NASPGHAN Webinar: (Link -requires registration to view): Changing the Dynamic: How to Enable EHRs to Work for You (if trouble with this link, go to https://learnonline.naspghan.org/webinar)
This webinar featured lectures by the following:
- Steven Liu for Epic functionality (in the ~first 20 minutes)
- John Pohl for Cerner functionality (in the ~second 20 minutes)
- Jennifer Lee discussed patient portal, improving provider-patient communication, & protecting adolescent confidentiality-21st Century Cures Act
- Jeannie Huang discussed the role of EHRs in value-based health care and clinical data collection.
Since our group mainly uses Epic, I will summarize some of the tips from Steven Liu, who also is our group’s Epic Physician Champion. Anyone who listened to the webinar will realize how there are so many tricks available. Some of the material from the talk is at the bottom in the form of screenshots; however, much of the information in the webinar is proprietary to EPIC and cannot be shared without permission.
Here are some of the key points:
- Customize your templates for progress notes/H&Ps/other notes.
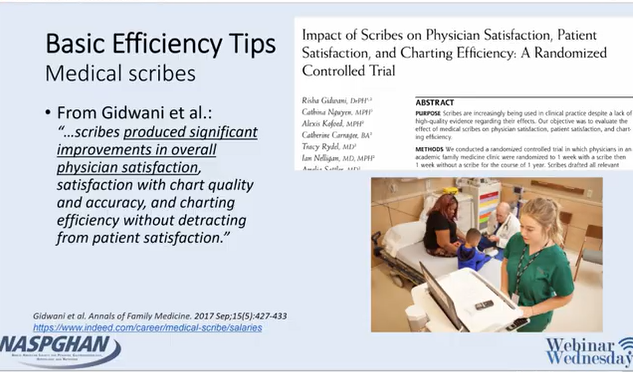
- Scribes may relieve frustration and be a good investment
- Use Smartphrases and Smartlinks
- Smartphrases can be taken (or customized) from other users -can browse your superusers phrases by looking under Smartphrase manager
- Smartforms can be very useful (eg. ImproveCareNow)
- Using Dictionary, users can change autocorrect: example: if you type EoE, you could have it modified to Eosinophilic Esophagitis
- Utilize/incorporate patient-entered questionnaires
- Utilize customized filters (wrench icon) under the chart review tabs
- Take advantage of the Chart Search function
- can search “PPI” or “calprotectin” and this will identify if patient has used a PPI or had a calprotectin
- can access this feature quickly with CTRL-spacebar
- Shortcuts can save time -examples ALT-A and ALT-S
- Take the time to build customized order panels, like “Celiac Annual Labs”
- Health Maintenance Checklists can be incorporated but users may need their system to activate this feature
- There is an Inbox Reminder function (to remind patient to get an appointment or test) or you can send a inbox message to yourself with a future date
- For more sophisticated users: generating reports with Workbench
- Epic has free classes (User Web -see slide below) available to help practitioners become more proficient (eg. Power User Course)
My take: Steven has helped everyone in our practice & listening to his talk makes me realize that I need to learn a good bit more and take some of his stuff. This EHR webinar provides a lot of tips to help good EHR users become better users. For those interested in research, understanding EHRs will be crucial going forward.
Related blog posts:
- Be Kind & the 21st Century Cures Act
- EMR Learning Curve -Long-term Benefits & Burnout Narrative
- What Went Wrong with EMRs: Death by 1000 Clicks