays are making this easier recently.
- The absence of susceptibility testing and cost would favor empiric treatment over endoscopy as a first-line approach in those who have a reliable non-invasive test indicating infection along with symptoms suggestive of H pylori infection.
Related blog posts:
Adult Guidelines:
- Quadruple Therapy for Helicobacter Pylori Favored in Toronto Guidelines
- ACG Guideline for Helicobacter Pylori | gutsandgrowth
Other related posts
- AGA: Best Practice Advice for Refractory H pylori
- Lots of Room to Improve with H pylori Treatment | gutsandgrowth
- Rifabutin-based Triple Therapy for H pylori | gutsandgrowth
- It is Getting Harder to Treat H pylori -Here’s Why
- Updated Pediatric H pylori Guidelines
- Understanding Resistance to Helicobacter pylori | gutsandgrowth
- Salvage Therapy and Standard Therapy for H pylori | gutsandgrowth
- High Rates of Helicobacter Pylori Resistance | gutsandgrowth
- What is evidence-based medicine for H pylori? gutsandgrowth
- H pylori –useful advice gutsandgrowth
- Twyman’s Law | gutsandgrowth
do NOT align with treatment recommendations in adults