AD Sperber et al. Gastroenterology 2021;160:99–114. Full text PDF. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study
A global epidemiological study of functional GI disorders
• 73,076 adults surveyed (33 countries, 6 continents)
• Data collection: By Internet (24 countries), by household interview (7 countries), or both methods (China and Turkey, green).
Key findings:
- Diagnostic criteria were met for at least 1 FGID by 40.3% persons who completed
the Internet surveys and 20.7% of persons who completed the household surveys - FGIDs were associated with lower quality of life and more frequent doctor visits
My take: In industrialized countries, about 40% have functional GI disorders.
Related article: C Ma et al. Gastroenterol 2021; 160: 88-98. Full text: Epidemiologic Burden and Treatment of Chronic Symptomatic Functional Bowel Disorders in the United States: A Nationwide Analysis
From 2007–2015, approximately 36.9 million (95% CI, 31.4–42.4) weighted visits in patients of non-federally employed physicians for chronic symptomatic FBDs were sampled. There was an annual weighted average of 2.7 million (95% CI, 2.3–3.2) visits for symptomatic irritable bowel syndrome/chronic abdominal pain, 1.0 million (95% CI, 0.8–1.2) visits for chronic constipation, and 0.7 million (95% CI, 0.5–0.8) visits for chronic diarrhea. Pharmacologic therapies were prescribed in 49.7% (95% CI, 44.7–54.8) of visits compared to nonpharmacologic interventions in 19.8% (95% CI, 16.0–24.2) of visits (P < .001). Combination treatment strategies were more likely to be implemented by primary care physicians and in patients with depression or obesity. The direct annual cost of ambulatory clinic visits alone for chronic symptomatic FBDs is approximately US$358 million
Related blog posts:
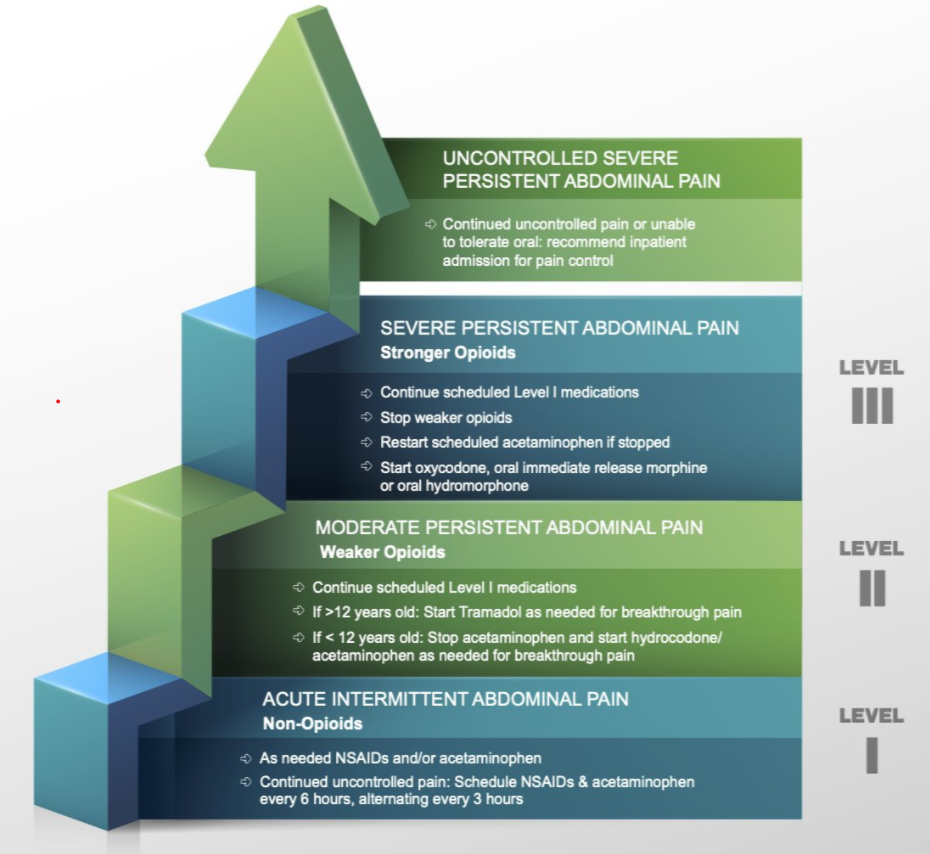
- Advice on Abdominal Pain for Everyone Who Treats Children
- #NASPGHAN19 Postgraduate Course -part 3
- Narrowing the Workup for Chronic Abdominal Pain –Carlo DiLorenzo Was Right! | gutsandgrowth
- “Implementing psychological therapies for gastrointestinal disorders in pediatrics”
- Prevalence of Rome IV Functional Bowel Disorders in Adults (US, UK, Canada) & Largest Study to Date on Hydroxychloroquine for COVId-19 | gutsandgrowth
- “Golden Half Hour in Chronic Pain” | gutsandgrowth