These videos are on TikTok account. I do not have an account but was able to access this short video on my laptop (had trouble accessing on my mobile):
Methods: The study used the fourth Trøndelag Health Study (HUNT4), conducted in 2017–2019, where 56,042 adult (aged >20 years) residents of Nord-Trøndelag County, Norway, participated. Serum samples from 54,505 participants were analyzed for anti-transglutaminase 2 IgA and IgG.
Key findings:
The rate of CeD seropositivity was 2.0% (1107/54,505).
The total biopsy-confirmed prevalence of CeD was 1.5% (853/56,042).
The study confirmed a new CeD diagnosis after participation in HUNT4 in 470 individuals and a known CeD diagnosis before participation in HUNT4 in 383 individuals.
The ratio of new, previously undiagnosed CeD cases (after HUNT4) to known, previously diagnosed CeD cases (before HUNT4) was 1.2:1 (470/383).
My take: This study showed that the ratio of undiagnosed cases to diagnosed case of CeD was improved from previously in Norway.
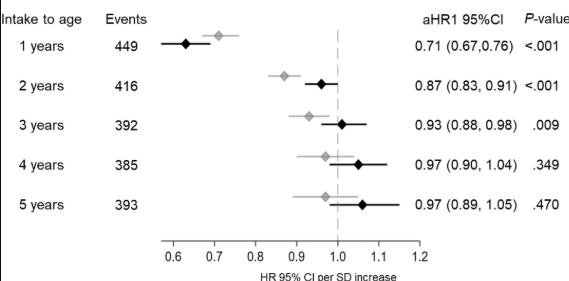
Methods: This study examined the quantity and timing of dietary fiber intake in children up to 5 years of age who were at genetic risk for celiac disease, assessing its relationship with their subsequent risk of developing the condition. The analysis included 6520 children carrying the HLA-DQ2 and/or DQ8 risk haplotypes who were prospectively followed for a total 61,669 person-years to age 13 years in The Environmental Determinants of Diabetes in the Young (TEDDY) study.
Key findings:
Dietary fiber intake from 6 months to 3 years of age was inversely associated with the subsequent risk of celiac disease in models unadjusted for the concurrent gluten intake and to 2 years of age in models adjusted for gluten intake (Figure 1A). In contrast, no association was observed between dietary fiber intake to 4 and 5 years of age and the risk of celiac disease regardless of whether models accounted for the gluten intake.
My take: Higher dietary fiber intake during the first 2 years of life was associated with a lower risk of celiac disease in children at genetic risk. Although this effect was modest, it was independent of gluten intake and other components found in fiber-rich foods in the child’s diet.
P Singh et al. Gastroenterology 2025; 168: 1128-1136. A Novel, IBS-Specific IgG ELISA-Based Elimination Diet in Irritable Bowel Syndrome: A Randomized, Sham-Controlled Trial
Background (from editorial): “Biomarkers that correspond with the distinct pathophysiological disturbances that underlie food sensitivity, and that can be used to monitor and guide management or predict response to food elimination are lacking…Previous studies have suggested a role for IgG-mediated food sensitivities in driving IBS symptoms.12 However, the role of IgG testing and subsequent dietary elimination for the management of IBS symptoms remains a subject of debate. Elevated IgG levels have been observed in healthy individuals, indicating that these antibodies may reflect a physiological response to dietary exposure rather than intolerance or sensitivity to a specific food.”
In this study, the researchers used a proprietary IgG-based sensitivity testing (“inFoods IBS” ELISA) from the company sponsor, Biomerica. This was a randomized, double-blind, sham-controlled trial enrolling subjects with IBS from 8 centers. Subjects positive for ≥1 food on an 18-food IgG assay. 223 were included in the modified intention-to-treat analysis. The primary outcome was a ≥30% decrease in abdominal pain intensity for ≥2 of the last 4 weeks of the treatment period.
Key findings:
A significantly greater proportion of subjects in the experimental diet group met the primary outcome than those in the sham diet group (59.6% vs 42.1%, P = .02).
Subgroup analysis revealed that a higher proportion of subjects with constipation-predominant IBS and IBS with mixed bowel habits in the experimental diet group met the primary endpoint vs the sham group (67.1% vs 35.8% and 66% vs 29.5%, respectively).
Discussion Points:
The authors claim the following: “Because IgG-based antibodies to foods can be elevated in healthy controls, it is important to develop disease-specific assays. The assay used in our study was developed specifically for patients with IBS and uses cutoff values derived from healthy controls.”
Limitations:
“Adherence was poor. Of those who filled out the dietary diary as instructed, 35% were nonadherent in the intervention group and 42% nonadherent based on a yes to an adherence question on ≥80% of days over the 12-week trial.” Adherence was higher in the sham control.
“Second, in a per-protocol analysis that included only the adherent participants, the clinical outcomes are much less impressive for the IgG-based elimination diet, raising critical questions as to whether other factors were responsible for the improvement in symptoms in the full dataset.”
Possible confounding bias: “2 of the 3 most commonly eliminated foods in the IgG-based elimination diet were high in FODMAPs (eg, milk, wheat), whereas all 3 most commonly eliminated foods in the sham diet were low in FODMAPs (poultry, rice, and goat cheese).”
The authors noted that it was unexpected that the response was more robust in the IBS-C and IBS-M groups rather than the IBS-D groups.
The company sponsor has had good success in publicizing their results on ABC, CBS and NBC. Here is a link from their website direct to YouTube. It highlights a specific young woman reporting success with this approach and commentary by one of the lead authors: inFoods IBS Finding Trigger Foods Faster.
My take: While most patients are eager to pinpoint trigger foods, I remain skeptical about this “precision testing for IBS.” There is no data indicating that this IgG-based diet outperforms patients who limit dairy and wheat, two common triggers. I agree with the associated editorial: “The clinical efficacy of IgG-based elimination diets will need further evaluation before they are implemented in routine clinical practice.”
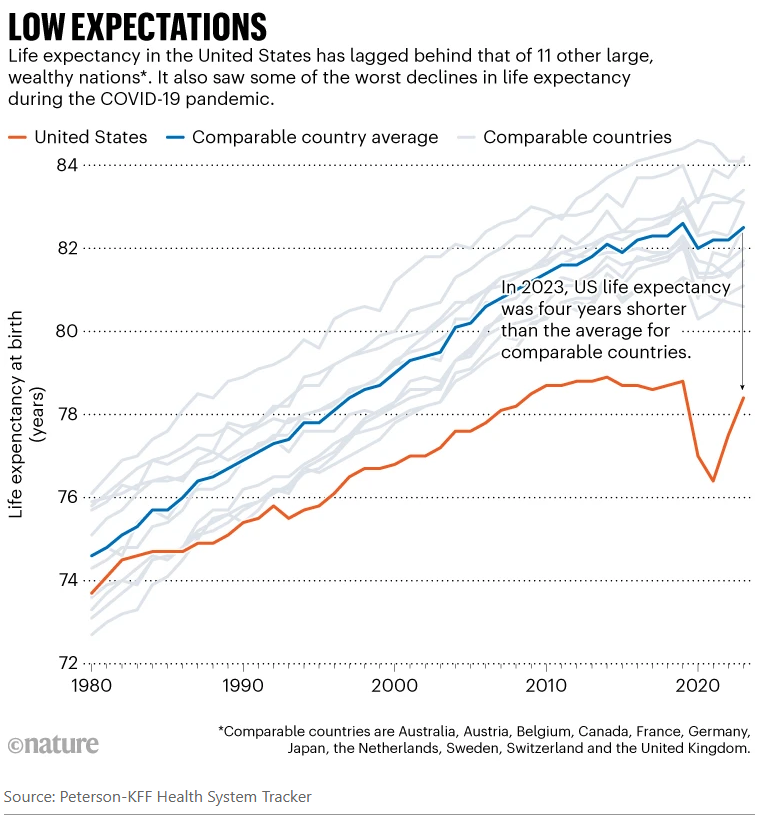
Since taking over as the top US health official in February, Robert F. Kennedy Jr has overseen radical changes that have alarmed many public-health experts…His mission, he says, is to ‘Make America Healthy Again’. “We are the sickest nation in the world,” he said in March, “and we have the highest rate of chronic disease.” His diagnosis holds some truth, say public-health specialists and analysts. Relative to other similarly wealthy nations, the United States has the shortest life expectancy despite spending the most on health care…And researchers agree that high rates of chronic disease, including heart disease and obesity, are key contributors to Americans’ higher death rates, as Kennedy emphasizes.
But researchers say that Kennedy — widely known as RFK Jr — has mostly ignored other leading causes of death and ill health, including car accidents, drug overdoses and gun violence…
Life expectancy in the United States was closer to the average for its peers around 1980 and gradually improved, according to KFF’s analyses. The gains were driven partly by a drop in smoking and increased use of cholesterol-lowering drugs known as statins…
Overall, chronic conditions — heart disease, cancer, stroke and respiratory disease — take up four out of five spots on the country’s list of biggest killers…One of the biggest drivers of those deadly conditions is obesity, say researchers. As of 2022, about 42% of adults were considered obese in the United States, compared with 27% in the United Kingdom and 5.5% in Japan. Obesity increases the risks of developing diabetes, heart disease, cancer and many other conditions. “The US has, particularly around diet, obesity and overweight, adopted unhealthier lifestyles at a higher rate than our country peers,” Bollyky says…
The problems caused by chronic disease are compounded by poor health care. Compared with a group of similar high-income countries, the United States is the only one that lacks universal health-insurance coverage… Lack of health insurance, high costs and other barriers prevent people from getting diagnoses and treatment early on…
The other big contributors to lower life expectancy in the United States — and what really sets the country apart, researchers say — are high death rates from substance misuse, car accidents, suicide and homicide (see ‘Varied causes’). These tend to kill people of working age…All told, the death rates in working-age people mean that one 5-year-old out of every 20 — or roughly one in every school class — will die before the age of 45, according to Angus’s calculations. The comparable figure is one in 50 in the United Kingdom and one in 100 in Switzerland…
Health spending in the United States was about US$13,000 per person in 2023, according to a KFF analysis. That compares to an average of about $7,000 per person in similar large, well-off countries…
Boosting rather than cutting spending on disease prevention is “where the big gains are to be made on population health” [Reginald Williams, a health-policy specialist at the Commonwealth Fund says his] first priority would be to expand health coverage. In the United States, around 8% of people lack health insurance, compared with around 1% or less in similar high-income countries. The second, he says, would be to invest more in primary care — the physicians and other health professionals who are the first port of call for patients, and who deal with disease prevention and management…
Tackling the high death rates from overdoses and guns, meanwhile, would involve addressing entrenched social and political issues such as gun ownership, poverty, unemployment and inequality.
My take: Despite big promises from politicians, there are no quick fixes for improving our national health. Improving health care access would help but this does not address deaths due to firearms, drug overdoses and to car accidents.
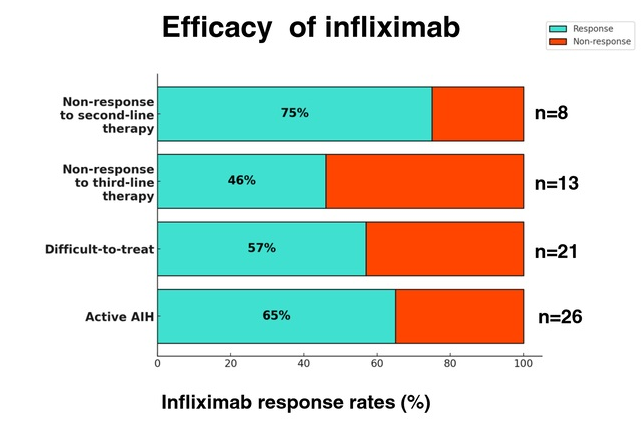
In this multicenter retrospective study, there were two groups of patients with autoimmune hepatitis (AIH) who received infliximab treatment:
Group 1 (n=20) had failed standard, second-line (mycophenolate mofetil and 6-mercaptopurine) or third-line (tacrolimus or cyclosporine) therapy.
Group 2 (n=22), infliximab was given for treatment of concomitant extrahepatic autoimmune diseases. Only 6 of these patients had active AIH at time of initiation of infliximab therapy
Key findings:
Overall, 65% (17/26) of the patients with active AIH achieved complete biochemical remission* (CR) on infliximab. This included CR in 75% (6/8) of nonresponders to second-line and in 46% (6/13) of failing third-line therapy.
*CR defined as normalization of serum transaminases and IgG levels
Five patients developed anti-infliximab antibodies, 1 had an allergic reaction and 4 had a lack of control of a concurrent autoimmune disorder, prompting discontinuation of infliximab
My take: While a randomized controlled trial would be better, this study demonstrates that infliximab is an option for AIH, especially in those with concurrent immune-mediated disorders and in those not responding to standard therapy. It is worth noting that infliximab can paradoxically induce an autoimmune hepatitis and stopping infliximab therapy can be curative in these patients (we recently had such a case).
Autoimmune Hepatitis Associated with Anti-TNF Therapy Serious liver injury related to anti-TNF therapy is rare. A great place to understand the spectrum of liver problems potentially related to infliximab is the livertox website
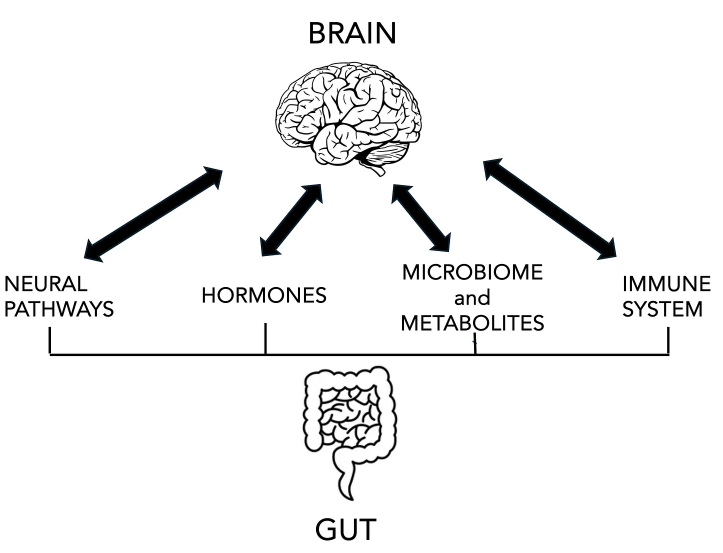
Eric Topol has summarized some of the recent advances in the understanding of the Gut-Brain Axis. Open Access Link: The Gut-Brain Axis Takes Center Stage (6/22/25)
Here’s a lengthy excerpt:
We’ve known about the gut-brain axis for decades but there has recently been an unprecedented jump in our knowledge base that has transformed our expectations for its preeminence.
There are 2 types of neural pathways, the “second brain” referring to the enteric (gut) nervous system from the cells that line the intestine and communicate to the vagus nerve to the brain (and in the opposite direction, too). There are also connections via the sympathetic, parasympathetic nervous system (autonomic nervous system, ANS) branches and spinal cord innervation to the gut primarily through the ANS.
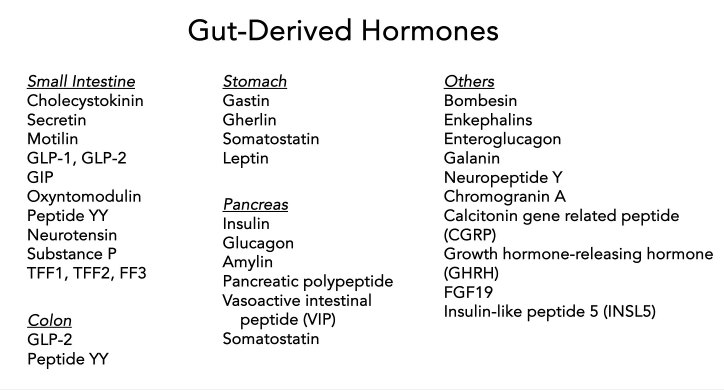
Cells in the gut produce hormones (enteroendocrine cells) such as glucagon-like peptide (GLP-1), gastric inhibitory peptide (GIP), peptide YY, secretin, gherlin, gastrin, and many others. Some of these regulate pancreatic hormones such as insulin, glucagon and amylin, which can be considered as gut hormones but derived from pancreatic cells rather than intestinal lining cells. The hormonal interaction between gut and brain also goes through the hypothalamus-pituitary-adrenal (HPA) axis.
The interaction with the immune system is critical to maintain integrity of the gut lining (avoiding “leaky gut syndrome”) and the blood-brain-barrier…
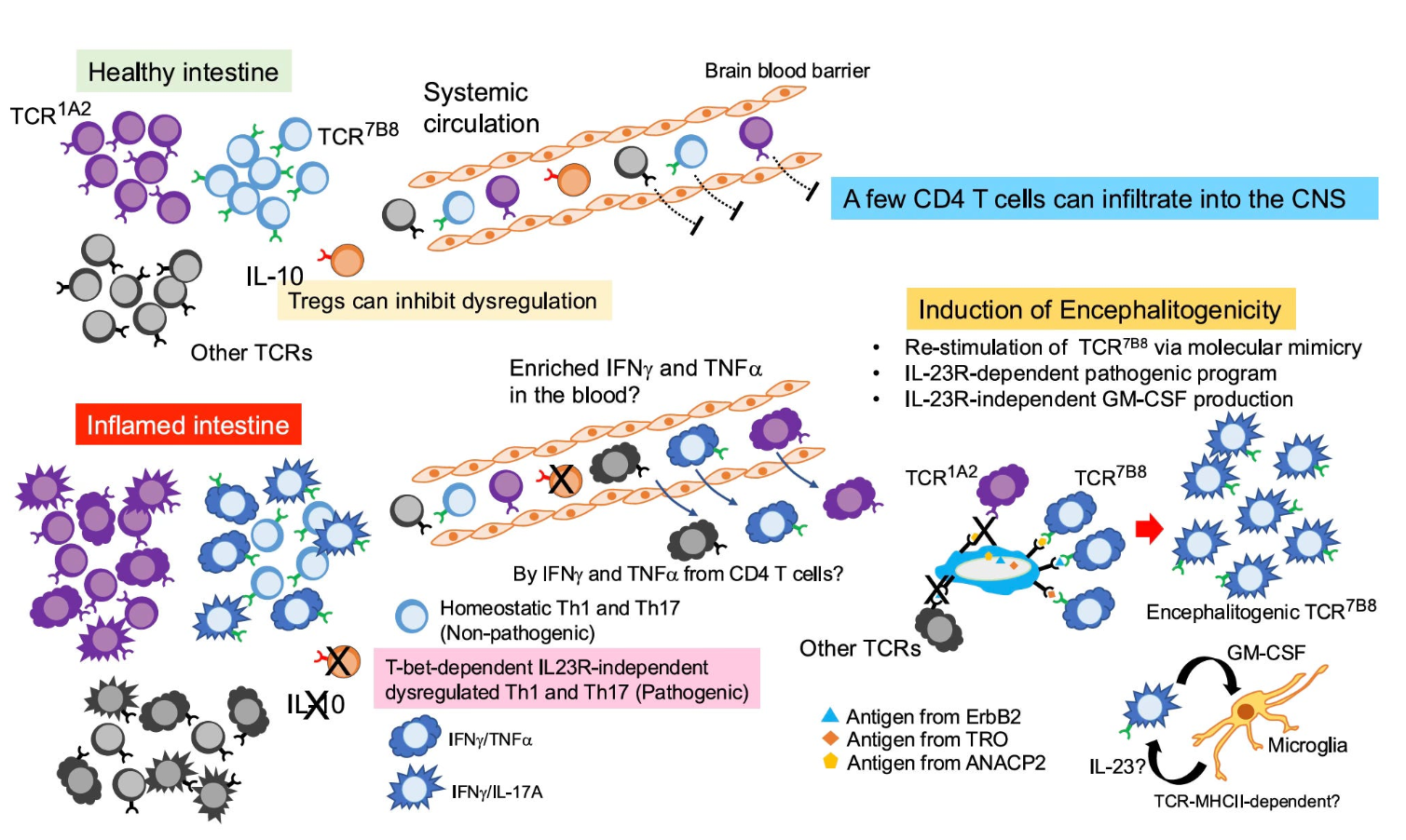
The precise way by which the gut can induce inflammation in the brain has remained unclear. In the journal Nature this week it was shown that inflamed gut-derived CD4+ T cells can infiltrate the brain, leading to neuroinflammation and neurological damage in the experimental model…bacteria derived proteins (antigens) looking like host derived proteins, inciting an immune response.
This was the second of 2 recent discoveries centered around gut-derived immune cells that get into the brain. Newly identified specialized CD4+ T cells from the gut and white adipose tissue establish residence in the brain’s subfornical organ and regulate feeding behavior…
It turns out the H. pylori can do good things too! As in blocking the formation of amyloid protein formation. This week in Science Advancesit was demonstrated that H. pylori releases the protein CagA (cytotoxin-associated gene A) which potently inhibits pathogenic amyloid assemblies..for formation in Alzheimer’s disease, Parkinson’s disease and type 2 diabetes…
Several new gut hormone clinical trials, beyond the ones that are widely used—semaglutide (Ozempic) and tirzepatide (Zepbound, Mounjaro), were unveiled…Through randomized trials, their broad impact has been unequivocally proven for diabetes, obesity, and for treating related conditions of heart failure (with preserved ejection fraction), kidney disease, liver disease, sleep apnea, along with unexpected suppression of addiction to alcohol, cigarette smoking, nail biting and gambling. Add a surprising impact that we’re starting to see for autoimmune diseases. Even before there is weight loss with these drugs, there is evidence from experimental models of reduced systemic (body-wide) and brain inflammation. What is surprising is that drugs like semaglutide have little direct penetrance to the brain, but exert their effect chiefly through the gut-brain axis. New molecules in this class will have enhanced brain penetrance…
Will They Work For Alzheimer’s Disease?
[In a Liraglutide trial with 200 participants with Alzheimer’s,] after 1 year of treatment there was a reported 18% less cognitive decline and 50% reduced brain shrinkage compared to placebo…[There are also two studies] pending EVOKE and EVOKE Plus trials of daily oral semaglutide participants aged 55–85 years with mild cognitive impairment or mild dementia due to Alzheimer’s…About 12% of American adults are already taking GLP-1 drugs
Earlier this year, as President Donald Trump was beginning to reshape the American government, Michael, an emergency room doctor who was born, raised, and trained in the United States, packed up his family and left the country…”Part of being a physician is being kind to people who are in their weakest place,” Michael said. “And I feel like our country is devolving to really step on people who are weak and vulnerable…”
The Medical Council of Canada said in an email statement that the number of American doctors creating accounts on physiciansapply.ca, which is “typically the first step” to being licensed in Canada, has increased more than 750% over the past seven months compared with the same time period last year — from 71 applicants to 615. Separately, medical licensing organizations in Canada’s most populous provinces reported a rise in Americans either applying for or receiving Canadian licenses, with at least some doctors disclosing they were moving specifically because of Trump…
While it was once more difficult for American doctors to practice in Canada due to discrepancies in medical education standards, Canadian provinces have relaxed some licensing regulations in recent years, and some are expediting licensing for U.S.-trained physicians…
Michael, the physician who moved to Canada this year, said he had long been wary of what he describes as escalating right-wing political rhetoric and unchecked gun violence in the United States, the latter of which he witnessed firsthand during a decade working in American emergency rooms…
This desire to leave has also been striking to Hippocratic Adventures, a small business that helps American doctors practice medicine in other countries…
Alison Carleton, a family medicine doctor who moved from Iowa to Manitoba in 2017, said she left to escape the daily grind of America’s for-profit health care system and because she was appalled that Trump was elected the first time.Carleton said she now runs a small-town clinic with low stress, less paperwork, and no fear of burying her patients in medical debt.
My take: There are more than one million physicians in the U.S. per AAMC data; so the absolute numbers leaving are quite small. However, this uptick in physicians leaving is another indicator of U.S. physicians being unhappy with U.S. healthcare policy and the direction in which it is headed.
Throughout the United States, PCPs have been leaving traditional practices for concierge and direct primary care (DPC) practices, in which patients are offered personalized and more accessible primary care in exchange for membership or retainer fees… these models can offer physicians notable advantages over traditional primary care models, including greater clinical autonomy, more take-home pay, and improved work–life balance and job satisfaction.4,5 Less burdened by prior authorizations, insurance denials, billing and coding tasks, and other demands in traditional practices — including the need to adhere to regulatory requirements under alternative payment models — physicians often have more time for direct patient care...Yet trade-offs — in the form of decreased access for patients [without a concierge physician] and increased strain on PCPs in traditional primary care — are borne by the rest of society.
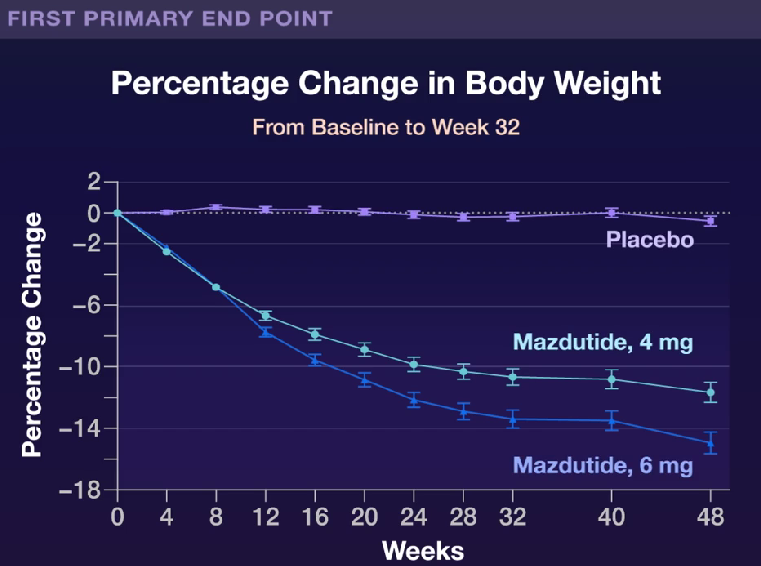
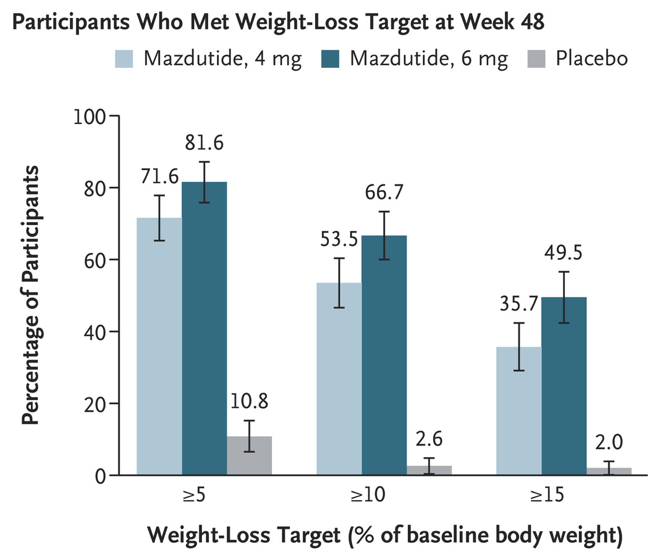
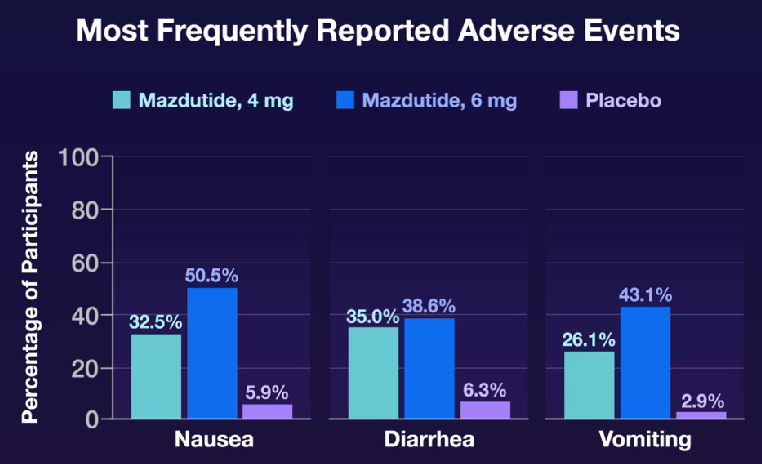
L Ji et al. NEJM 2025; 392: 2215-2225. Once-Weekly Mazdutide in Chinese Adults with Obesity or Overweight
This study from China enrolled young participants (mean age 34 yrs) and lower BMI (mean 31.1) than in similar studies of other GLP1 RAs and GLP 1 RA/GIP dual agonists. However, there was a high prevalence of dyslipidemia (62.3%), MAFLD (48.9%), hyperuricemia (40.2%), and hypertension (22.8%).
Key findings:
At week 48, the mean percentage change in body weight from baseline was –11.00% in the 4-mg mazdutide group, –14.01% in the 6-mg mazdutide group, and 0.30% in the placebo group
My take: Mazdutide resulted in significant weight loss along with improvements in cardiometabolic measures. This study shows beneficial effects in a younger cohort with significant cardiometabolic disease. Improvements in younger populations is likely to result in more substantial effects on outcomes than improvement in older cohorts.
Background: “Etrasimod is an oral, once-daily, selective S1P1,4,5 receptor modulator for the treatment of moderately to severely active ulcerative colitis and in development for the treatment of other immune-mediated inflammatory diseases. Etrasimod prevents trafficking of lymphocytes to inflamed mucosal tissue and sites of primary disease manifestation, offering a unique, promising mechanism for the treatment of eosinophilic oesophagitis.”
There were 108 participants in this study: 41 patients received etrasimod 2 mg, 39 received etrasimod 1 mg, and 28 received placebo.
Key findings:
Median percentage changes from baseline in peak eosinophil count (PEC) at week 16:6 were −58·4% for etrasimod 2 mg (p=0·010 vs placebo), −39·4% for etrasimod 1 mg (p=0·29 vs placebo) and −21·5% for placebo.
Significant reductions from baseline in oesophageal PEC were achieved with both etrasimod doses (n=27 for 2 mg n=28 for 1 mg) at week 24 versus placebo (n=19), with a numerically larger reduction seen with the 2 mg dose, which had a median placebo-adjusted difference of –103·9% from baseline in oesophageal PEC. Oesophageal PEC did not decrease further with longer etrasimod treatment during the extension period (to 52 weeks in a smaller subset)
Etrasimod 2 mg was associated with a significant improvement in DSQ score at week 24 versus placebo in patients with no history of dilation (LS mean −21·6 vs –9·6, p=0·031)
No serious treatment-emergent adverse events occurred.
My take (borrowed from the authors): “This [phase 2] study provides the first evidence that targeting the S1P pathway can improve disease activity in eosinophilic oesophagitis. Given that current treatment options for eosinophilic oesophagitis have variable and incomplete response rates, etrasimod presents a promising option.” Larger studies are warranted.
I Mansuri et al. J Pediatr Gastroenterol Nutr. 2025;80:988–997. Clinical outcomes of maintenance therapy with sulfasalazine compared to 5-aminosalicylates in children with ulcerative colitis
Methods: This was a retrospective review of children diagnosed with UC between June 1999 and December 2019 at Boston Children’s Hospital. 124 started on sulfasalazine (SZ) and 309 on 5-aminosalicylates (5-ASA). Most patients had mild to moderate disease based on PUCAI score; ~12% had severe disease.
Key findings:
At 1 year, 54%, 44.3%, and 36.6% of patients on SZ, 5-ASA, and those who switched, respectively, were in steroid-free remission (p = 0.13)
All medication switches due to adverse reactions (24) were from SZ to 5-ASA. No patient was switched from 5-ASA to SZ because of adverse reactions. The non-severe adverse reactions noted were nausea, vomiting, abdominal pain, non-severe skin rash, headache, mild leucopenia, and lymphadenitis. Three patients had serious skin reactions, and one had pancreatitis.
SZ tended to have more minor adverse reactions. Except for countering adverse reactions, switching between SZ and 5-ASA did not offer therapeutic benefits. Disease severity at diagnosis predicted early treatment escalation
Discussion Points:
SZ offers advantages such as lower cost and availability in suspension form; the suspension form is particularly beneficial for young children and those unable to swallow the solid form of medication.
5-ASA formulations can be almost 10–50 times more expensive than SZ. For example, the wholesale acquisition cost of monthly generic SZ is $30 compared to $274 for generic Lialda, $1131 for generic Pentasa, and $1890 for generic Asacol HD
My take: About 20% of patients had to switch from Sz to 5-ASA due to adverse reactions; though, Sz had a mildly higher response rate (not statistically-significant). Switching between SZ and 5-ASA or vice versa is unlikely to provide much therapeutic benefit; patients who switched agents for medical reasons (rather than reactions) were more likely to require escalation to either a biologic or immune modulator.