Outcomes of VEO-IBD. B Kerur et al. Inflamm Bowel Dis 2021; 27: 295-302. Bowel Disease in North America: A Retrospective Cohort Study The study population included 269 children (105 [39%] Crohn’s disease, 106 [39%] ulcerative colitis, and 58 [22%] IBD unclassified). Key findings:
- By the end of follow-up, stricturing/penetrating occurred in 7 (6.6%) children.
- Median age at diagnosis was 4.2 years. 71 (26%) were ❤ yrs.
- Only 5 (1.7%) had a coexisting immunological disorder.
- Over 5 years, cumulative use of an immunomodulator and biologic was 61% and 41% respectively. Exclusive enteral nutrition was used in 10 children (4%).
- 11.5% (n=19) had a change in diagnosis from UC/IBD-U to Crohn’s disease
- The risk of any bowel surgery in Crohn’s disease was 3% by 1 year, 12% by 3 years, and 15% by 5 years and did not differ by age at diagnosis.
- The risk of colectomy in ulcerative colitis/IBD unclassified was 0% by 1 year, 3% by 3 years, and 14% by 5 years and did not differ by age of diagnosis.
Related blog posts:
- Very Useful VEO-IBD Position Paper
- Patterns and Puzzles with VEO-IBD This is a very good review and the image on this day has one of my favorite patient t-shirts.
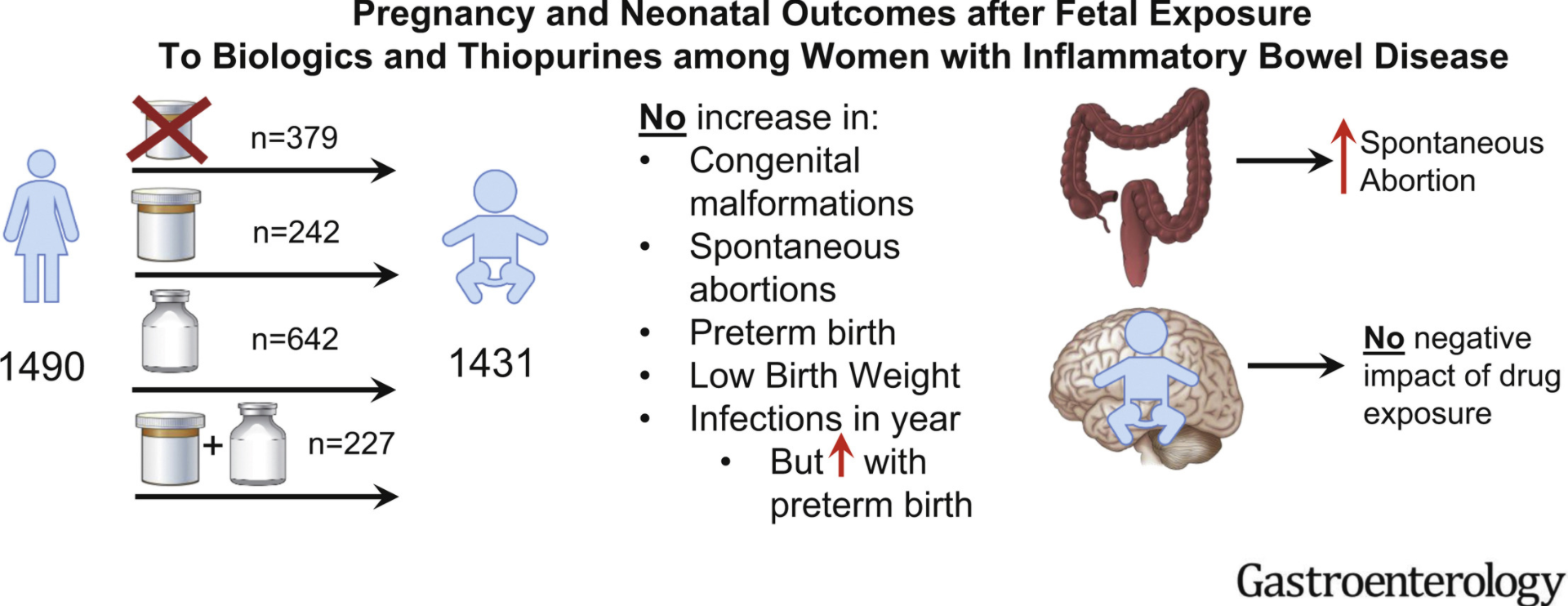
IBD Therapies and Newborn Outcomes (also covered in a prior blog post: Disease Activity, Not Medications, Linked to Neonatal Outcomes in Women with IBD). U Mahadevan et al. Gastroenterol 2021; 160: 1131-1139. Pregnancy and Neonatal Outcomes After Fetal Exposure to Biologics and Thiopurines Among Women With Inflammatory Bowel Disease
In this PIANO study (2007-2019), pregnant women with IBD were enrolled in a prospective, observational, multicenter study across the United States. PIANO is an acronym for Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes.
Disparity Not Apparent Among Insured Population. EL Barnes et al. Inflamm Bowel Dis 2021; 27: 364-370. Black and White Patients With Inflammatory Bowel Disease Show Similar Biologic Use Patterns With Medicaid Insurance
In this study, which analyzed Medicaid Analytic eXtract data from 4 states (California, Georgia, North Carolina, and Texas) between 2006 and 2011, the authors identified 14,735 patients with IBD (4672 black [32%]). Key finding: “In patients with Medicaid insurance, where access to IBD-specific therapy should be similar for all individuals, there was no significant disparity by race in the utilization of IBD-specific therapies.”