Danish residents with elevated lipids and CVD risk factors who were taking statins for CVD prevention saw a 16% lower risk per unit time of incident IBD, the researchers found (AS Faye et al. J Intern Med 2025;298[6]:686-696. Statin use for primary prevention of cardiovascular disease reduces the risk of incident IBD: A population-based cohort study)…
The study was a population-based, prospective cohort design drawing on the Danish National Registries. Participants were over 40 years of age and had undergone low-density lipoprotein (LDL) measurement between 2008 and 2022…Each of 110,961 people who picked up statin prescriptions within six months of LDL measurement was matched to five others (n=554,805) not prescribed statins by age, sex, calendar year, and CVD risk factors…
The aHR of developing IBD for statin users versus nonusers was 0.84 (95% CI 0.72-0.97)…The five-year number needed to treat (NNT) with statins was 2,881 to prevent one additional IBD case…
In addition to lipid-lowering properties, statins have anti-inflammatory and immunomodulating actions.
My take: This study suggests that statins have an “off target” beneficial effect in reducing the risk of inflammatory bowel disease. However, it is possible that statin use is not directly beneficial but an epiphenomenon. For example, individuals taking statins may have modified their diet to lower their risk as well.
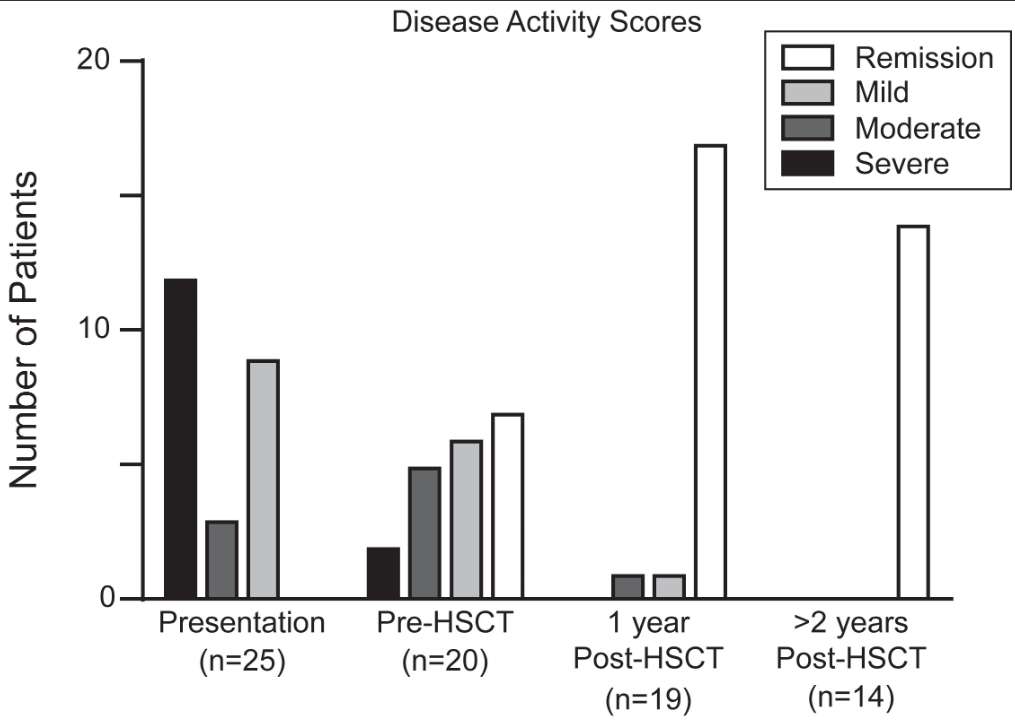
This was a retrospective single-center (CHOP) study of 25 children with monogenic IBD who underwent Hematopoietic Stem Cell Transplant (HSCT) (2012-2022).
Key findings:
Seventy-two percent of patients had Crohn’s Disease, and 28% were classified as IBD-unspecified. Ninety-two percent of patients had VEO-IBD, 56% presenting under age 1
At most recent follow-up, 92% of patients achieved sustained medication-free remission of IBD and 60% with prior ostomy underwent re-anastomosis. There was 100% survival at a median follow-up of 3 years
There was significant improvement in growth, hospital days, and severe infections
Disease activity scores at the time of IBD presentation, immediately prior to transplant, 1-year post-transplant, and at most recent follow up if ≥2 years since transplant.
Discussion points:
“Delay of HSCT with the goal of obtaining remission of IBD prior to transplant may prove to be determinantal, as outcomes of HSCT are in general improved for younger patients,20 and medical remission is often unattainable for more severe forms of monogenic IBD. Within our cohort, 32% of patients had moderate or severe disease at the time of transplant despite medical optimization. None of these patients developed intestinal GVHD, which was a rare event in our total cohort”
“HSCT is not without risk, and complications occurred in our cohort, at rates typical of other IEI cohorts”
“The selection of patients who would benefit from HSCT requires multidisciplinary discussion.”
With regard to patient selection, one item that was not included in the discussion was the one patient excluded from their analysis who had a TTC7A gene defect. In the results section, it was explained that the patient with “TTC7A was subsequently excluded as transplant was performed for the indication of SCID alone, rather than treatment of intestinal disease.” More discussion on this point is merited as many centers would NOT have a patient with TTC7A undergo HCST specifically because it cannot correct the underlying bowel disease.
Also, it was noted that one patient with CTLA4 deficiency had undergone HSCT prior to the discovery of the genetic defect. With the more widespread use of genetic testing available now, this discovery may have obviated the need for HSCT as treatment with abatacept is typically effective.
My take: Overall, the authors present impressive results for HSCT for monogenic IBD and strengthen the need for genetic testing in those with early onset disease and those refractory to treatment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: “The prevalence of obesity among patients with inflammatory bowel disease (IBD) is estimated at 15-40%, and continues to rise. Obesity has been associated with a more severe phenotype of IBD.”
Methods: Retrospective cohort with 244 patients. Semaglutide was the most commonly prescribed agent (54%).
Key findings:
GLP-1RA use led to weight loss from 102 kg to 97.6 kg at 12-24 weeks postinitiation
GLP-1RA was associated with a significant drop in CRP from 10.1 mg/dL to 3 mg/dL
In a subset of 32, fecal calprotectin values decreased from 825 mcg/kg to 235 mcg/kg (P= 0.13)
Limitations: Retrospective study with a short duration, lack of a control group for this study, and lack of endoscopic data.
My take: As with the broader population, GLP-1 RAs help with weight loss in patients with IBD. Many patients may derive health benefits from weight loss alone. This study, though with numerous limitations, indicates the potential beneficial effects on the activity of IBD based on improvements in biomarkers.
From editorial (which is more expansive than the study):
Kappelman et al4 report the US prevalence of pediatric-onset IBD (diagnosed before the age of 20 years by a physician) as well as rates of disease based on race and ethnic background. To ensure that a representative population was captured, they combined multiple health administrative databases…
The authors report that the US currently has a pediatric IBD prevalence of 125 per 100,000 population, increased from 110 per 100,000 in 2011. This is higher than previously reported in Canada (82 per 100,000 in 2023)6 and Sweden (75 per 100,000 in 2010).7These differences may be due to the older age cutoff used in the US data, <20 years vs <18 years in the Canadian and Swedish studies. However, misclassification bias may also play a role...
Nevertheless, understanding the approximate prevalence of pediatric IBD in the US allows for adequate human and financial resource planning for this important population of children with an impactful chronic disease. The high prevalence should raise concerns among health care practitioners and policy makers that we have under-resourced IBD care in children, especially considering the high rate of use of biologics and the growing direct health costs incurred in the treatment of this population.11
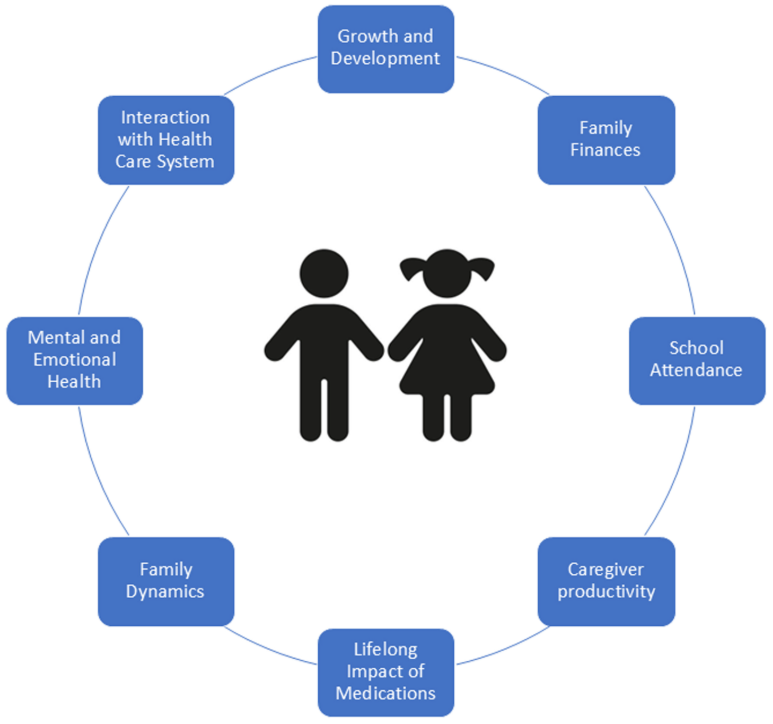
The burden of IBD in pediatrics goes beyond that of the child. Compared with adult IBD, it disproportionately affects caregivers and families (owing to missed work for appointments, hospitalizations, and home care), mental health of both the patient and the parents, and the health system...
They report that pediatric IBD is more frequent among White children and adolescents (145 per 100,000) compared with Black (91 per 100,000) and Hispanic (88 per 100,000) children, whereas children of Asian origin have markedly lower rates (52 per 100,000).“
My take: The updated prevalence data helps understand the increasing frequency of pediatric IBD. The associated commentary reminds us of the broader burden the disease has for families and for our communities.
B Kaj‐Carbaidwala et al. J Pediatr Gastroenterol Nutr. 2025; 80:450–454. Determining the time to cholangiocarcinoma in pediatric‐onset PSC‐IBD
Background: “Cholangiocarcinoma is a devastating disease, with up to 80% mortality and limited treatment options…A large retrospective cohort study reported that cholangiocarcinoma occurred in 1000 per 100,000 (1%) of children with PSC, with all occurring in children over 15 years of age and at a median of 6 years after the PSC diagnosis…Primary sclerosing cholangitis (PSC) is associated with a 400× increased risk of cholangiocarcinoma.”
Methods: Review of n = 175 studies resulted in a cohort of n = 21 patients with pediatric‐onset PSC‐IBD‐cholangiocarcinoma
Key findings:
The earliest diagnosis of cholangiocarcinoma was made at 14 years of age.
14% of of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first 6 months of the second diagnosis
23% of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first year of the second diagnosis
38% of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first 2 years.
50% of patients with pediatric‐onset PSC/IBD developed cholangiocarcinoma within the first 7 years
50% of patients were between 14 and 25 years old when diagnosed with cholangiocarcinoma
Based on these data, the authors recommend screening for cholangiocarcinoma in this population of pediatric patients with IBD-PSC. Screening would include ultrasound or magnetic resonance cholangiopancreatography along with serum cancer antigen 19‐9 screening every 6–12 months. At the same time, the authors acknowledge limitations including a highly-selected patient population (selection bias) and relatively small number of patients. The absolute increase in risk for cholangiocarcinoma is not known. This study did not provide an estimate of the number of patients with IBD-PSC who develop cholangiocarcinoma; it only provides data on those with cholangiocarcinoma (thus no denominator to establish risk).
My take: Children, particularly adolescents, with IBD-PSC are at increased risk for both cholangiocarcinoma and colorectal cancer. The optimal surveillance strategy is still unclear. However, particularly in adolescents, I would favor yearly ultrasound and CA 19-9 for cholangiocarcinoma along with a low threshold for frequent colonoscopy (see ESPGHAN guidelines below).
In the news: AP 5/4/25: Cuts have eliminated more than a dozen US government health-tracking programs “U.S. Health Secretary Robert F. Kennedy Jr.’s motto is “ Make America Healthy Again,” but government cuts could make it harder to know if that’s happening…..Among those terminated at the Centers for Disease Control and Prevention were experts tracking abortions, pregnancies, job-related injuries, lead poisonings, sexual violence and youth smoking, the AP found.”
Anantara Resort, Mai Khao Phuket
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
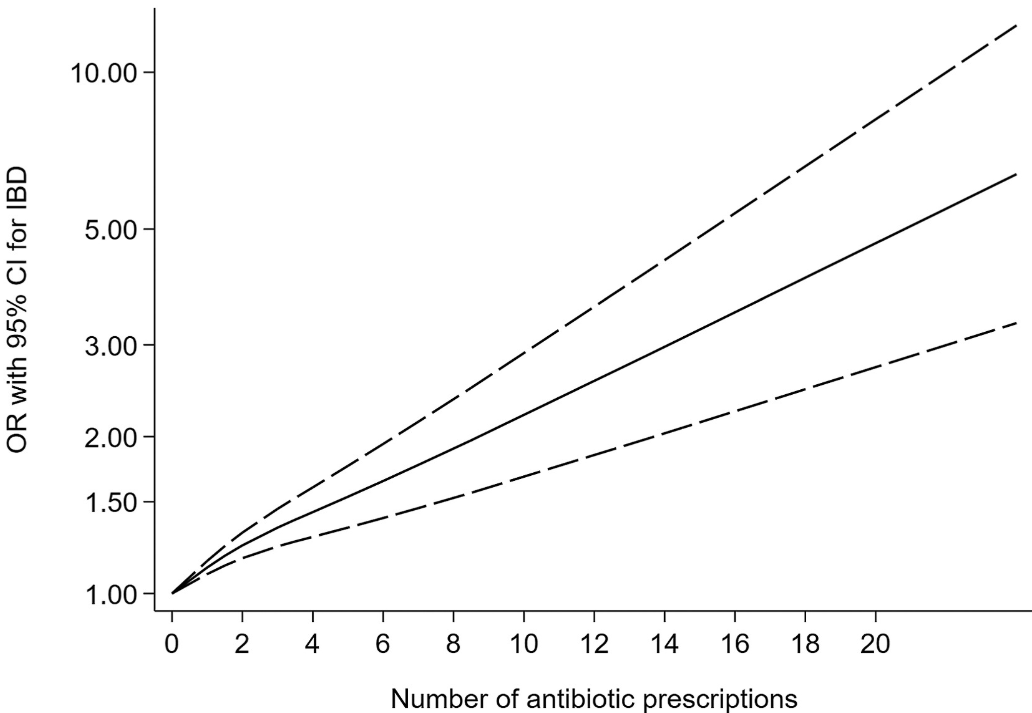
Twenty-eight studies involving 153,027 patients with IBD were included.
Key findings:
Antibiotic exposure was significantly associated with an increased risk of new-onset IBD for prescription-based studies (pooled OR, 1.41; 95% CI, 1.29–1.53) and for questionnaire-based studies (pooled OR, 1.35; 95% CI, 1.08–1.68). ‘
This association existed for both Crohn’s disease and ulcerative colitis, as well as in children and adults for prescription-based studies.
Some of the limitations:
There was statistical heterogeneity was high in the primary analysis, possibly because of inconsistencies in study design
Most studies included a clear lag time, yet an inadequate lag time still creates the possibility of reverse causality.
The authors could not disentangle the risk of antibiotics from the risk of infection in leading to the development of IBD.
Nonlinear dose-response relationship between antibiotic exposure and risk of new-onset IBD (solid black line and short dash black line represent estimated ORs and corresponding 95% CIs of nonlinear relationship)
My take: This is another study showing an association between antibiotic use and new-onset IBD. While this study does not prove causation, it is another reason for good antibiotic stewardship.
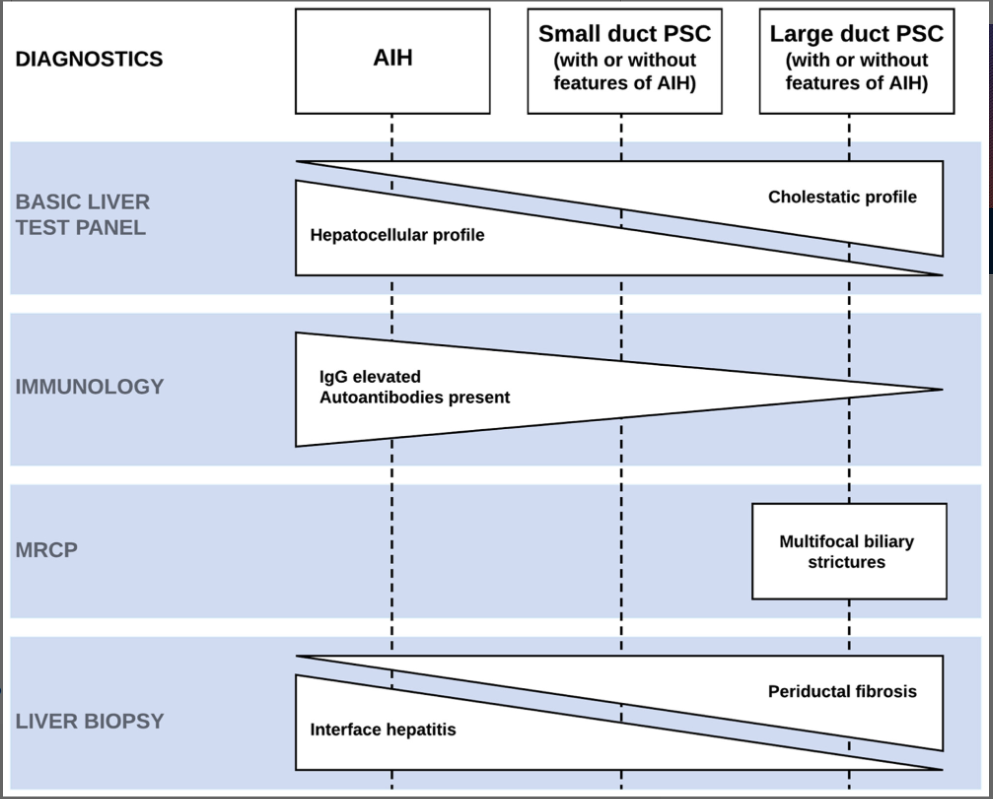
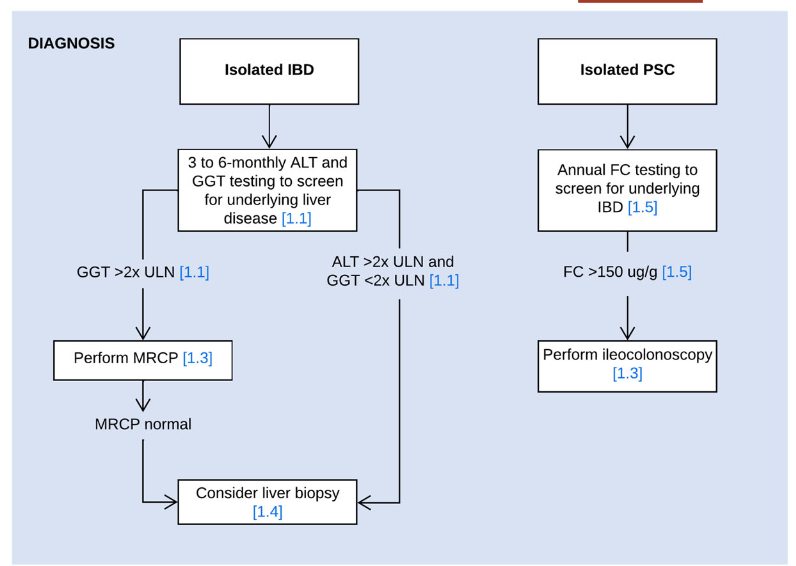
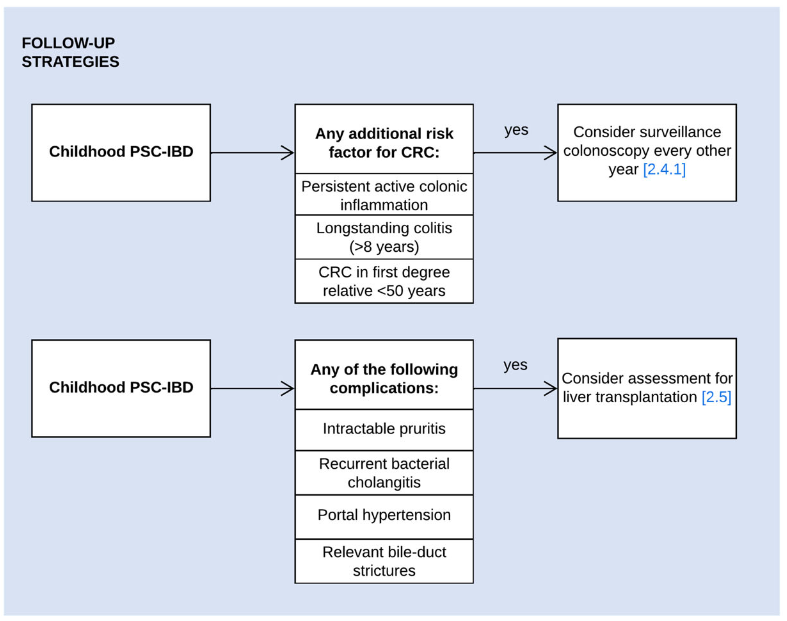
PF van Rheenen et al. JPGN 2024; DOI: 10.1002/jpn3.12378. Open Access! Primary sclerosing cholangitis in children with inflammatory bowel disease: An ESPGHAN position paper from the Hepatology Committee and the IBD Porto group
Recommendations:
In children with suspected or confirmed IBD, screening for liver disease is usually performed at 3 to 6 months intervals and a work‐up for underlying liver disease is most commonly initiated when liver enzymes exceed 2x the upper limit of normal
Use MRCP as the radiological modality of choice for diagnosing PSC
Consider performing a liver biopsy in children with IBD and suspected PSC in the following circumstances: i) Normal biliary tree at MRCP, ii) raised immunoglobulin G and the presence of liver-specific autoantibodies, or iii) clinical uncertainty before steroid induction therapy for IBD
Perform fecal calprotectin screening at least once yearly in children with isolated PSC and/or AIH to select patients for diagnostic endoscopy for suspected inflammatory bowel disease (panel recommends cutoff of >150 indicating need for ileocolonoscopy)
Surveillance colonoscopy should be considered in children with PSC–IBD and the following risk factors of colorectal cancer: i) persistent active colonic inflammation, ii) longstanding colitis (≥8 years), or iii) a family history of colorectal cancer in a first-degree relative <50 years. (The overall risk of colon cancer in those <18 yrs of age is very low)
UDCA may be prescribed at doses of 15–20 mg/kg/day. Despite evidence of improvement of liver enzymes, its long-term effect on disease progression has not been demonstrated. Consider a 6-months therapeutic trial of UDCA, either immediately after PSC diagnosis or when spontaneous normalization of GGT does not occur in the first 6 months postdiagnosis. Continue UDCA treatment if there is a meaningful reduction or normalization of GGT or improvement of symptoms
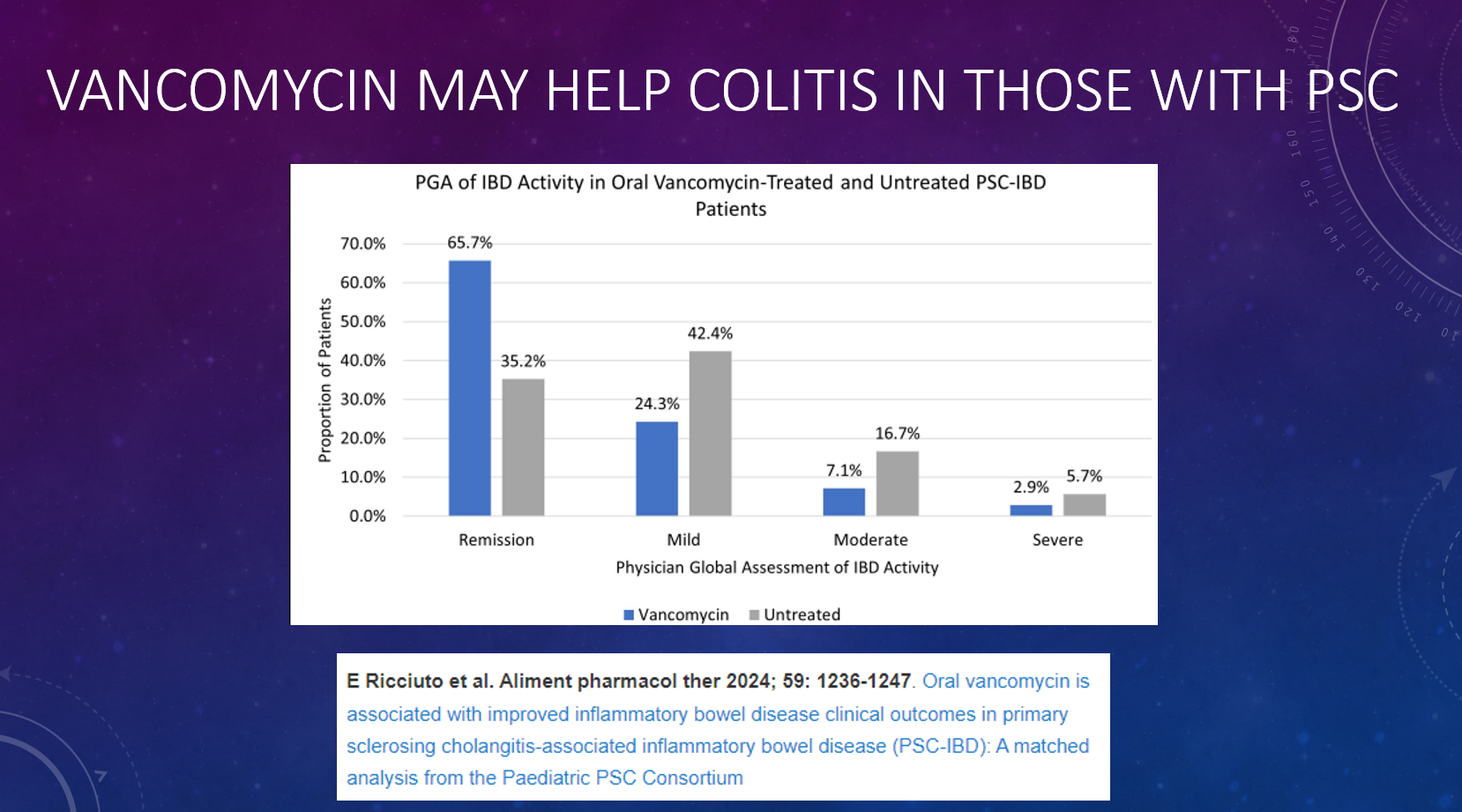
Oral vancomycin may be prescribed for a potential improvement in liver biochemistry as well as bowel inflammation. Its long-term effect on disease progression has not been demonstrated
In children with PSC–IBD and biochemical, serological, and histological features of AIH, the use of corticosteroids and antimetabolites may suppress immune-mediated hepatitis. In the absence of convincing AIH features, the use of corticosteroids and antimetabolites is not indicated to manage PSC
Children with PSC, relevant bile-duct strictures and cholestatic symptoms should be assessed for liver transplantation. When their symptoms are likely to improve following biliary intervention, ERCP can be considered
Recommended blood testing for children with PSC: At diagnosis: Autoantibodies (ANA, anti-SMA, anti-LKM-1, anti-LC1, and anti-SLA), Every 3-6 months: ALT, AST, GGT, Albumin, INR, Platelets, CRP. Every 12 months: IgG, AFP, and Fat Soluble vitamins. Consider f/u autoantibodies in those with elevated IgG at f/u lab testing
My take: This is a useful position paper; it does not have a zillion recommendations like some other ESPGHAN positions papers. Given the frequency of liver enzyme elevation in patients with IBD, mild to modest elevations may need to be observed before launching an extensive evaluation (see related blog posts below).
Aspen Webinar 2021 Part 5 -Autoimmune Liver Disease & PSC 2021. This lecture highlights studies show lack of efficacy with vancomycin, ursodeoxycholic acid and vedolizumab in altering the liver disease. Also, there is potential utility of MMP-7 for distinguishing between PSC and AIH
This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).