A recent study (BG Feagan, WJ Sandborn et al NEJM 2016; 375: 1946-60) provides extensive data regarding the effectiveness of ustekinumab for Crohn’s disease.
This publication combines three trials (industry-sponsored): UNITI-1, UNITI-2, and IM UNITI. The first two trials with 741 and 628 patients respectively examined intravenous ustekinumab for induction. Patients (18 years or older with Crohn’s disease) received either 130 mg, 6 mg/kg or placebo. UNITI-1 were patients with primary or secondary nonresponse to TNF antagonists. UNITI-2 were patients in whom conventional therapy failed or in which unacceptable side effects developed. The majority of UNITI-2 patients had not received a TNF antagonist.
IM UNITI with 397 patients followed patients who completed the first two trials for maintenance (90 mg SC every 8 weeks or every 12 weeks). For this study, the primary end point was remission at week 44 (CDAI score <150).
The IM UNITI study involved 260 sites in 27 countries.
Key findings:
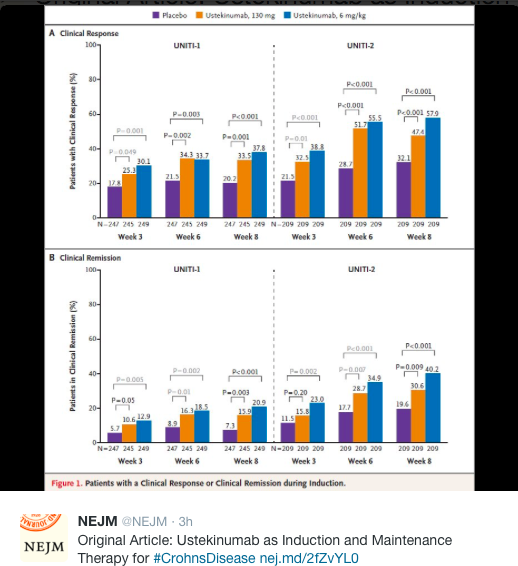
- With the induction trials, ustekinumab outperformed placebo at 6 weeks. For UNITI-1, 130 mg dosing resulted in 34.3% response, 6 mg/kg resulted in 33.7% response and placebo 21.5%.
- For UNITI-2, 130 mg dosing resulted in 51.7% response, 6 mg/kg resulted in 55.5% response and placebo 28.7%.
- For IM UNITI, every 8 weeks dosing resulted in 53.1% remission at week 44, compared with 48.8% dosed every 12 weeks, and 35.9% who received placebo.
- For IM UNITI, among those who started in remission at week 0, 66.7% (q 8 weeks), 56.4% (q12 weeks) and 45.6% (placebo) remained in remission at 44 weeks.
When looking at more objective results, both UNITI-1 and UNITI-2 showed significant drops in calprotectin and CRP values; both of these objective markers favored 6 mg/kg over 130 mg fixed induction dose.
- UNITI-1 at 6 weeks, calprotectin dropped 38.6 in 130 mg dosing group, 41.3 in 6 mg/kg group and 0 in placebo.
- UNITI-2 at 6 weeks, calprotectin dropped 55.0 in 130 mg dosing group, 106.3 in 6 mg/kg group and 0 in placebo.
- For the IM UNITI objective markers, it was noted that the median CRP values generally were unchanged in both treatment groups (q8 weeks, and q12 weeks) but increased in the placebo group by ~4 mg/L. Also, calprotectin remained <250 mg in both ustekinumab treatment groups at a much higher percentage than those who received placebo.
Safety:
Extensive safety data are reported and more than 60% of all patients, including placebo-treated patients reported potential adverse effects. Adverse effects and serious adverse effects were similar in treatment and control groups. During 1 year of therapy, there were no deaths or instances of the reversible posterior leukoencephalopathy syndrome.
Other points:
- Response to ustekinumab was observed as early as week 3
- UNITI-2 patients, most of whom had not failed a TNF antagonist, had higher response than UNITI-1 likely due to disease which was less refractory and of shorter duration
My take: These data support the use of ustekinumab for Crohn’s disease, particularly in patients who have not responded to other therapies.