This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
The authors utilized prospectively collected data from 3 population-based birth cohorts (Danish National Birth Cohort, Norwegian Mother, Father, and Child Cohort, and All Babies in Southeast Sweden). This collectively included nearly 170,000 offspring.
Key findings:
During median follow-up of 16.3–22.3 years, between 1996 and 2021, 543 offspring were diagnosed with IBD
In each country, there was no association between exclusive breastfeeding duration and offspring IBD risk
Discussion:
“In contrast to majority of case-control studies, both cohort studies reported null association between breastfeeding, treated as a binary exposure (any versus no breastfeeding) or by duration, and offspring IBD risk. Similarly, 2 nested case-control studies, leveraging prospectively collected data on early life exposures as part of the population-based Jerusalem Perinatal Study and 2 United Kingdom birth cohorts (the 1946 National Survey of Health & Development and the 1958 National Child Development Study) reported null associations between breastfeeding and IBD risk.22,23 Data from these studies, which are more rigorous in methodology compared with case-control studies, are consistent with findings from our analyses.”
My take: While this study has some limitations inherent in observational data, this study with prospectively-collected data indicates that breastfeeding did not modulate the risk of developing IBD.
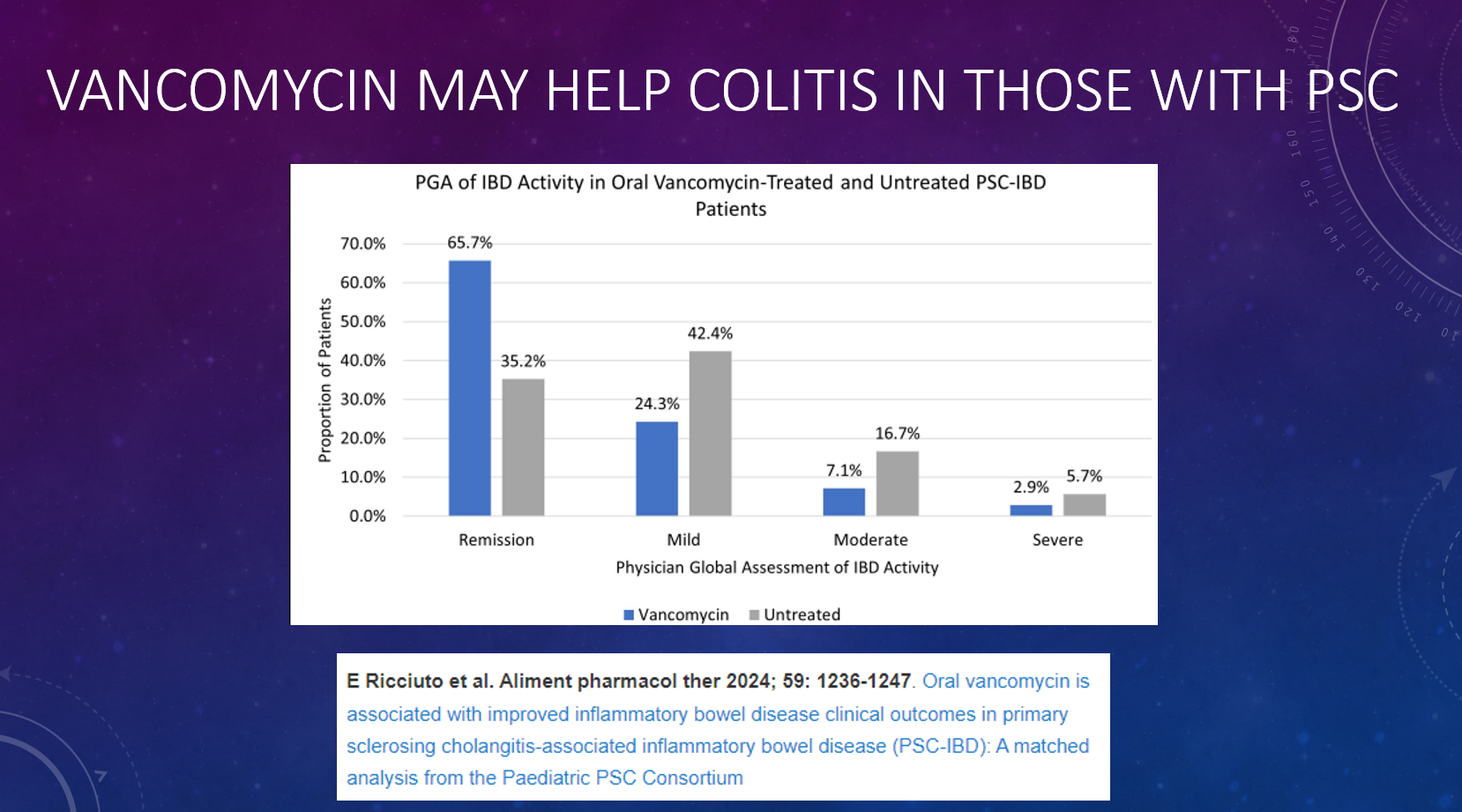
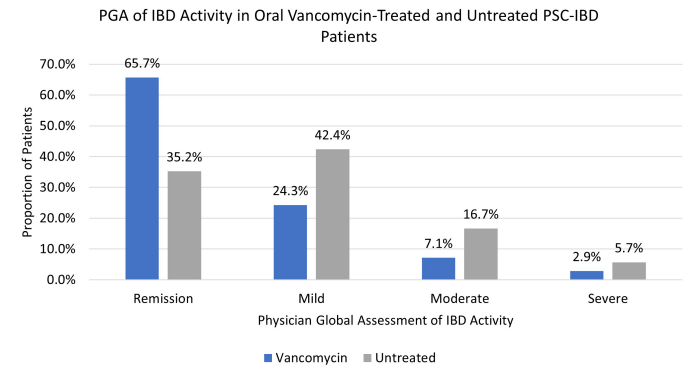
This was a retrospective study from 54 centers with 113 PSC-IBD pediatric patients receiving vancomycin (median age 12.7 years, 63% male). The matched cohort included 70 vancomycin-treated and 210 untreated patients. Clinical remission was defined as physician global assessment (PGA) of zero. It is noted that the Pediatric PSC consortium included 1362 patients at the time of this study; only 11% (n=113) were treated with vancomycin for at least 3 months. The median dose of vancomycin was 17 mg/kg/day and median duration was 2.5 years.
Key findings:
Vancomycin was associated with greater odds of IBD clinical remission (odds ratio [OR] 3.52, 95% CI 1.97-6.31; adjusted OR [aOR] 5.24, 95% CI 2.68-10.22).
Vancomycin was associated with increased odds of endoscopic remission (aOR 2.76, 95% CI 1.002-7.62; N = 101 with data), and with lower CRP (p = 0.03) and higher hemoglobin and albumin (both p < 0.01).
At baseline, prior to vancomycin, 34% (30/88) were in clinical remission; this increased to 60% (52/86) after 6 months of treatment. After ~ 1 year, 71% (55/78) of children treated with vancomycin were in remission, compared with 35% who had not receive the antibiotics.
Ursodeoxycholic acid use: 53% for vancomycin-treated and 82% of control group (P<0.001). Other cotherapies were similar including infliximab (36% vs. 27%) and vedolizumab (13% vs 7%)
Only 28 vancomycin-treated patients had baseline and f/u colonoscopy data available. 46% of this subgroup had endoscopic remission compared to 26% of matched untreated controls.
In the discussion, the authors acknowledge the limitations of a retrospective observational study. RCTs are quite difficult with rare disorders, especially in children. In addition, the exact mechanisms for vancomycin efficacy remain unclear -possibly microbial changes or its effects on bile acids. They note that many patients treated with vancomycin had mild clinical activity at baseline. Though, even this population may benefit with resolution of clinical inflammation which could reduce the risk of colorectal cancer.
My take: In patients with PSC-IBD, the use of vancomycin for IBD should be a consideration especially in those who have not responded adequately to other treatments.
Aspen Webinar 2021 Part 5 -Autoimmune Liver Disease & PSC 2021. This lecture highlights studies show lack of efficacy with vancomycin, ursodeoxycholic acid and vedolizumab in altering the liver disease. Also, there is potential utility of MMP-7 for distinguishing between PSC and AIH
The proverb “Necessity is the mother of invention” is often attributed to Plato. In the dialogue of The Republic, Plato wrote, “our need will be the real creator”. This quote came to mind as I was reading about the use of f for fatigue in inflammatory bowel disease (IBD).
Background: “Fatigue is highly prevalent in patients with IBD, affecting 72% of patients with active inflammatory bowel disease (IBD) and 47% in remission, and is associated with poor quality of life, absenteeism and presenteeism.1 However, understanding the mechanisms of IBD fatigue remains limited, as reflected in a lack of effective treatments.1“
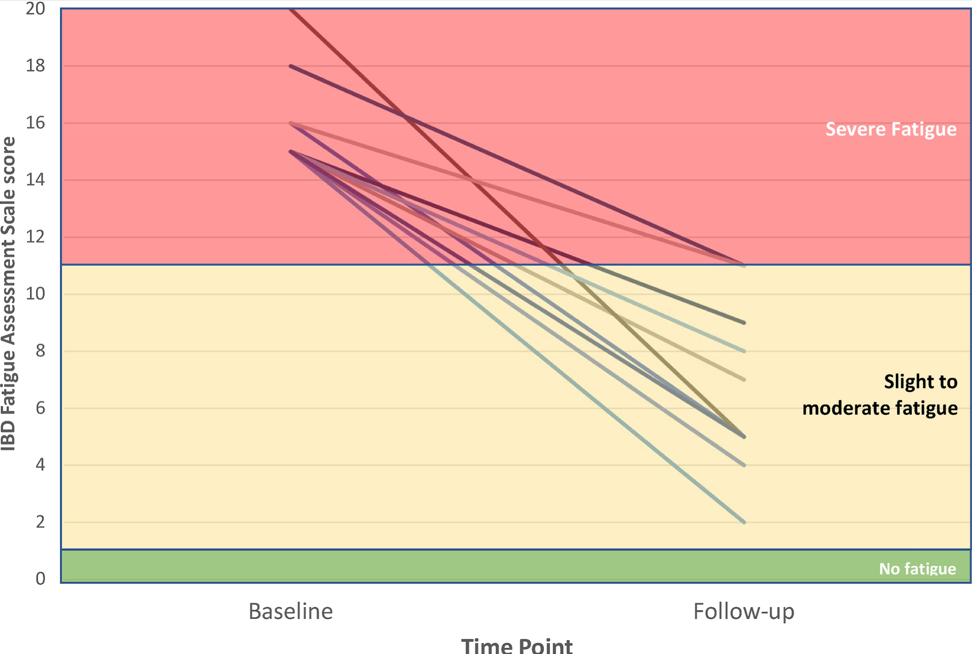
Methods: “Ten patients with IBD and severe fatigue were referred to a consultant psychiatrist. In all cases, mucosal inflammation and organic causes of fatigue (anemia, B12 deficiency, hypothyroidism) had been investigated and treated as much as possible. We measured fatigue severity using the IBD Fatigue Assessment Scale (IBD-FAS), designed specifically for IBD.5 Scores of 11 or higher out of 20 indicate severe fatigue and we only included patients scoring in this range.5
Dosing (for adults) of modafnil is described in the article.
Key findings:
“At baseline, the mean IBD-FAS score was 16.0 (SD, 1.7) of 20. After modafinil treatment [at 6 months], the mean IBD-FAS score was 6.7 (SD, 3.0), representing a mean improvement of 58.1% from baseline.”
“Although all 10 patients were severely fatigued at baseline, only 2 patients were still in the severe fatigue range after treatment.”
“Tolerability was good: 1 patient reported transient headache and 1 patient reported transient dizziness; another patient reported mild palpitations; but none of the patients reported gastrointestinal side effects.”
My take: Perhaps, modafinil will be helpful –pharmacologic therapy for severe fatigue is an unmet need. More studies are needed as this is a small study without a control group.
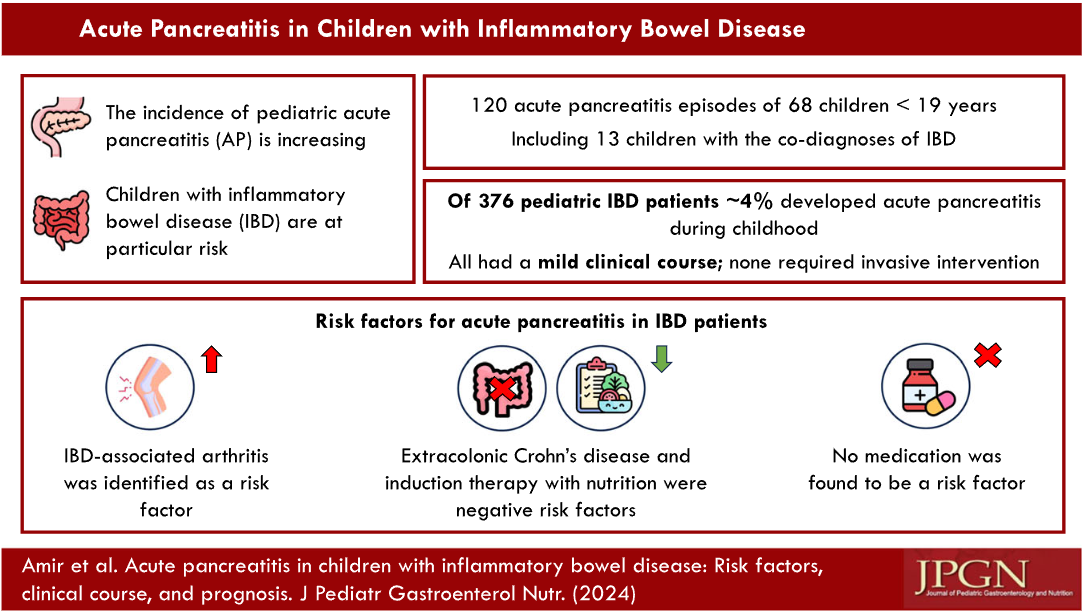
A Anafy et al. JPGN 2024; 79:325–334. Acute pancreatitis in children with inflammatory bowel disease: Risk factors, clinical course, and prognosis
In this retrospective study with 376 children, Key Findings:
4% of patients with pediatric IBD developed acute pancreatitis (AP)
The presumed etiology for AP in all IBD patients was IBD-related: IBD flare-up in five, side effects of medications in two, and undetermined in seven.
The only risk factor for AP development among IBD patients was IBD‐associated arthritis (23% vs. 3% for IBD‐non‐AP).
Extracolonic Crohn’s disease emerged as a negative risk factor for AP: it was present in only 2/13 (15%) IBD‐AP patients compared to 20/39 (51%) IBD‐non‐AP patients (p = 0.05). Patients who receive induction therapy with nutrition (exclusive enteral nutrition or Crohn’s disease exclusion diet) were less likely to be present in the IBD‐AP group (1/12 [8%] vs. 17/39 [44%] IBD non-AP patients, p = 0.04.
This study population, at the time of AP, had a relatively high number treated with ASA agents (66%; 11/14 AP-IBD and 26/42 Non-AP-IBD)), 27% with azathioprine (6/14 with AP-IBD and 9/42 Non-AP-IBD), and low number receiving biologics (18%, 2 AP-IBD and 8/42 Non-AP-IBD
My take: This study shows that acute pancreatitis is common in children with inflammatory bowel disease.
SJ Martinez-Dominguez et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1274–1283, https://doi.org/10.1093/ibd/izad175 Open Acess! Inflammatory Bowel Disease Is an Independent Risk Factor for Metabolic Dysfunction–Associated Steatotic Liver Disease in Lean Individuals
Methods: This was a cross-sectional, case-control study including 300 lean cases with IBD and 80 lean controls without IBD, matched by sex and age (median age ~45 yrs). All participants underwent a liver ultrasound, transient elastography, and laboratory tests. All patients with current or previous use of systemic steroid in the last 2 years were excluded from the analysis
Key Findings:
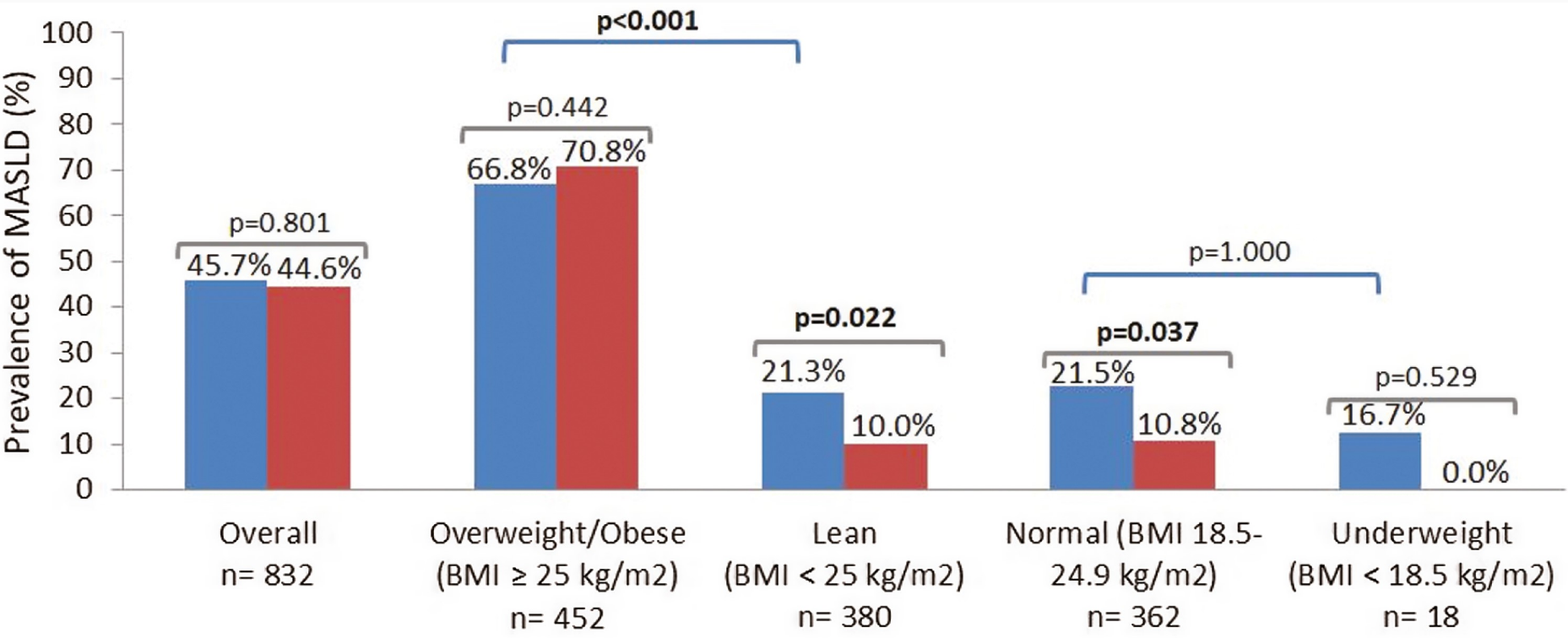
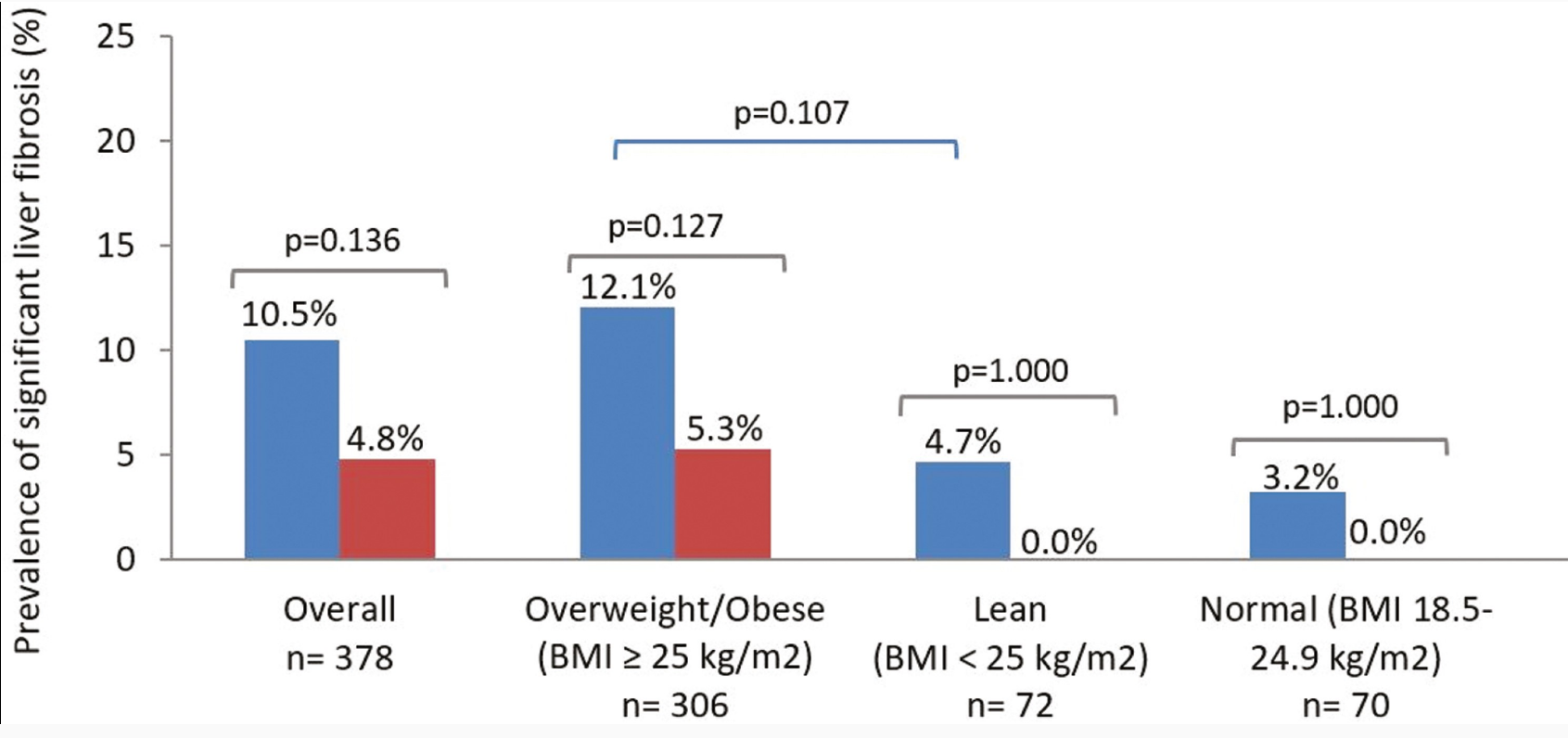
The lean IBD group showed a significantly higher prevalence of MASLD compared with lean non-IBD group (21.3% vs 10%; P = .022), but no differences were observed in the prevalence of significant liver fibrosis (4.7% vs 0.0%; P = 1.000)
No differences were found between the prevalence of MASLD in IBD and non-IBD participants who were overweight/obese (66.8% vs 70.8%; P = .442)
IBD was an independent risk factor for MASLD in lean participants (odds ratio [OR], 2.71) after adjusting for classic metabolic risk factors and prior history of systemic steroid use
Prevalence of metabolic dysfunction–associated steatotic liver disease (MASLD) in cases and controls according to body mass index (BMI) status. Blue bars: cases (inflammatory bowel disease). Red bars: controls (non–inflammatory bowel disease). P values in bold indicate statistical significance (P < .05).
My take: This study suggests that “chronic inflammation could play a role in MASLD development.” Also, this indicates that MASLD could be a reason for elevated LFTs in patients with IBD, even in lean patients.
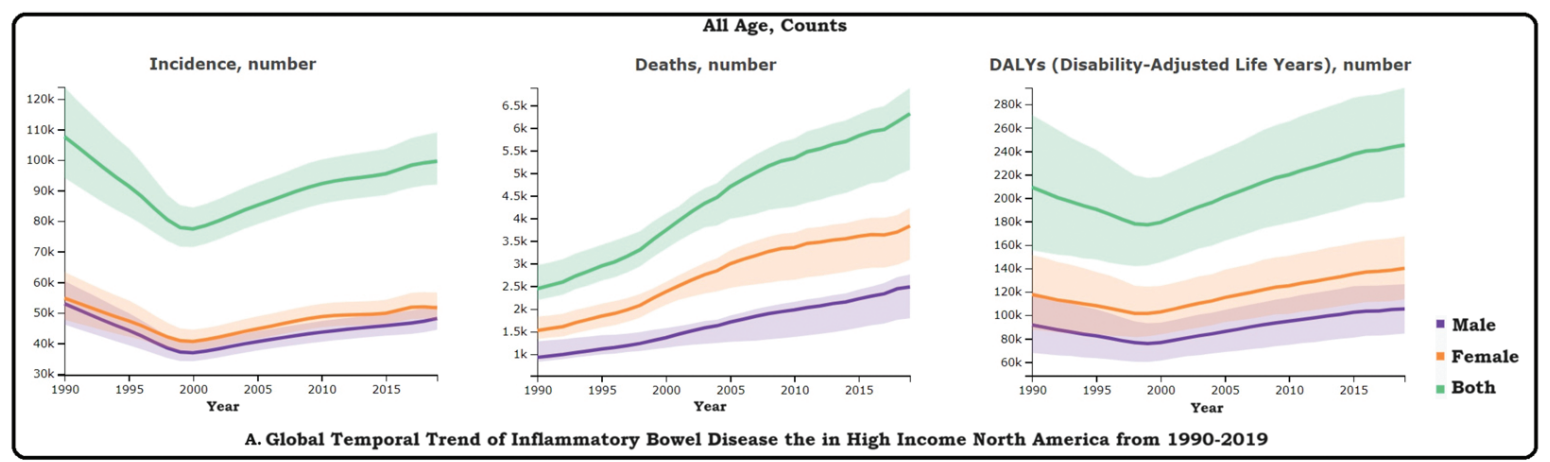
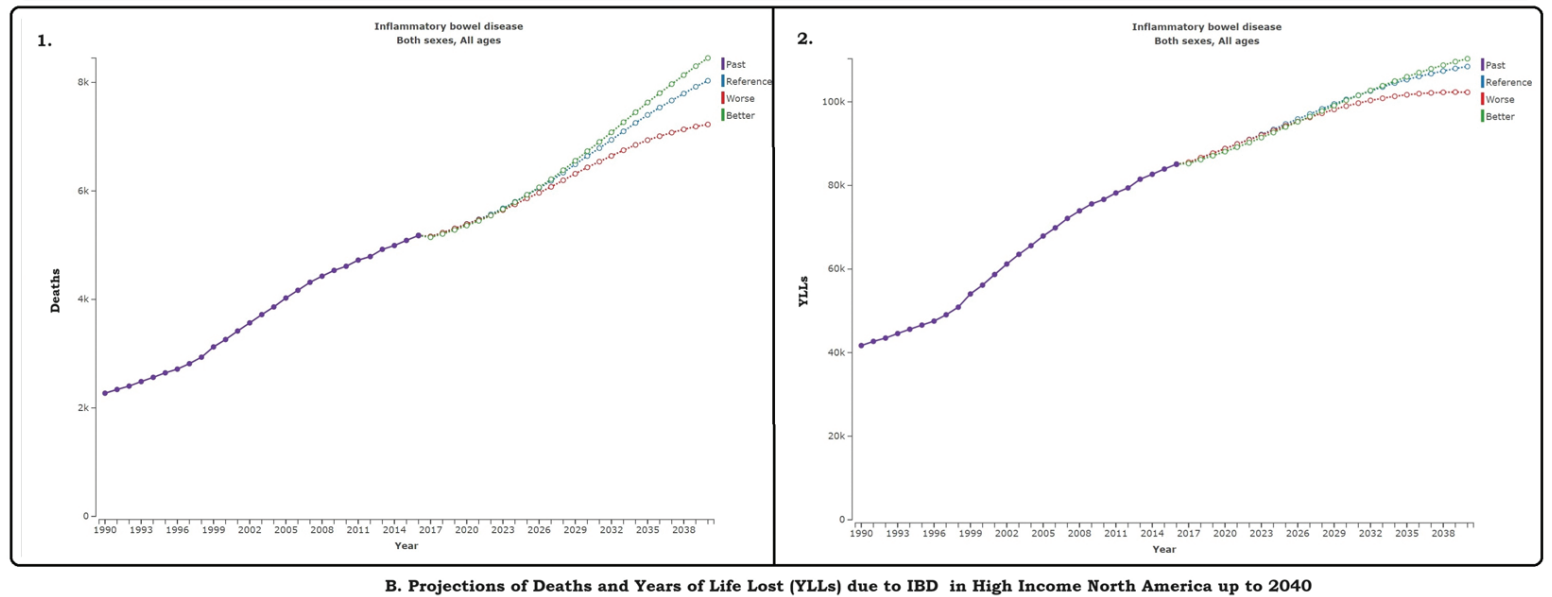
Methods: “Utilizing Global Burden of DIsease tool, we estimated IBD prevalence, incidence, mortality, and Disability Adjusted Life Years (DALYs) of IBD in High-Income North America. Standardized statistical techniques facilitated comparisons by age, sex, year within this specific region. The DisMod-MR 2.1 tool was employed to estimate incidence and prevalence, while mortality rates were discerned using the Cause of Death Ensemble Model (CODEm). Additionally, we projected the deaths and Years of Life Lost (YLLs) up to 2040 using regression analysis.”
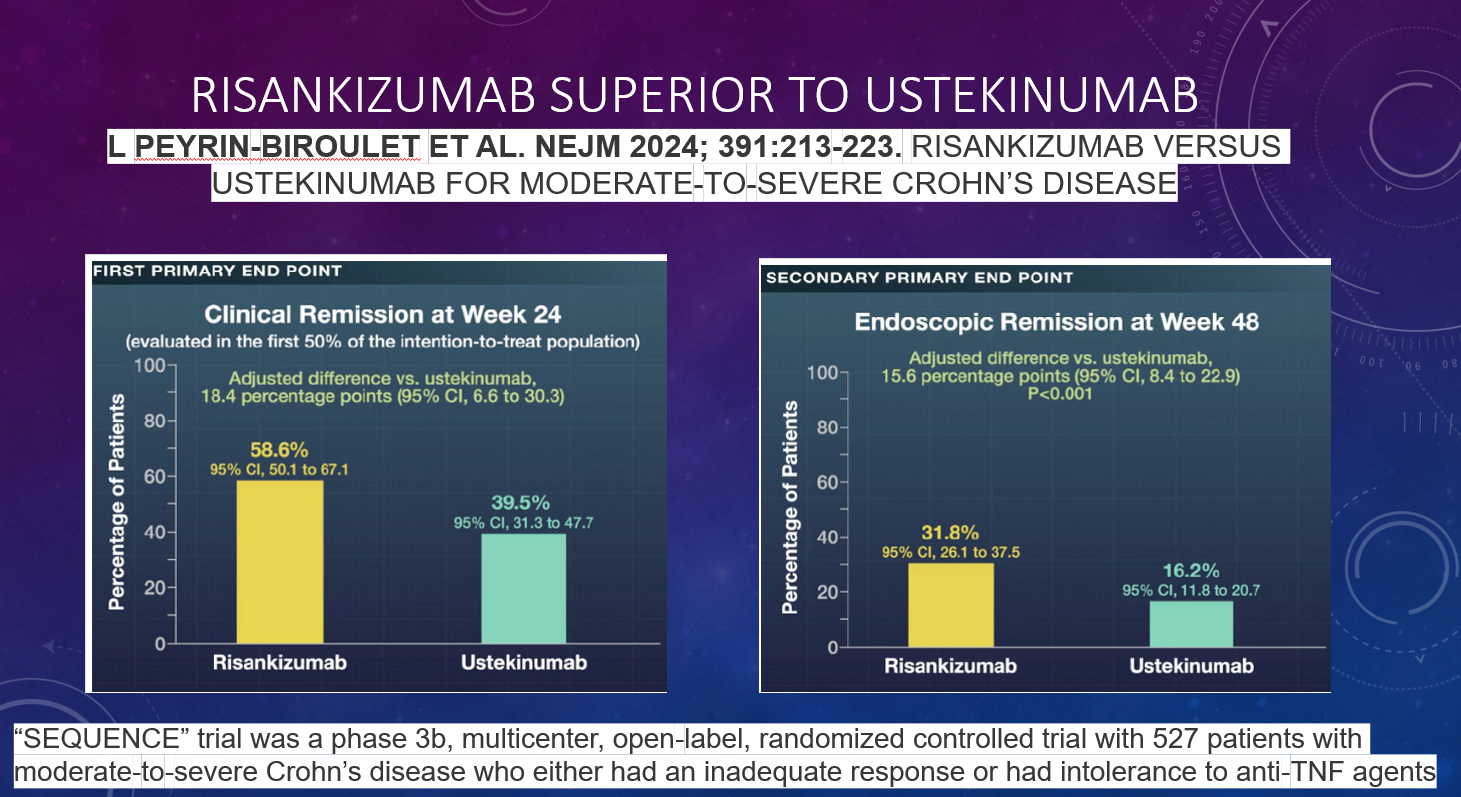
D Alsoud et al Inflamm Bowel Dis 2024; izad315, https://doi.org/10.1093/ibd/izad315. Real-world Effectiveness and Safety of Risankizumab in Patients with Moderate to Severe Multirefractory Crohn’s Disease: A Belgian Multicentric Cohort Study
Methods: Data from consecutive adult CD patients who started risankizumab before April 2023 were retrospectively collected at 6 Belgian centers. A total of 69 patients (56.5% female, median age 37.2 years, 85.5% exposed to ≥4 different advanced therapies and 98.6% to ustekinumab, 14 with an ostomy) were included.
Key findings:
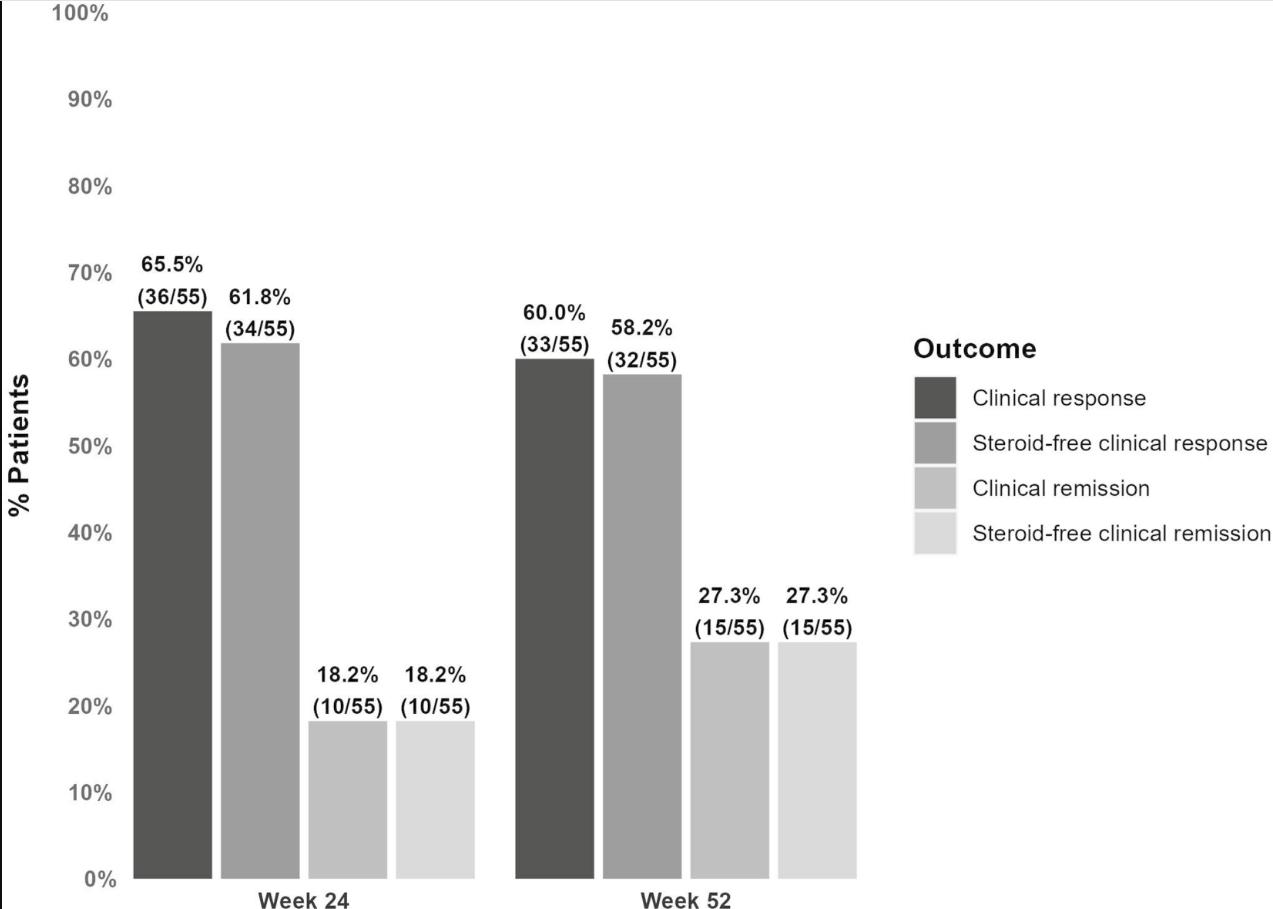
At week 24, 61.8% (34 of 55) and 18.2% (10 of 55) of patients without an ostomy achieved steroid-free clinical response and remission, respectively.
At week 52, these numbers were 58.2% (32 of 55) and 27.3% (15 of 55), respectively. Endoscopic data were available in 32 patients, of whom 50.0% (16 of 32) reached endoscopic response within the first 52 weeks.
Results in patients with an ostomy were similar (steroid-free clinical response and remission, 42.9% and 14.3%, respectively).
20.3% (14 of 69) of patients underwent CD-related intestinal resectionsand 18.8% (13 of 69) of patients discontinued risankizumab during followup (median 68 weeks).
Risankizumab was well tolerated with no safety issues.
Discussion points: “98.6% of patients in the current study were exposed to ustekinumab compared with less than 20% in the registration trials. This indicates that a previous lack or loss of response to the inhibition of the p40 subunit common to IL-12 and IL-23 does not preclude a potential response from subsequent selective inhibition of IL-23. “
My take: This study shows that risankizumab can be effective in refractory patients, even in those who have received similar type medications (eg. ustekinumab).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
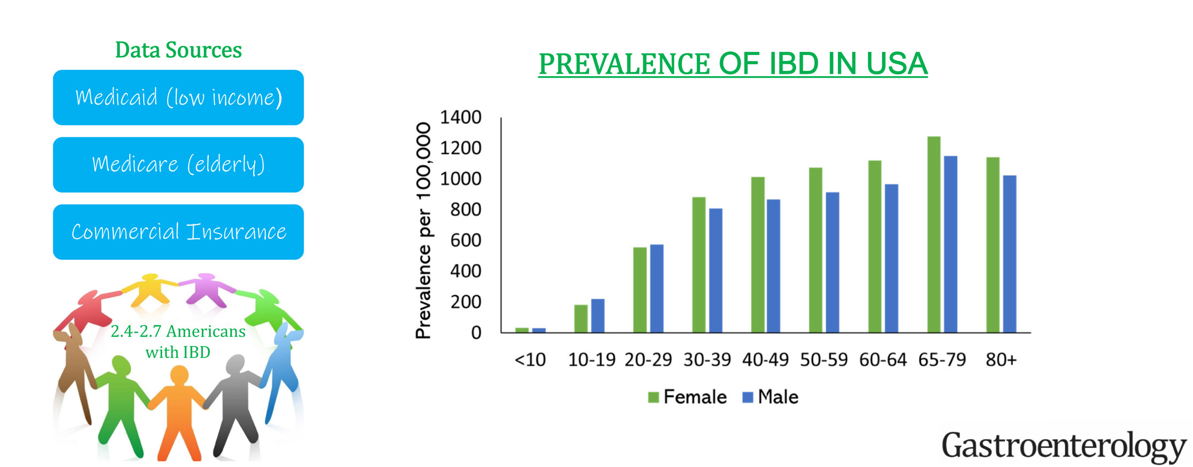
This “INPUT” (INcidence, Prevalence, Treatment and OUTome in Patients with IBD) study used 4 different data sets to provide “the clearest depiction to date of IBD [epidemiology] in the U.S.
Key findings:
The age-, sex- and insurance-standardized prevalence of IBD was 721 per 100,000 population. This equates to estimated 2.39 million Americans with IBD.
Sub-category prevalence: the prevalence of IBD per 100,000 population was 812 in White, 504 in Black, 403 in Asian, and 458 in Hispanic Americans.
My take: The prevalence of IBD continues to increase and the U.S. has one of the highest rates in the world.
In this prospective cohort with 369 patients, treatment included the following 113 infliximab, 133 vedolizumab, and 123 ustekinumab. All patients received standard dosing (eg. 5 mg/kg/dose every 8 weeks with infliximab). Per Table 1, dose of thiopurine was 100 mg (range 50-150, “using a 2:1 ratio of azathioprrine and mercaptopurine”); most patients received methotrexate at a dose of 12.5 mg. Key findings:
Infliximab levels were much improved in patients receiving combination therapy with either a thiopurine or methotrexate. In those patients receiving a thiopurine, a threshold of 6-TGN ≥146 was considered optimal.
Patients receiving combination therapy with methotrexate or a thiopurine and a 6-TGN concentration ≥146 pmol per 8 × 108 RBCs, and those with baseline infliximab level ≥12.3 μg/mL had a lower rate of secondary nonresponse when compared with those on monotherapy, thiopurine with 6-TGN <146 pmol per 8 × 108 RBCs, and baseline infliximab level <12.3 μg/mL (88.2 vs 11.8% [P = .04], 71.2 vs 45.5% [P = .04])
Ustekinumab and vedolizumab levels were NOT increased in patients receiving an immunomodulator
My take: This study reinforces the idea that there are pharmacokinetic benefits of combination therapy with infliximab (and extrapolated to other anti-TNF agents); there is a lack of benefit for most patients receiving ustekinumab and vedolizumab. Even with ustekinumab and vedolizumab, it is possible that patients with more severe disease may still benefit independent of pharmacokinetic effects on biologic agent.
Higher doses of infliximab monotherapy with therapeutic drug monitoring may achieve similar results as combination therapy. However, patients switching from one anti-TNF to another due to immunogenicity/antidrug antibodies are particularly likely to benefit from combination therapy. In addition, a recent ImproveCareNow study showed better outcomes for pediatric patients who received methotrexate with adalimumab (see below).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.