NY Times 3/11/24: The Fourth Anniversary of the Covid Pandemic
“Globally, Covid ranks among the worst killers since 1900. AIDS, for example, is estimated to have killed about 40 million people, but over a half century rather than only four years. The 1918 flu killed somewhere between 20 million and 50 million people.”
“Among high-income countries, the U.S. has had one of the highest Covid tolls. The excess-death rate here, as a study by Jennifer Nuzzo and Jorge Ledesma of Brown University notes, has been much higher than in Canada, Britain, Germany, France, Spain, Sweden, Denmark, Japan, South Korea or Australia…”
“Many Americans, especially political conservatives, were skeptical of the vaccines despite overwhelming evidence of their effectiveness. To this day, more than 30 percent of self-identified Republicans have not received a Covid vaccine shot, compared with less than 10 percent of Democrats…You can see the tragic effects of vaccine skepticism in this chart.“
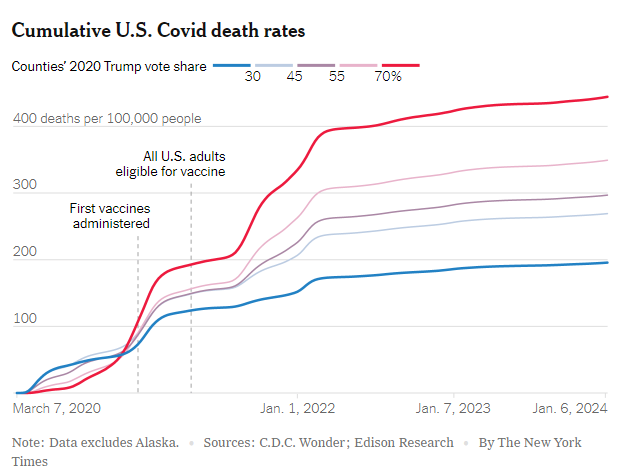
“While many liberals exaggerated the value of pandemic restrictions, they were right about the vaccines. “
According to data from Washington State in 2023, the death rate for those older than 65 years due COVID-19 was nearly double in those unvaccinated compared to those who had been boosted. In the younger age group, 35-64, the rate of fatal infection was much lower but remained 5 times as high in those unvaccinated compared to those who had been boosted.
My take: COVID-19 has exacted a tremendous toll and these articles do not even focus on long COVID which afflicts so many people as well.
Related blog posts:
- Life Expectancy Dropping in U.S. (March 2023)
- Partisan Divide, Misinformation and Risk of COVID-19 Death (May 2022)
- Excess Deaths From COVID-19 and Other Causes (Dec 2020)
- No Exaggeration: Too Many Children Are Dying in the U.S.
- Firearms: #1 Cause of Pediatric Deaths & Households with Guns =More Deaths