This past week Chelly‘s terrific work for Camp Oasis and CCFA was highlighted by the AJC: Doc devotes time to patients at summer camp and beyond. Chelly also leads our ImproveCareNow Team.


This past week Chelly‘s terrific work for Camp Oasis and CCFA was highlighted by the AJC: Doc devotes time to patients at summer camp and beyond. Chelly also leads our ImproveCareNow Team.
JE Axelrad et al. Inflamm Bowel Dis 2023; 29: 888-897. Early Initiation of Antitumor Necrosis Factor Therapy Reduces Postoperative Recurrence of Crohn’s Disease Following Ileocecal Resection
This retrospective cohort study identified 1037 patients with Crohn’s disease who underwent ileocecal resection (ICR). Only 5.4% were younger than 18 yrs at the time of surgery. In this cohort, 278 (26%) received a biologic agent as prophylaxis to prevent recurrence with 80% receiving an anti-TNF agent. In those receiving an anti-TNF agent, 35% were started on therapy within 4 weeks of surgery and 65% were started between 4 and 12 weeks. Recurrence was defined by endoscopy (≥ i2b Rutgeerts score) or radiography (active inflammation in neoterminal ileum). Key findings:
In their discussion, the authors note that their findings reinforce previous studies which showed beneficial effects of anti-TNF therapy for POR, including the PREVENT trial. This randomized controlled trial with infliximab initiation within 45 days postoperatively in high risk individuals reduced endoscopic recurrence at 18 months (22.4% compared with 51% in placebo group).
My take: Anti-TNF therapy, even in those with prior exposure, likely improves outcomes in patients with Crohn’s disease following ileocecal resection. This study indicates that starting therapy within the first 4 weeks is more beneficial.
Related blog posts:

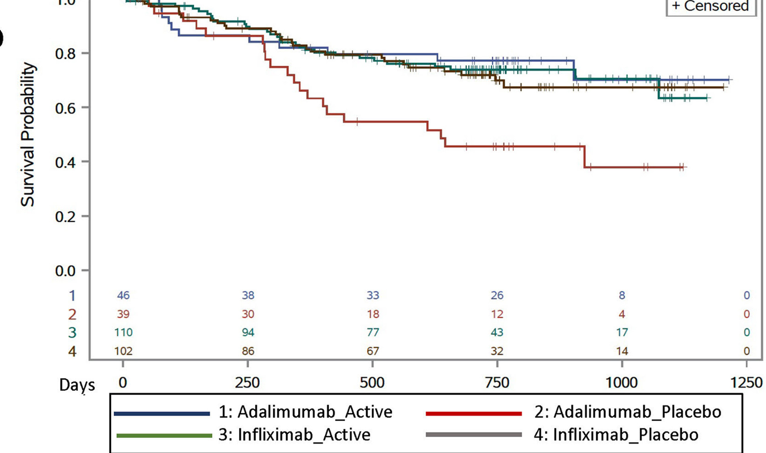
MD Kappelman et al. Gastroenterology. 2023: 165: 149-161. Open Access! Comparative Effectiveness of Anti-TNF in Combination With Low-Dose Methotrexate vs Anti-TNF Monotherapy in Pediatric Crohn’s Disease: A Pragmatic Randomized Trial
This study enrolled 297 children with Crohn’s disease starting anti-TNF therapy. Patients initiating infliximab or adalimumab were randomized in 1:1 allocation to methotrexate or placebo and followed for 12–36 months.
Methotrexate dosing: For those in the active arm, oral methotrexate was administered with a weekly dose of 15 mg for children ≥40 kg, 12.5 mg for children 30 to <40 kg, and 10 mg for children 20 to <30 kg. All participants received pretreatment with ondansetron 4 mg (or placebo) to prevent nausea and folic acid (1 mg/d).
Key findings:
My thoughts on this study:
My take: Given the increased difficulty monitoring the kids on adalimumab, they are probably better off on dual therapy. My suspicion, though, is that if they had optimized levels, the benefit of dual therapy is probably small and would mirror the findings with IFX.
O Ledder et al. JPGN 2023; 76: 799-806. Approach to Endoscopic Balloon Dilatation in Pediatric Stricturing Crohn Disease: A Position Paper of the Endoscopy Special Interest Group of ESPGHAN
This position paper regarding dilatation of strictures in Crohn’s disease provides mostly vague advice.
Here are a few examples:
The main clear cut recommendations are to obtain careful consent, expecting a complication rate of ~4% (eg. bleeding, sepsis, perforation), and to have surgical backup.
My take: This “position paper” offers very few positions on management advice and gives little clear guidance in terms of dilating strictures in Crohn’s disease.
Related blog posts:





SS C Rao et al. Gastroenterol 2023; 164: 1202-1210. Randomized Placebo-Controlled Phase 3 Trial of Vibrating Capsule for Chronic Constipation
Methods: This was a a phase 3, double-blind, placebo-controlled trial of patients with chronic constipation, who were randomized to receive either a vibrating or placebo capsule, once daily, 5 days a week for 8 weeks. The primary efficacy end points were an increase of 1 or more complete spontaneous bowel movements per week (CSBM1 responder) or 2 or more CSBMs per week (CSBM2) from baseline during at least 6 of the 8 weeks
Key findings:
The capsule used is 24 mm x 11 mm and includes a motor for vibrations, a battery, a computer chip and a latex-free plastic shell. The control group had received a dissolvable sham capsule.
I looked up cost of this new treatment and it is approximately $89/month which equates to $139 price per poop (PPP). To my knowledge, the PPP is a new metric –I have not seen it previously. For the vibrating capsule, I derived this figure by dividing the monthly cost into a weekly cost and dividing it by 0.16 (mean difference in weekly stooling with vibrating capsule). The PPP may be competitive with some of the constipation medications which cost in the range of ~$500 per month on GoodRx (like prucalopride and linaclotide) but is much more costly than senna products which can be purchased for ~$5/month.
My take: The vibrating capsule is an expensive way to help with constipation

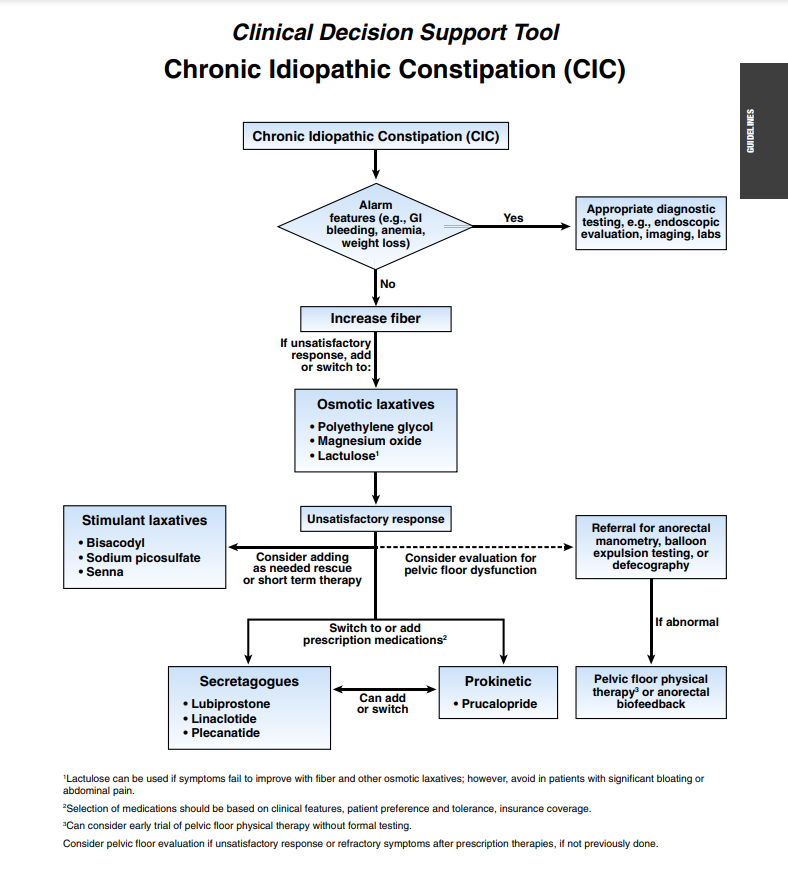
Related article: L Chang, WD Chey, AJ Lembo et al. Gastroenterol 2023; 164: 1086-1106. Open Access! American Gastroenterological Association-American College of Gastroenterology Clinical Practice Guideline: Pharmacological Management of Chronic Idiopathic Constipation
Gastroenterol 2023; 164: 1107. Open Access! Clinical Decision Support Tool
These guidelines for adults with constipation are similar to guidelines published in 2020 with the addition of prucalopride.
M Nistel et al. JGPN 2023; 76: 786-792. Impact of Dose Reduction of Topical Steroids to Manage Adrenal Insufficiency in Pediatric Eosinophilic Esophagitis
In this retrospective study with 32 children with both eosiniphilic esophagitis and adrenal insufficiency (and 81 control subjects), key findings:
One of the more useful parts of this publication is the authors provided their standardized approach in identifying AI: “our standard practice is to obtain a morning cortisol level 4-6 months after initiation of STS [swallowed topical steroids]. Subjects with morning cortisol <5 mcg/dL on 2 occasions (due to concerns with assay variation, patient compliance with fasting and holding steroids prior to testing) are then referred to endocrinology for further evaluation.”
My take: This article lays out a good approach for identifying AI in kids with EoE and then provides data on how effective reducing steroids are in resolving AI. It is noted that the peak eosinophil count tended to increase when STS doses were decreased.
Related posts:
Unrelated article from NPR (not from The Onion): Harvard professor who studies dishonesty is accused of falsifying data (June 26, 2023)



One of my partners, Jordan Weitzner, retrieved this foreign body with an upper endoscopy from an 8 yo patient recently.

Related blog posts:
HS Ahmed et al. Hepatology 2023; 77: 2063-2072. The association between hepatic steatosis and incident cardiovascular disease, cancer, and all-cause mortality in a US multicohort study
The authors included 10,040 participants from the Framingham Heart Study, the Coronary Artery Risk Development in Young Adults Study, and the Multi-ethnic Study of Atherosclerosis to assess the longitudinal association between liver fat (defined on CT) and incident cardiovascular disease (CVD).
Key finding:
Hepatic steatosis was associated with all-cause mortality after 12.7 years of mean follow-up when adjusting for baseline CVD risk factors, including body mass index (HR: 1.21, 1.04–1.40); however, the association between hepatic steatosis and incident CVD was not statistically significant after we accounted for body mass index in models considering baseline covariates or time-varying covariates. We observed no association between hepatic steatosis and CVD-related mortality or incident cancer.
My take: While CVD is the leading cause of mortality in patients with fatty liver disease, this study suggests that hepatic steatosis is a marker for this increased risk rather than an independent cause.
DU Lee et al. Liver Transplantation 2023; 29: 626-643. The trends in cost associated with liver transplantation in the US: Analysis of weighted hospital data
This lengthy article is loaded with data on trends and costs of liver transplantation in the U.S.
Key findings:
Editorial: A Kaplan et al. Liver Transplantation 2023; 29: 568-569. Open Access!
Liver transplant at all costs Key points:
My take: It is likely that the costs of liver transplantation are going to continue to rise unless we develop a shortage of suitable liver donors or a shortage of transplant personnel. Severe fatty liver disease and alcoholic liver disease continue to increase in frequency while hospital costs continue to soar. Reducing costs will rely on reversing the tide of these diseases.
Related blog posts:

SR Gupta et al. JPGN 2023; 76: 776-781. Outcomes for Standardized Home and Hospital-Based Infusions of Infliximab for Children With Inflammatory Bowel Disease
In this retrospective study with 102 children, key findings:
The authors note that HI were arranged with a single home health company with pediatric PALS-trained nurses. In addition, there was “direct communication between the home health nurse and IBD nurse after each infusion.”
Prior studies of HI have shown increased AOs in patients receiving HI including stopping therapy, ER visits, and hospitalizations (Clin Gastroenterol Hepatol 2020; 18: 257-258, Am J Gastroenterol 2020; 115: 1698-1706, JAMA New Open 2021; 4: e2110268).
My take: If set up properly, home infusions could be a reasonable alternative to hospital-based or office-based infusions.

In this article, from May 31, 2023: Sick Workers Tied to 40% of Food Poisoning Outbreaks, C.D.C. Says
“Each year, 48 million people become sick from a food-borne illness, according to C.D.C. estimates. Of those, 128,000 are hospitalized and 3,000 die.”
