In this retrospective observational longitudinal cohort study with 3007 patients with IBD from the ImproveCareNow Network, the authors found a high rate of continued linear growth after expected growth plate closure (15 years in females, 17 years in males).
Key findings:
80% manifested continued growth beyond the time of expected growth plate closure, more commonly in CD (81%) than UC (75%; P = 0.0002)
Median height gain was greater in males with CD (1.6 cm) than in males with UC (1.3 cm; P = 0.0004), and in females with CD (1.8 cm) than in females with UC (1.5 cm; P = 0.025)
My take: This study provides additional information about delayed skeletal maturation in the pediatric population with inflammatory bowel disease. Interestingly, the rate of continued growth with ulcerative colitis was nearly as high as with Crohn’s disease.
Using more than 11 million subjects enrolled in Nationwide Korean database, the authors explored the associations between statin use and fatty liver disease in adults (20 yrs or older).
Key findings:
The use of statin was associated with a reduced risk of NAFLD development (adjusted odds ratio [AOR] 0.66; 95% confidence interval [CI] 0.65–0.67). NAFLD was diagnosed by calculating fatty liver index (FLI).
The use of statins reduced the risk of significant liver fibrosis (AOR 0.43; 95% CI 0.42–0.44). Fibrosis was based on a BARD score ≥ 2.
The effects of statins may be mediated by anti-inflammatory and antifibrotic actions, which have been evident in experimental models of chronic liver disease.
My take: Statin use appears beneficial in patients with NAFLD. Since dyslipidemia is frequent in patients with NAFLD, there should be a low threshold for using statin therapy.
NAFLD Guidance from AASLD (2018) One of the recommendations includes the following: In patients with suspected NAFLD, the authors recommend evaluation for comorbidities including dyslipidemia, diabetes, hypothyroidism, polycystic ovary syndrome, and sleep apnea.
A recent editorial (NL Schecter et al. JAMA Pediatr. 2021;175(1):7–8. doi:10.1001/jamapediatrics.2020.1798. Full text: The Golden Half Hour in Chronic Pediatric Pain—Feedback as the First Intervention -thanks to Ben Gold for this reference) notes that with pain we need to take a more holistic approach: ” Commonly, patients with chronic pain are evaluated by multiple clinicians, including pediatricians and specialists, each of whom may have addressed only one of the child’s persistent symptoms (ie, headache, abdominal pain, dizziness, nausea, or fatigue). When each symptom is addressed in isolation, it seldom provides comprehensive relief. Moreover, this process can foster a family’s belief that each symptom represents a distinct illness.”
Key points:
Brief feedback discussion following an assessment for pediatric chronic pain may be akin to the “golden hour” in trauma or neonatal care. During this critical time, there is an opportunity to connect with a family, clarify misconceptions, move toward a shared biopsychosocial understanding of pain, and engage families in a comprehensive plan for recovery.”
Tips for mastering the golden hour:
Elicit Parent and Child Expectations at the Outset “This facilitates a thorough understanding of a family’s main concerns, reduces anxiety, and improves satisfaction. For example, if a parent reports that they expect their child to undergo additional diagnostic testing, this needs to be appreciated and addressed during the feedback.”
Validate Symptoms “Explicitly stating that you do not believe the child is “faking” or that the problem is merely due to psychological stress is critical”
Offer a Positive Diagnosis “Although you are special, your symptoms are not unique or mysterious…. If the focus is on what has been ruled out, there are always additional diagnoses that you, the patient, or the internet can introduce.”
Provide Education “it can be helpful to explain that chronic pain is like a fire alarm that keeps ringing although there is no fire. “
Emphasize a Multidisciplinary Intervention Plan plan for medical intervention, psychological support, and physical activity
Offer an Optimistic Appraisal “optimistic appraisals are most effective when a clinician has first validated a child’s pain, provided a positive diagnosis and education, and outlined an evidence-based, multidisciplinary approach to care”
My take: This article offers helpful advice. However, whether there is a “golden hour” of opportunity is not clear. Having better outcomes with early intervention could easily be related, at least in part, to selection bias.
Random blinded allocation (1:1) to either 30 mg lansoprazole (n=172) twice daily or matched placebo (n=174) twice daily for 16 weeks of patients with persistent throat symptoms.
Eligible patients had persistent (>6 weeks) unexplained throat symptoms—principally hoarseness, throat pain, globus sensation, throat clearing, postnasal secretions or excess mucus, cough, or choking sensation
Primary outcome was symptomatic response at 16 weeks measured using the total reflux symptom index (RSI) score.
Key finding:
No evidence was found of benefit from PPI treatment in patients with persistent throat symptoms. RSI scores were similar between the lansoprazole and placebo groups after 16 weeks of treatment and at the 12 month follow-up.
Improvements (reduction in RSI score) were observed in both groups—score at 16 weeks: lansoprazole 17.4 (15.5 to19.4) and placebo 15.6 (13.8 to 17.3). No statistically significant difference was found between the treatment arms. Furthermore, “no trends were in favour of lansoprazole.”
Limitation: “Our trial could be criticised for lacking any objective measure of GORD within the methodology or for employing any such test as an inclusion criteria. However, we did address the use of PPIs in an empirical setting, which was a near universal practice at the time of our study.”
My take (borrowed in part from authors): “No evidence supports the empirical use of PPIs to treat persistent throat and voice symptoms.” Despite this finding, “old habits die hard” and I predict that it will be a long time before this finding is widely adopted into clinical practice.
This prospective study followed the natural history of NAFLD in children with timed liver biopsy reassessment in children (n=122) using the placebo arms of 2 large multicenter clinical trials; patients received standard of care lifestyle advice. The study population had a mean age of 13 years; 71% were Hispanic participants
Key findings:
At enrollment, 31% of the children had definite NASH, 34% had borderline zone 1 NASH, 13% had borderline zone 3 NASH, and 21% had fatty liver but not NASH
Over a mean period of 1.6 ± 0.4 years, borderline or definite NASH resolved in 29% of the children, whereas 18% of the children with fatty liver or borderline NASH developed definite NASH
Fibrosis improved in 34% of the children but worsened in 23%
Progression was more likely with increasing ALT, increasing GGT, type 2 diabetes/increasing HgbA1c
Overall, one-third had histologic features of progression within 2 years, in association with increasing obesity and serum levels of aminotransferases and loss of glucose homeostasis.
The study conclusions are limited by selection bias, potential liver biopsy sampling errors, limited enrollment of non-Hispanic children, and relatively short duration of follow-up
A terrific review of sickle cell disease (SCD) associated liver problems: F Lacaille et al. JPGN 2021; 72: 5-10. The Liver in Sickle Cell Disease
While the most frequent liver-related problem in individuals is cholelithiasis (>25% after age 5 yrs), a host of other problems can develop –this article is a good reference.
~6% of children and 10% of adults develop severe liver complications of SCD
With sequestration, indications include pain with acute drop in hemoglobin (>2 g/dL)
Acute hepatic crisis is often signaled by elevated conjugated bilirubin
With severe liver disease/liver ischemia, authors advocated for exchange transfusion which “more efficiently decreases HbS percentage, faster restoring the blood flow than simple transfusion.” Consider after excluding biliary complication if INR is >1.4 with increased conjugated bilirubin (>3 mg/L). “Simple transfusion should be discussed in other cases.”
Cholangiopathy and autoimmune liver disease
Although autoimmune sclerosing cholangitis/autoimmune hepatitis are rare, it may account for 8% of children with SCD referred for hepatic dysfunction
Liver biopsy, needed for diagnosis, “is a dangerous procedure in SCD, which cannot be performed without at least a transfusion”
“Steroids can induce sickle crisis”
Look for ANA, SMA, LKM, and ANCA
Iron Overload
“It is not usually a significant concern in children…In our patients, the median ferritin level was about 3000 ng/mL, and none had a severe overload on MRI”
Infections/Drug toxicity
Need to consider hepatitis B, hepatitis C, and hepatitis E in particular
Inquire about herbal medicines and recreative drugs
Liver transplantation
Results are often poor.
Problems include sickle cell crisis in the transplanted liver, and drug toxicity which can add to the neurological and renal morbidities of SCD
Stem cell transplantation
Consider for severe complications of SCD including hepatic complications
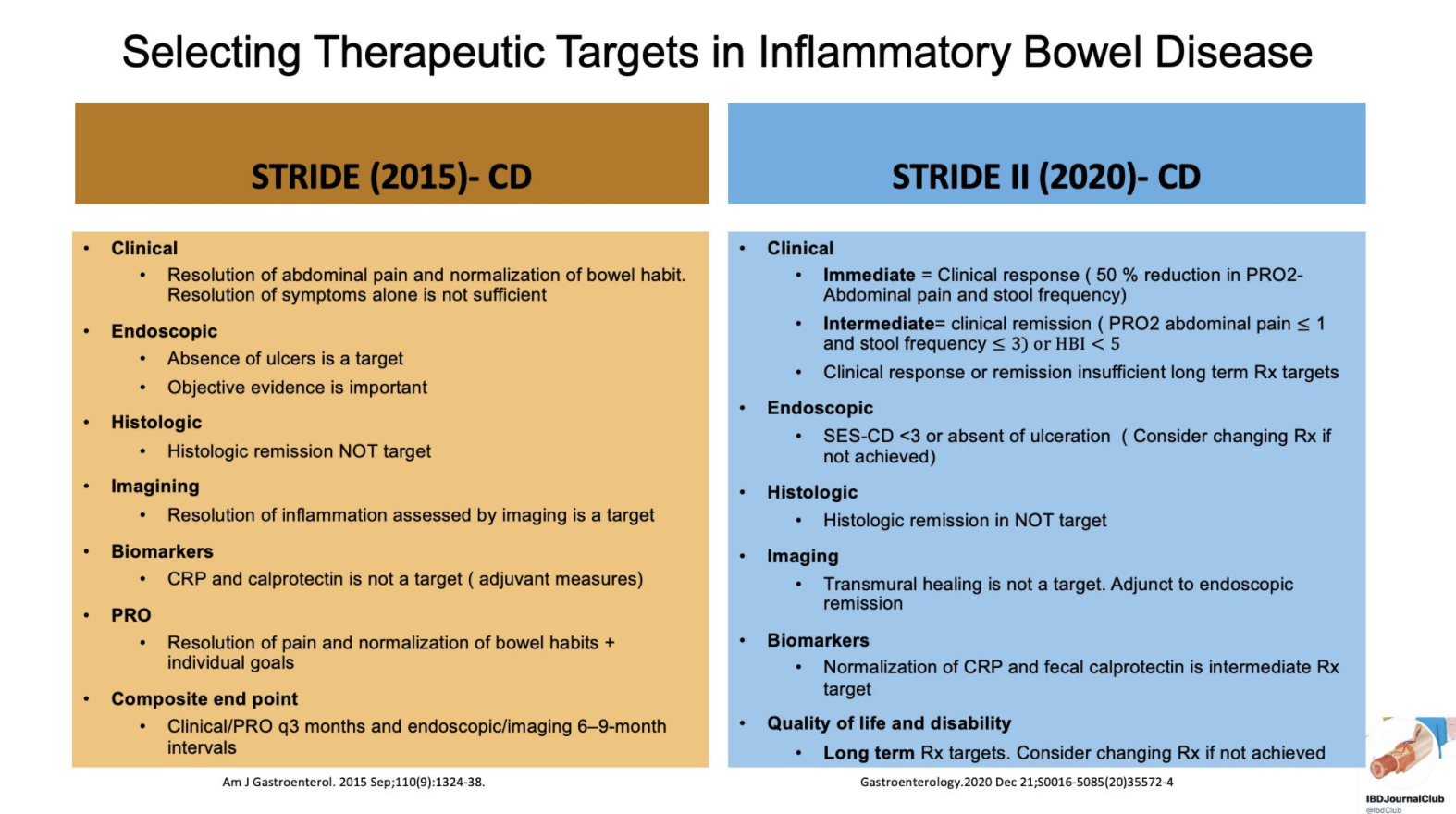
From Tauseef Ali’s Twitter Feed — a summary slide of Crohn’s disease targets for both pediatric and adult patients and a slide showing typical response/remission/healing times to medications.
Recommendations were based on a systematic review of the literature and iterative surveys of 89 IOIBD members, recommendations were drafted and modified in two surveys and two voting rounds.
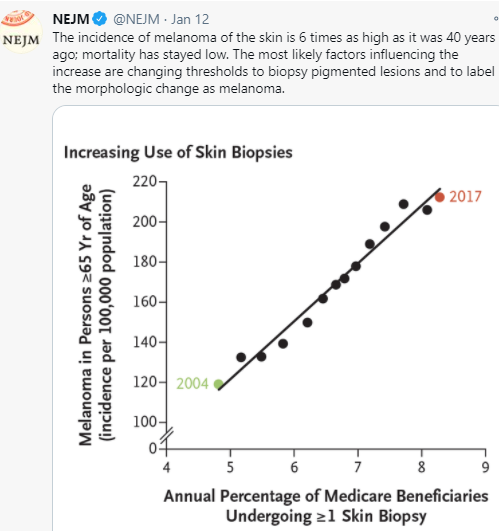
It would seem intuitive that screening for melanoma in at-risk pediatric patients would be worthwhile. And, this has been recommended in pediatric patients with inflammatory bowel disease who have received medications which increase the risk. However, a recent article (HG Welch et al. NEJM 2021; 384: 72-79. The Rapid Rise in Cutaneous Melanoma Diagnoses) provides a lot of reason to question this practice;. This article did not focus on pediatrics but its message about overdiagnosis of melanoma is applicable to this population as well.
Key points:
The increase in melanoma diagnosis (6-fold increase over 40 years) without a significant change in mortality (see Figure 4) indicates that the increase is primarily related to diagnostic scrutiny
This is driven by a fear of missing a diagnosis, medicolegal concerns and patient anxiety along with lower thresholds for referring to dermatology, lower thresholds for dermatologists to biopsy, and lower threshold by pathologists to diagnose melanoma
There are “no definitive diagnostic criteria for the pathological diagnosis of melanoma”
“The incidence of melanoma in situ is now 50 times as high as it was in 1975 (25 vs 0.5 per 100,000 population)…[yet there is a] lack of any appreciable effect in reducing the occurrence of invasive melanoma.”
Adverse consequences of unnecessary dermatology referrals: feeling vulnerable related to overdiagnosis of melanoma, increased costs, and difficulty obtaining life or health insurance
More “survivors” of melanoma overdiagnosis increase awareness of melanoma and can increase the cycle of overdiagnosis
My take: Routine visits to dermatology are difficult to justify in the absence of worrisome skin findings. “Although the conventional response has been to recommend regular skin checks, it is far more likely that more skin checks are the cause of the epidemic — not its solution.”
This articles serves as a good review of exocrine pancreatic insufficiency (EPI).
Etiologies:
“Cystic fibrosis is the most common cause of EPI in children .” Other congenital causes include aberrant embryonic development of the pancreas, “Shwachman-Diamond syndrome, Johanson-Blizzard syndrome, Pearson marrow pancreas syndrome, and Jeune syndrome”
“Acquired causes of EPI can be transient, such as in the aftermath of acute pancreatitis (which can persist weeks to months)”
Also, infants, compared to adults, have “physiological” EPI. Lipase output is 5–10% of adult values during the 1st 6 months of life.
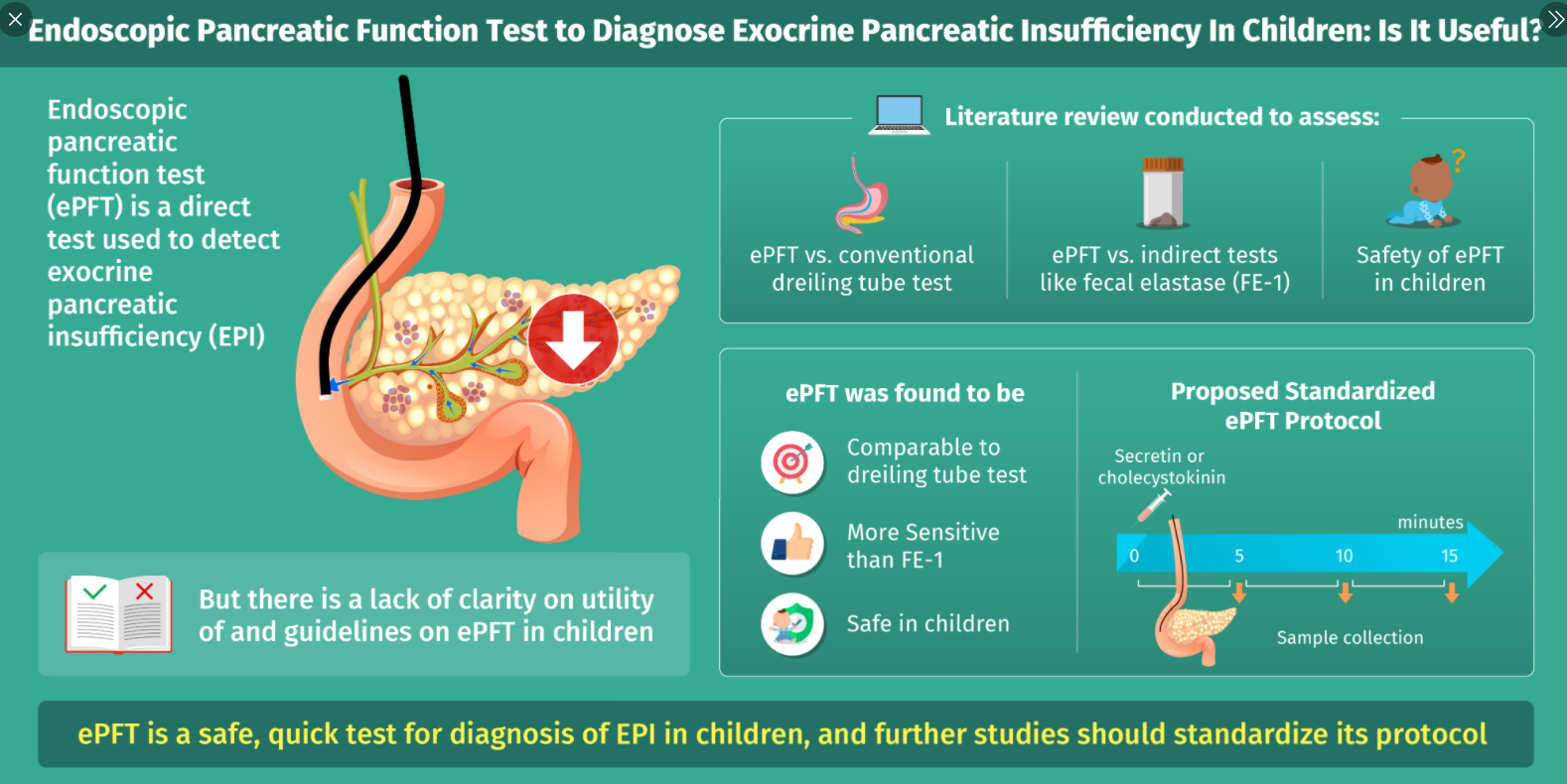
Advantages/Disadvantages of Endoscopic Testing for EPI:
Advantages:
• Safe, technically easy, and quick procedure to perform in conjunction to routine investigative EGD
• Allows assessment of acinar and ductal function
• High sensitivity and specificity in detection of isolated and generalized enzyme deficiencies
• Can diagnose minor and more severe degrees of EPI and aid in early diagnosis of CP in patients with unremarkable radiological changes
Disadvantages:
• Can be done only in conjunction with EGD and the patient will likely require sedation• Prolongs routine EGD
• Assesses peak enzyme activity and bicarbonate concentrations rather than total secretory capacity
• No standardized pancreatic fluid collection frequency or duration in pediatrics
• Lack of age-specific standardized reference ranges in pediatrics
Endoscopic Testing Caveats:
Any sample with a pH less than 7 may be unreliable as it is below the pH optimum of the enzymes and may reflect contamination with gastric fluid; however, ” the inability to increase pH, or bicarbonate, upon secretin stimulation may be reflective of loss of cystic fibrosis transmembrane conductance regulator (CFTR) function”
My take: With careful clinical judgement, endoscopic EPI testing is rarely needed. First of all, fecal elastase measurements can detect most patients with EPI. In addition, a lot of patients with poor growth and suspected malabsorption are too young for reliable endoscopic EPI testing.