Seven studies reported the prevalence of IDTI (Incidentally-diagnosed terminal ileitis) in 44,398 persons undergoing non-diagnostic colonoscopy
The pooled prevalence rate of IDTI was 1.6%
Progression to overt CD was rare over 1-7 years of followup
My take: As noted below by Dr. Rubin, in those with normal labs who are asymptomatic, most incidental ileitis is not progressive and should be monitored.
This slide from @RealCecum Twitter Feed and @IBDMD Twitter Feed
This prospective observational study provides helpful outcome data for infants (n=80) born with congenital duodenal obstruction (CDO).
Key findings (also see infographic below):
Though there was an 8.4% overall mortality, there were no deaths directly attributed to CDO. 69% had associated anomalies.
Median length of stay after repair was 20 days; at 28 days following repair, 76% had been discharged home
Failure to achieve full enteral feeds was NOT related to CDO (due instead to other gastrointestinal anomalies). Mean time for full feeds was 13 days post-op; 90% reached full enteral feeds at 28 days.
Repair type: 80% had duodenoduodenostomy, 14% had duodenojejunostomy, the others: membrane incision (n=1), membrane resection (n=2), and duodenoplasty (n=2)
My take: This data will inform clinicians of expected outcomes in this population. I hope this cohort is followed long-term to provide more information about long-term outcomes including frequency of pancreatitis.
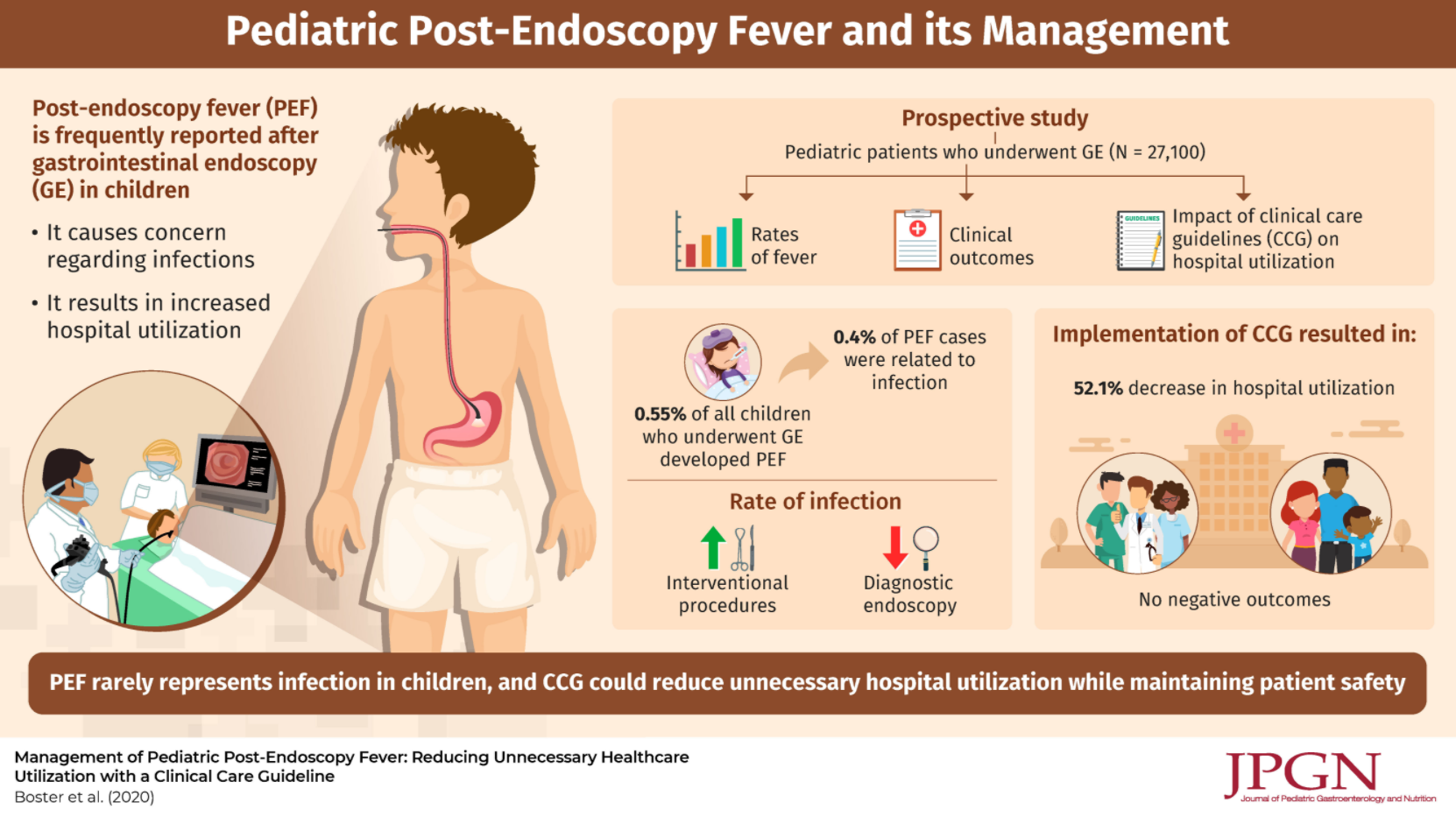
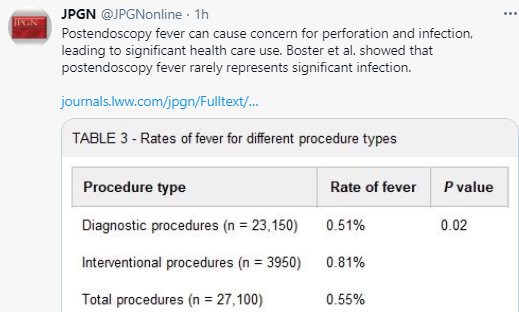
Using a prospective database with 27,100 endoscopies, the authors evaluated a clinical care guideline to reduce unnecessary medical care following endoscopy.
Key findings:
Post-endoscopy fever (PEF) occurred in 0.55% (n=150)
ONLY 6 of these 150 PEFs (0.4%) were attributed to a procedure complication: 3 had perforations (all with abdominal pain), 2 had aspiration (both had emesis at time of endoscopy) and 1 had a positive blood culture (though had undergone a liver biopsy as well as endoscopy)
The authors published their care guideline (Figure 1) which stratifies risk based on whether the procedure was an interventional (high risk) vs diagnostic (low risk), ASA class, duration of fever, concomitant immunosuppression (eg. steroids), and associated symptoms including vomiting, diarrhea, bleeding, new abdominal pain, impact on activities of daily living, and hydration
Interestingly, the authors note that their cohort had a total of 23 perforations, but only 3 presented with fever
Using the care guideline resulted in a “significant shift in the prevalence of Grade 2 and above (requiring hospital use) to Grade 1 (clinical observation and reassurance) adverse events, dropping ED visits and admissions by 43.6% and 76.4% respectively for the post-endoscopy fever patients.” This shift was not associated with any observed negative patient outcomes or missed diagnoses.
My take: The authors note that fever is often related to release of inflammatory cytokines which can occur with endoscopy in the absence of complications. The authors methodical guideline to post-procedure fever provides a logical approach to this common problem.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Related article: AE Wiskin et al. Clin Nutrition 2021; https://doi.org/10.1016/j.clnesp.2020.12.029. Prevalence of Home Parenteral Nutrition in childrenKey finding: In 2019, 389 children received HPN (home parenteral nutrition) in the UK; this is nearly double the number last reported in 2012 and is a prevalence of 30 per million children (Thanks to Kipp Ellsworth for this reference)
In total, 59% of children with BMI z-score <−0.5 had moderate-severe osteopenia and only 18% of those with higher z-scores.
Osteopenia was associated with lower BMI z-score (−0.8 ± 1.2 vs −1.8 ± 1.1, P < 0.001) and higher PCDAI (33.7 ± 15.2 vs 25.7 ± 16.5; P = 0.009)
None of the higher risk patients were receiving long-term corticosteroids
Limitations: retrospective study with relatively small sample size, pubertal stage not recorded, variability in DXA studies, and lack of followup information
My take: The authors have NOT shown that identification of osteopenia at the time of diagnosis improves outcome of Crohn’s disease or bone disease. This is why I disagree with their recommendation to routinely screen children with BMI z-score <−0.5. In those in which finding osteopenia may influence treatment, then a DXA study would be worthwhile.
A recent large retrospective study (R Mandile et al. JPGN 2021; 72: 282-287. Seronegative Villous Atrophy in Children: Clinical and Immunohistochemical Features) provides information about conditions, besides celiac disease (CD) which present with villous atrophy. 64 of 1282 pediatric patients were seronegative with villous atrophy; seronegative was defined as testing negative twice for serology (TTG IgA/EMA or if IgA-deficient, IgG antibody serology).
Key findings:
Diagnoses were: inflammatory bowel diseases (IBD) (21/64), food allergy (8/64), infections (7/64, of which 3 HIV infections), immune deficiency (3/64), short bowel syndrome (3/64), congenital diarrhea (2/64), other/inconclusive diagnosis (8/64). In addition, there were 12 with Gastro-Esophageal Reflux Disease (GERD) & the authors speculate that perhaps hyperacidity could play a role in some of these cases.
Only one quarter of the seronegative patients had an increased number of intraepithelial lymphocytosis (IELs)
Among those with villous atrophy attributed to IBD, this was nearly equally-split between Crohn’s disease and ulcerative colitis, 10 and 11 patients respectively (according to Table 1)
The authors note that the ~5% of patients with seronegative villous atrophy with alternative diagnosis than Celiac disease may be an overestimation as more individuals are being diagnosed without biopsy based on serology
Despite the large cohort, there are still other rare conditions that were not identified in this study (eg. autoimmune enteropathy, CTLA4B deficiency,drug-induced enteropathy, and tropical sprue)
My take: This article provides a good starting point for patients with villous atrophy and negative serology.
During the study period 12,744 children underwent an EGD with biopsies. Of those, we identified 426 children with LD (3%).
Among the LD (compared to control group), 5% had celiac disease (vs 0%, P < 0.001), 9% had Crohn disease (3%, P = 0.003) and 3% had Helicobacter pylori gastritis (1%, P = 0.021).
After a median follow-up of ~32 months, 13 of 20 responders (65%) reported clinical improvement from endotherapy/mPES.
A genetic variant was identified in 19/26 (73%) tested patients
Post-ERCP pancreatitis (PEP) was the only observed adverse event; 21% (12/58)
Discussion:
The authors note that the beneficial finding of improvement after mPES in children is contrary to findings in adults. In addition, there is an active sham-controlled randomized clinical trial ongoing in adults (NCT03609944). They speculate that this could be related to longer disease burden in adults. In addition, they note that their findings had limitations:
this was a retrospective study with a small sample size
the results were based on a subjective non-validated questionnaire with concerns for recall bias
My take: I am not convinced that sphincterotomy is beneficial in most children with pancreatitis and pancreas divisum –the majority of whom have an underlying genetic variant which likely triggers pancreatitis. The only way to answer this question definitely is to perform a randomized clinical trial similar to the sham-controlled study in adults.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
S Kemme et al. JPGN 2021; 72: 194-201. Outcomes of Severe Seronegative Hepatitis-associated Aplastic Anemia: A Pediatric Case Series This small case series (n=4) with HAAA found that this condition was poorly responsive to steroids, azathioprine and tacrolimus; however, Anti-Thymocyte Globulin (ATG) was associated with sustained biochemical remission of the hepatitis. Two patients underwent hematopoietic stem cell transplantation. All patients had extensive investigations. All had evidence of systemic hyperinflammation (with markedly-elevated ferritin and soluble IL-2 R levels) and CD8+ T cell predominant liver tissue infiltration.
Workup: In the well and stable premature with elevated DB, “aminotransferases, AP, GGT, glucose, T4, TSH, UC, urine CMV PCR, and US with Doppler evaluation should be obtained…Coagulation studies in well babies with other evidence of good synthetic function are not necessary.” Empiric ursodeoxycholic acid may be given with weekly evaluation.
Genetic testing: “Genetic panels are indicated in babies with no obvious risk factors after the first tier of studies…In critically ill babies with multisystem disease, critical whole exome sequencing (WES) is faster and provides broader results.”
Sepsis: Babies with sudden increase in DB and ALT should be evaluated for sepsis (including urosepsis) and CMV.
Nutritional support: Infants should be “supported with MCT and vitamin supplementation.”
Severe liver disease: “Babies with coagulopathy and marked elevation of aminotransferases who have multiorgan failure in the first few days of life need to be evaluated for perinatal complications, severe metabolic disease, and gestational alloimmune liver disease (GALD). In this period, ischemic shock or infectious disease is much more common than primary liver disease, but the presentations can overlap.”
Liver biopsy: “Liver biopsy should be pursued in babies whose cholestasis is not improving and the diagnosis is unclear.”
Etiology: Infection, genetic disease, cardiac dysfunction, large heme loads, and hypothyroidism are common causes of liver dysfunction in the NICU. Common findings included trisomy 21-associated liver dysfunction (n=12), and thyroid disease. 6 patients had type 2 Abenathy shunts -only one required closure. Two patients had biliary atresia. Other liver diseases identified included GALD (n=2), PFIC2, Alagille, Alpha-one-antitrypsin, Cystic Fibrosis, and Niemann-Pick.
Wahid N et al. AASLD 2020, Abstract 153. Summary from GI & Hepatology News: Liver-related deaths decline after Medicaid-expansion under ACA. “Beginning around 2015, liver-related deaths began to decline in expansion states by a mean of –0.6%, while they continued on an upward trajectory in the nonexpansion states…“It’s a no-brainer that the lack of insurance accessibility for the most vulnerable people in the United States meant that they were dying of cirrhosis instead of being transplanted,” said Elliot Benjamin Tapper, MD, of the University of Michigan, Ann Arbor.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.