Yesterday, I received two emails (first from Steven Liu) about an article in Science and today I’ve already seen this article is referenced in a CNN report:
New York Clinical Trial Quietly Tests Heartburn Remedy Against Coronavirus
Key points:
- In China, a review of ~6000 patients suggested lower mortality in those taking famotidine (not statistically significant)
- Famotidine may interfere with viral replication protease in the coronavirus based on computer modeling
- A randomized trial with IV famotidine (large quantities are not available) is underway in New York using 9 times the dose used for heartburn.
- The article notes that increased heart problems are common in those with reduced renal function
- “We still don’t know if it will work or not”
My take: Famotidine may be a hot commodity –at least until studies are completed. Based on experience with hydroxychloroquine, some of our patients may need to look for alternative acid blockers.
Related blog posts:
- NY Times: How Will We Know When to Reopen the Country? & Timely Tweets
- Hydroxychloroquine NOT Likely Effective
- COVID-19 Projections -IHME Data IHME Link: IHME Website for COVID-19 This post details the projected needs (ventilators, ICU beds) and projected mortality. Currently, peak of this pandemic in U.S. is anticipated to be April 16th.
- How to Do a Colonoscopic Polypectomy and U.S. COVID-19 Tracker NPR: Map: Tracking The Spread Of The Coronavirus In The U.S This tracker details the pandemic in every state.
- How to Protect Healthcare Workers from COVID-19 -Lessons from Hong Kong and Singapore Atul Gawande has a very pertinent article in the New Yorker: Keeping the Coronavirus from Infecting Health-Care Workers
- What is the Current Standard of Care for PPE and Endoscopy Cases? Link to manuscript: COVID-19 in Endoscopy: Time to do more?
- Bill Gates: What We Need to Do Now for COVID-19, False-negative testing & Article Describing 3 Stages of Infection From NY Times: If You Have Coronavirus Symptoms, Assume You Have the Illness, Even if You Test Negative Bill Gates: Here’s how to make up for lost time on covid-19 & article describing 3 stages of infection: COVD-19 Illness in Native and Immunosuppressed States: A Clinical-Therapeutic Staging Proposal
- Allocating Scarce Resources During COVID-19 Pandemic Links CDC Link: Testing for COVID-19 Full Link NEJM 2020 (Ezekial J Emmanuel et al): Fair Allocation of Scarce Medical Resources in the Time of Covid-19. This post also displays some data on sensitivity/specificity of testing
- Iron Injectables Links Financial Times: Coronavirus tracked: the latest figures as the pandemic spreads | Free to read & from Johns Hopkins: COVID19 Caseload & Outcomes Worldwide
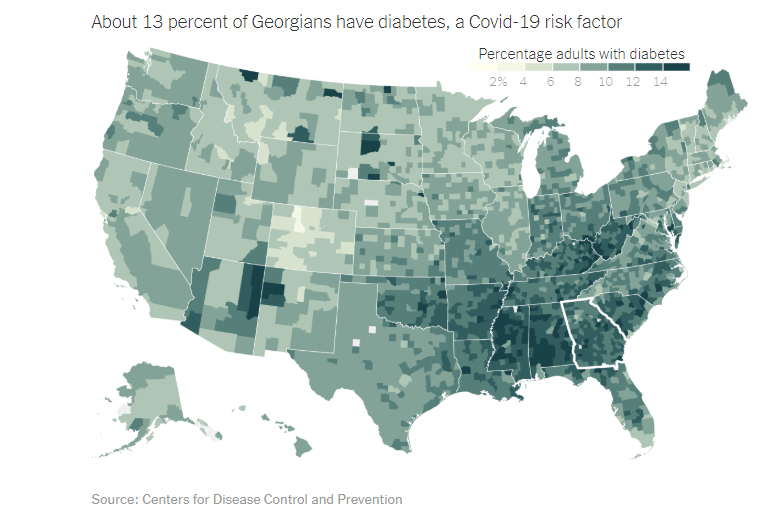
- COVID-19: Veneto vs. Lombardy and Georgia’s Part of this Pandemic Link: Harvard Business Review: Lessons from Italy’s Response to Coronavirus & Georgia DPH: COVID-19 Daily Status Report
- “Crushing It” Two More Pediatric Hepatitis C studies Full link from NY Times: How Long Will Coronavirus Live on Surfaces or in the Air Around You? and blog post shows how to properly place PPE
- Ethical Dilemmas and Digestive Symptoms –Common with COVID-19 Full link: NEJM: Facing Covid-19 in Italy — Ethics, Logistics, and Therapeutics on the Epidemic’s Front Line & digestive symptoms ACG: Full Link: ACG Media Statement
- More Advice on Coronavirus for Pediatric GIs: NASPGHAN and CCFA CCFA Guidance for Pediatric Caregivers and Patients —Updates on COVID-19 and IBD
- Autoimmune Hepatitis Outcomes, Grand Rounds on Splenomegaly, Hydroxychloroquine for SARS-CoV-2 & Zantac Warning
- Liver Shorts and COVID-19 Screenshots This post includes Fauci donuts, AJG reference on COVID-19 digestive symptoms, and technology to sterilized used PPE
- New: NEJM link to video demonstrating need for PPE during intubation -see picture at bottom of post. Fluorescent Spray During Intubation and at the bottom -there is an image showing how hydroxychloroquine and azithromycin could increase risk for life-threatening arrhythmias