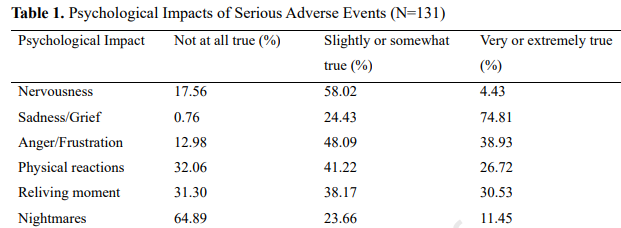
Background: “Serious adverse events (SAEs) are unavoidable occurrences for those performing complex endoscopic interventions. These affect not only the patient (the first victim), but also possibly the proceduralist (the second victim). Second victim syndrome (SVS) was first described by Dr. Wu detailing the negative psychological effects of adverse patient events on physicians (Ref: Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727).”
Methods: Survey responses form “X” platform (n=195) were collected in 2023. Only responses from advanced endoscopists (defined as those who perform either endoscopic ultrasound or endoscopic retrograde cholangiopancreatography annually) and advanced endoscopy fellows were included.
Key findings:
Higher procedural volume (>1000/year) was associated with feelings of greater emotional preparedness for SAEs
Speaking with colleagues (53%), exercise (33%), discussions at conferences (17%) and meditation (8%) were rated as used and very or extremely helpful
Discussion Points: “Peer support programs have proven to be well received and highly utilized. Additionally, surgeons criticize the often-punitive handling of SAEs, and note that the tone and culture in the review process following an SAE dictates reduction or exacerbation of SVS.”
My take: When I have had a complication in a patient, speaking with colleagues has provided a lot of support. One book I have recommended to others is the following: Complications: A Surgeon’s Notes on an Imperfect Science by Atul Gawande.
I was recently listening to a radio program (On Point) about the beneficial effects of sunlight.
The program notes that the potential beneficial effects of sunlight are much greater than the risks. Increased sunlight has been associated with lower rates of death, as well as lower rates of cardiovascular disease and autoimmune conditions like multiple sclerosis, type 1 diabetes, and Crohn’s disease.
When dermatologists recommend avoiding sunlight, they may be focused on the risks but not the benefits (though this varies among individuals). In addition, despite the more than 5-fold rise of melanoma diagnosis (especially in wealthy communities), there has not been a change in the rate of deaths due to melanoma. Skin cancers associated with sun exposure are mainly basal cell tumors and squamous cell tumors. These non-melanoma skin cancers have excellent survival rates.
Here is a link: The Healing Power of Sunlight (48 minutes) The most important part of this is in the middle, starting around 20 minutes.
My take: It’s a good idea to avoid sunburns but getting sunshine is good for health.
Related article:
Environ Epidemiol 2025. 9(3):e401. doi: 10.1097/EE9.0000000000000401. The association between time spent outdoors during daylight and mortality among participants of the Adventist Health Study 2 Cohort. Conclusion: “Moderate time outdoors in daylight during warmer months could be associated with lower risks of all-cause, CVD, and noncancer non-CVD mortality”
From AGA Today (8/5/25): “Sterile Water is Unnecessary for Endoscopy”
GI and Hepatology News (8/4, Pass) reports a review suggests that “endoscopists can safely forgo sterile water in favor of tap, reducing both environmental and financial costs.” Researchers found that only two studies since 1975 “directly compared sterile and tap water use in endoscopy,” and “neither showed an increased risk of infection from tap water. In fact, some cultures from allegedly sterile water bottles grew pathogenic bacteria, while no patient complications were reported in either study.” Current guidelines “recommend sterile water for procedures involving mucosal penetration but acknowledge low-quality supporting evidence.” However, they pointed out that “these recommendations are based on outdated studies, some unrelated to GI endoscopy.” Furthermore, the “review estimates that the production and transportation of sterile water bottles contributes over 6,000 metric tons of emissions per year from US endoscopy units alone.” The review was published in Gastro Hep Advances.
“With a conservative estimate of using half of a 1-L sterile bottle for irrigation per endoscopy, 22 million yearly endoscopies in the US could result in an additional 6000 tons of eCO2.”
Economic Costs:
“A 1-L bottle of sterile water costs $3–$10. For an endoscopy unit performing 30 procedures daily and a conservative estimate of half a water bottle per case, the average monthly direct costs could be $1000–$3000”
Discussion:
“There is no direct supporting evidence for using sterile water during endoscopy…a Cochrane review show no difference in infection risk when using tap or sterile water to irrigate wounds…Similarly, there is no benefit in using sterile water for enteral feeds in immunosuppressed patients, and tap water enemas are routinely acceptable for colon cleansing before sigmoidoscopies in all patients, irrespective of immune status.
My take: Plastic water bottles in endoscopy centers contribute to health-care waste, climate change and increased costs.
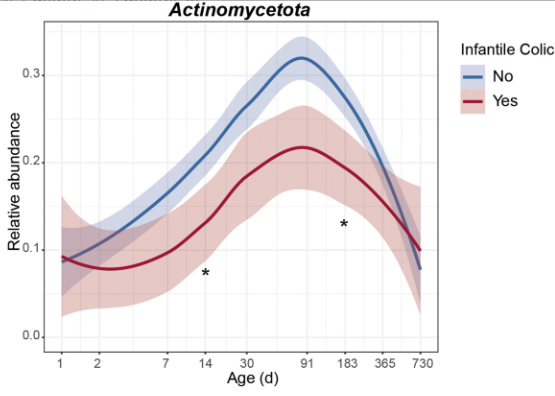
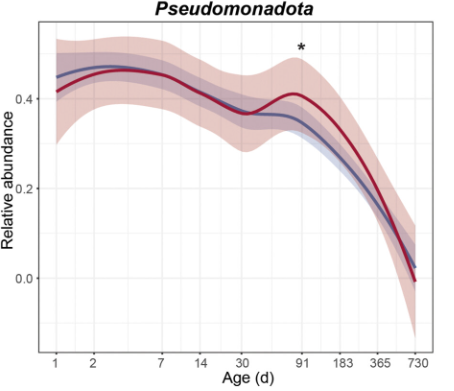
E Van Daele et al.J Pediatr Gastroenterol Nutr. 2025;81:217–225. Aberrant microbiota signatures precede symptomdevelopment in infantile colic
My take: There has been an interest in altered microbiome and colic for a long time. Whether these alterations are causally-related to colic and whether there is a way to treat these alterations remains unclear.
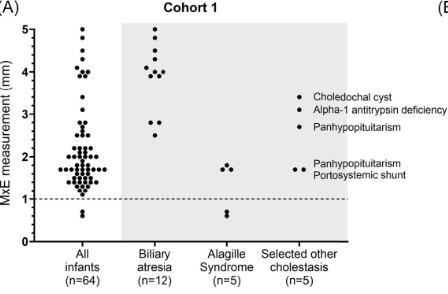
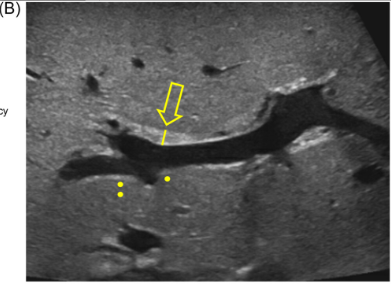
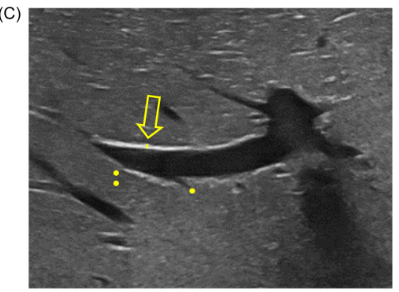
AM Upton et al. J Pediatr Gastroenterol Nutr. 2025;81:212–216. The “maximum echogenicity” at the right portal vein: Biliary atresia versus Alagille syndrome
Background/Methods: One way clinicians can distinguish between biliary atresia and Alagille syndrome is with a positive “triangular cord sign.” This ultrasound finding refers to a thickened echogenicity at the anterior aspect of the right portal vein…the maximum echogenicity at the anterior aspect of the right portal vein (“maximum echogenicity” or “MxE”) was measured in a group of infants with cholestasis (Cohort 1, n=64) and in another group of infants with Alagille syndrome (Cohort 2, n=30).
Key findings:
“Thin echogenicity at the anterior aspect of the right portal vein may help distinguish between biliary atresia and Alagille syndrome…None of the 12 infants with biliary atresia in Cohort 1 had a MxE < 1.0 mm”
“A MxE < 1.0 mm could help identify Alagille syndrome. 2 of the 64 infants with cholestasis in Cohort 1 had a MxE < 1.0 mm. Both infants were eventually diagnosed with Alagille syndrome. In the Cohort 2 infants with Alagille syndrome, 16 of 30 infants had a MxE < 1.0 mm”
Infant with biliary atresia Infant with Alagille Syndrome
Discussion Point:
“Infants with Alagille syndrome can have smaller bile ducts which may be inapparent on invasive testing such as cholangiography. As a result, they may be presumptively diagnosed with biliary atresia and inappropriately treated with the Kasai portoenterostomy. Unfortunately, these infants have poorer outcomes compared to infants with Alagille syndrome who do not receive the Kasai portoenterostomy.” Thus, distinguishing Alagille from biliary atresia is very important.
My take: This study shows that MxE (a refinement of what has previously been called the triangular cord sign) on ultrasound may help distinguish biliary atresia from Alagille syndrome. As this is a single-center study, it will be important to determine if this ultrasound finding can be replicated in other centers and whether the finding is operator-dependent.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
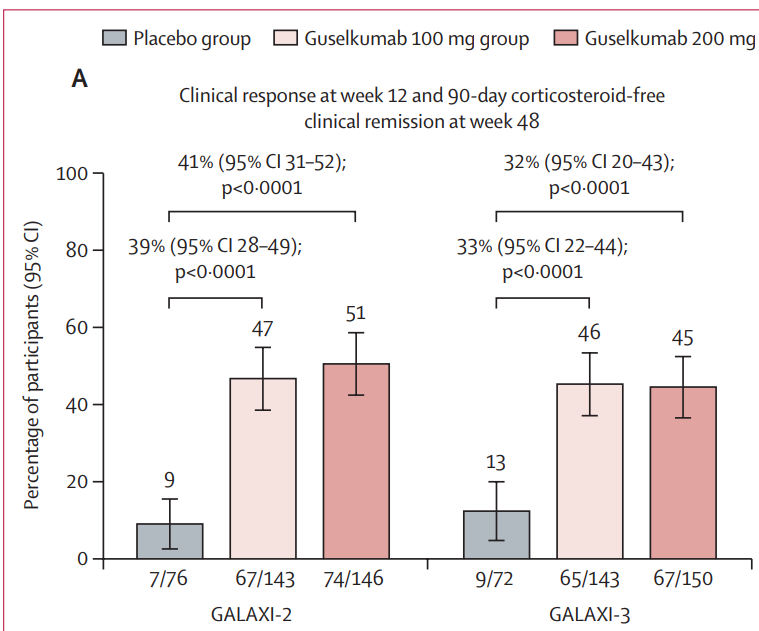
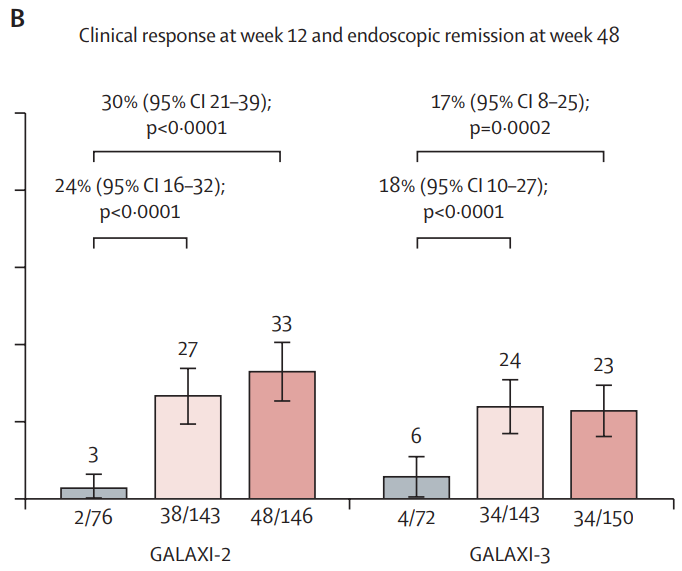
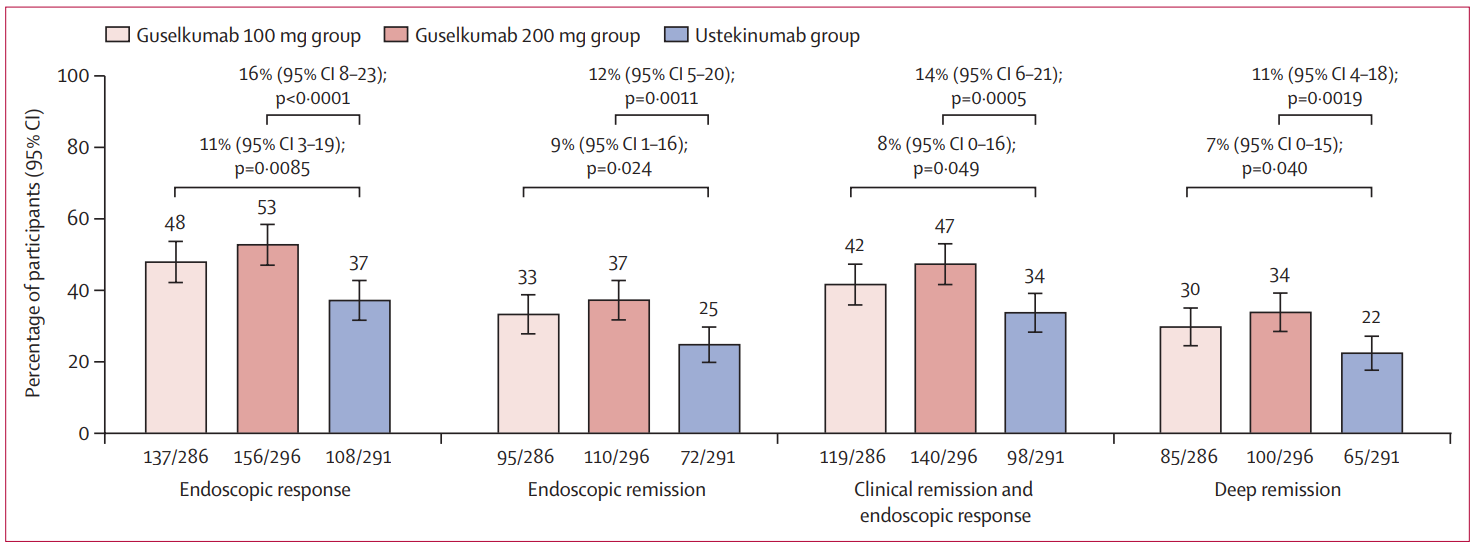
Methods: “GALAXI-2 and GALAXI-3 were identically designed, phase 3, randomised, double-blind, triple-dummy, treat-through trials with active and placebo comparators…1048 participants were randomly assigned, treated, and followed up until week 48, of whom 1021 participants were included in the primary analysis population: 508 (49·8%) in GALAXI-2 and 513 (50·2%) in GALAXI-3.” The studies enrolled adult patients with moderately to severely active Crohn’s disease.
Key findings:
Discussion points:
“Guselkumab treatment in participants with moderately to severely active Crohn’s disease was also evaluated in the GRAVITI study, which had a fully subcutaneous induction and maintenance treatment regimen. Clinical and endoscopic outcomes reported with subcutaneous guselkumab induction in the GRAVITI study were similar to those in the phase 3 GALAXI studies following intravenous guselkumab induction.”
“The incidence of adverse events with guselkumab during induction was low and similar to placebo.”
My take(borrowed from authors): In GALAXI-2 and GALAXI-3, both guselkumab dose regimens (each including intravenous induction and subcutaneous maintenance) were superior to placebo for short-term (week 12) and long-term (week 48) endpoints and both guselkumab dose regimens were also superior to ustekinumab
DR Shores et al. J Pediatr Gastroenterol Nutr. 2025;81:158–161. Navigating the blame game: Exploring necrotizing enterocolitis, preterm nutrition, and the ramifications of a formula shortage
Key points from this commentary:
“Recent lawsuits involving preterm infant formula manufacturers in the United States (Abbott and Mead Johnson) … [a] formula shortage crisis … might ensue if these formulas are pulled from the market”
“Breast milk has long been associated with protection against NEC, possibly due to bioactive molecules that maybe protective. However, infants fed exclusively breastmilk can still develop NEC, highlighting a multifactorial etiology. Mother’s own breast milk provides the best protection against NEC and is the ideal primary form of nutrition for preterm infants…pasteurized donor breast milk provides some protection against NEC and should be offered if mother’s own breast milk is not available”
“Although preterm formula does not protect against NEC, it is the healthcare standard, assuming all medical comorbidities are taken into consideration for individualized care…preterm infant formulas that are specifically formulated to provide the calories, protein and micro-nutrient needs of preterm infants”
“Placing all the blame for the development of NEC on preterm formula manufacturers is not supported by science and is thus unfounded”
“For infants without access to mother’s own or donor breast milk, specialized formulas remain critical to their nutrition and survival….Vilifying formula companies risks provoking further shortages of essential specialized formulas, which could directly harm the very babies we all aim to protect”
National Covid Memorial Wall in London is a visual representation of the UK’s catastrophic loss to Covid-19. There are more than 240,000 individually hand-painted red hearts, each representing a person who died in the UK with Covid-19 as a direct cause of death. Many of the hearts on the Wall have been personalized with individual message
This entire essay is worth reading but may be behind a paywall.
An excerpt:
For most of my colleagues and me, the C.D.C. and the N.I.H. were the medical Mount Olympus, the towering pillars of medical authority. Contrary to right-wing portrayals, these were not dictatorial authorities. These were earned authorities, comprising our best, brightest and most dedicated peers. The formidable talents of these doctors and scientists would have commanded enviable salaries had they taken jobs in industry, but they chose the public sector instead — something that we clinicians were forever grateful for…
While there are some doctors who viewed our public health institutions with disdain — some of them now are running these very organizations — most practicing physicians relied heavily on them to deliver the best care possible to their patients, despite occasional quibbles. What a relief, I always felt, that there were people organizing the things I can’t do — testing new treatments, conducting population studies, keeping tabs on worldwide diseases, issuing guidelines and more.
But now that support is a shell of what it once was. I can no longer automatically rely on these institutions because their scientific North Star, even if imperfect at times, has been replaced by one that seems nakedly political. Remaining staffs are no doubt working valiantly to do their jobs, but they are hobbled by loss of colleagues, resources and reliable leadership. So when I hear that the C.D.C. has changed a vaccine recommendation, I now question whether that’s a recommendation I can trust. When the F.D.A. commissioner says he wants to change how the agency approves or rejects new treatments, I no longer feel sure that science is driving those decisions. It’s hard to convey how profoundly grieved my colleagues and I feel…
Robert F. Kennedy Jr.’s view seems to be that we doctors are shills for corporate interests and government bureaucrats, and that torching our vaunted institutions is the prescription to fix us. Mr. Kennedy’s ire seems oddly directed. I, too, am disgusted by the role of money in health care, but I see it more as a result of the system we’ve set up, rather than the people who labor within it…
Notably missing from Mr. Kennedy’s Make America Healthy Again agenda is any suggestion that we provide universal health care, as most other developed countries do. There is no push to expand Medicare and Medicaid, which help some of our sickest patients. There is no focus on expanding access to early childhood education and supplemental nutrition programs, which offer steep health benefits…[There] is a barely concealed antipathy toward the people who are the engine of these institutions — doctors, scientists, policy wonks…
Every time you go to your doctor or get treated by a nurse, there’s a chorus of researchers, public health workers, policy experts, epidemiologists and advisory panels arrayed behind them, aided by laboratories, databases, websites, early-detection systems and clinical guidelines. Our current government seems determined to wrench this away, handicapping your health care team’s ability to care for you.
My take (borrowed in part from author): Our health care system needs to improve costs, accessibility, and outcomes. Yet, the changes to our healthcare and research under this administration are making matters worse. “So many of our resources are now gone, and those that remain no longer feel trustworthy. Americans’ health will decline at the hands of our federal government. And there’s no vaccine for that.”
Prescription drug denials by private insurers in the United States jumped 25 percent from 2016 to 2023, according to a new analysis of more than four billion claims… compiled for The New York Times by the medical data company Komodo Health, shows that denial rates rose from 18.3 percent to 22.9 percent….
Experts who have studied denials said the skyrocketing costs of popular new weight loss medications and greater automation of the claims process with artificial intelligence may have contributed to the rising rejection rates…
Prior authorization was responsible for about 10 percent of denied claims in the Komodo data. The analysis found that the most common reason for a drug claim to be rejected was that a refill had been requested “too soon,” before the patient was eligible for more medication…
Pricey new GLP-1 weight loss drugs like Ozempic, and other blockbuster medications, may have led insurers to increase restrictions on other drugs as they grappled with ways to offset those growing costs.
My take: Insurance companies and their pharmacy benefit managers are increasing their denials of medications. Presumably, much of this increase is driven by the pursuit of higher profits rather than the pursuit of better patient outcomes.
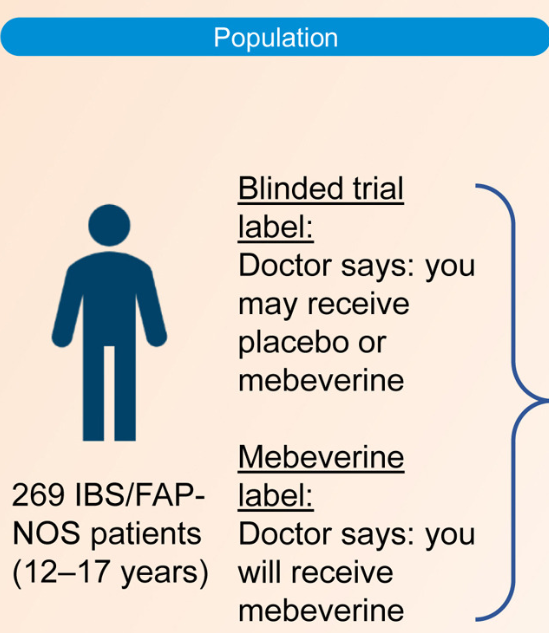
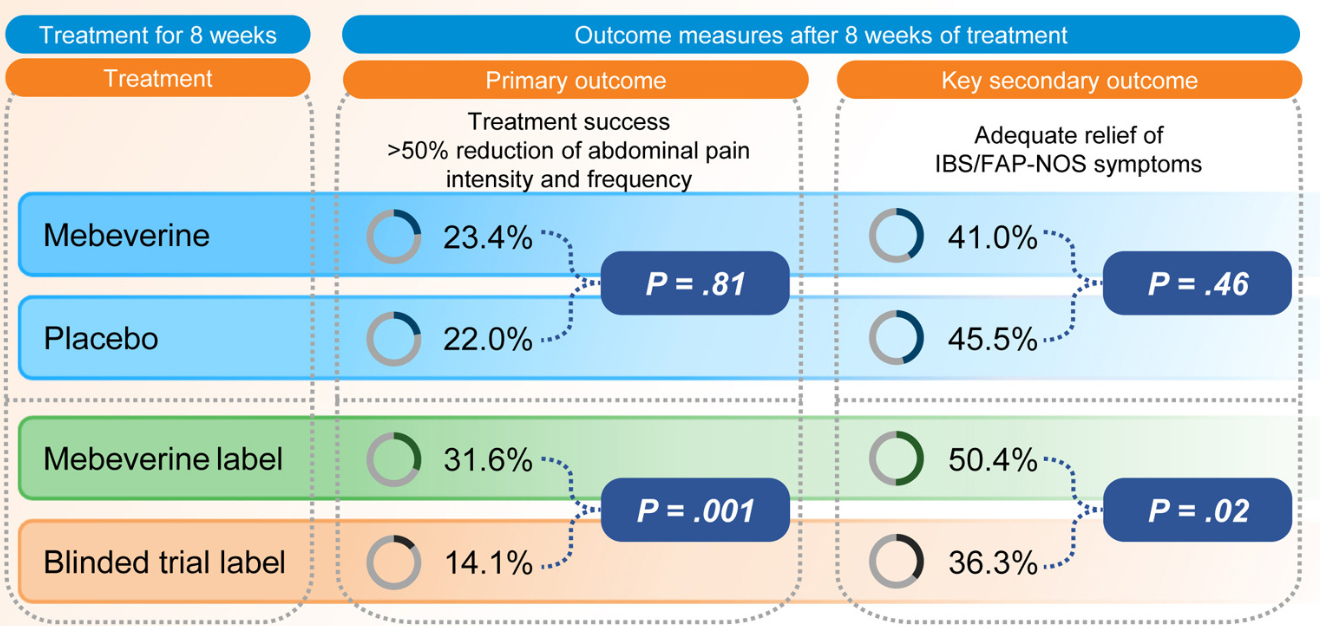
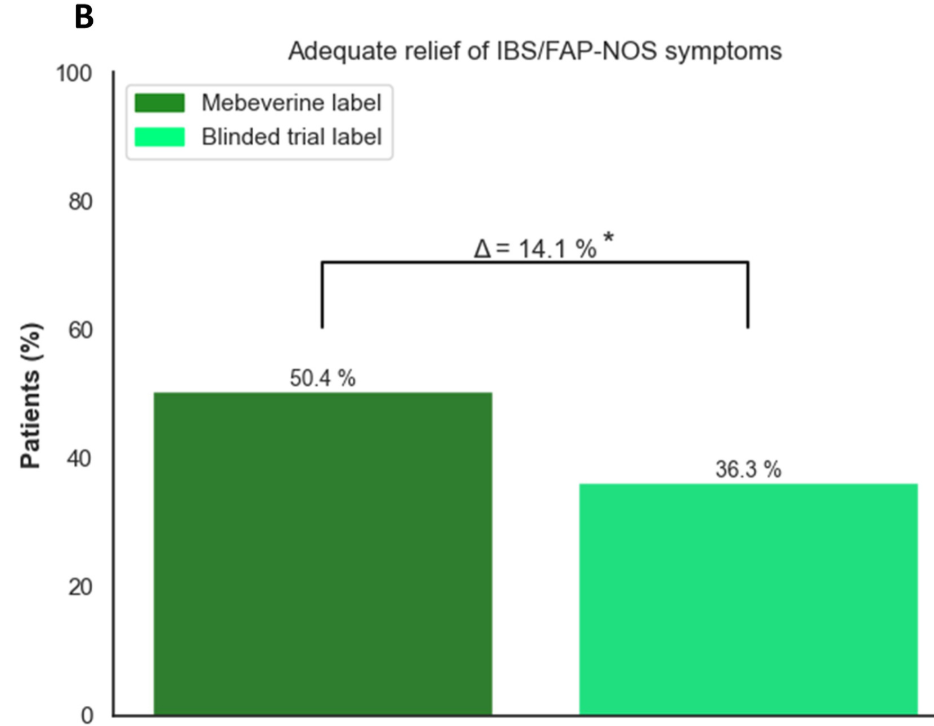
Methods: This was a randomized trial with 12-17 yr olds with irritable bowel syndrome or functional abdominal pain who received mebeverine (200 mg twice daily) or placebo for 8 weeks. Treatment was labeled as “mebeverine or placebo” (blinded trial label) or “mebeverine” (mebeverine label), creating the following 4 groups: (1) mebeverine-blinded trial label, (2) mebeverine-mebeverine label, (3) placebo-blinded trial label, and (4) placebo-mebeverine label. Randomization (1:1:1:1) was masked to physicians, except for drug labeling. Primary end point was treatment success (>50% reduction of abdominal pain intensity and frequency) after 8 weeks. The key secondary end point was adequate relief of symptoms.
Key findings:
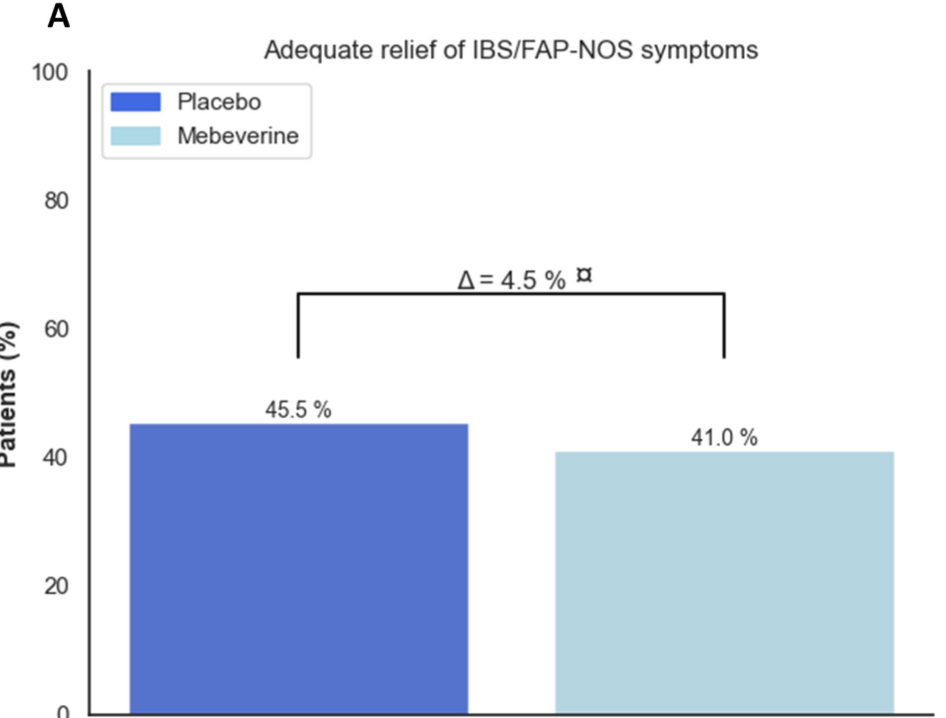
Blinded Trial Label: Treatment success was similar between those receiving mebeverine (groups 1 and 2) (n = 31 [23.4%]) and placebo (groups 3 and 4) (n = 30 [22.0%]; odds ratio [OR], 1.08
Effect of Being Informed of Treatment with Active Medication: Treatment success was higher in groups with the mebeverine label (groups 2 and 4) (n = 42 [31.6%]) compared with the blinded trial label (groups 1 and 3) (n = 19 [14.1%]; OR, 2.84
Discussion Points:
“This is the first study evaluating the impact of positive labeling on pain in a pediatric population. Our findings of a doubled treatment effect rate (32.9% vs 15.1%) when children were told they were receiving the active drug, are in line with adult studies showing higher pain reduction with positive labeling..14,19 It underscores the importance of positive expectations in pain management, which operates via multiple mechanisms.”
“Results of previous research has shown that children with IBS can also report symptom relief when they know that they are receiving an inert compound, known as an ‘“’open-label placebo.’22“
“Ethical norms state that ‘“’the use of a placebo without the patient’s knowledge may undermine trust, compromise patient–physician relationship, and result in medical harm to the patient.’26“
My take: This is a fascinating study showing how expectations for treatment can enhance the placebo effect. While the authors and the associated editorial mull over the ethical issues regarding deception of giving placebo without the family’s knowledge, in clinical practice many of the current drugs (eg. antispasmotics, neuromodulators, probiotics) have uncertain benefit and can be given without concern for deception.
Related blog posts:
Good Study, Bad Practice: Placebo for IBS and Functional Abdominal Pain “It is a mistake to consider placebo as a treatment for functional abdominal pain. In many children, pain fluctuates and may improve with reassurance, distraction, healthier diets, and physical activity. However, we also need more effective therapies including pain psychology, dietary approaches and medications. The idea that placebo helps is misleading and undermines the fact that patients with functional disorders need effective treatment.”