I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Key findings from this double-blind randomized controlled trial (n=121):
ICU admissions were 9.8% in LR group compared with 25% of NS group (RR 0.4, CI 0.2-0.9)
Quicker discharge with 44% at 72 hrs in LR group compared with 28% in NS group
Median length of stay was 3.5 days (LR group) compared with 4.6 days (NS group)
Critique of study from editorial: “The strengths of their study include a well-designed protocol, reasonable sample size and inclusion of patients within 8 hours of diagnosis; thus, fluids were administered during the critical period when there is a window of opportunity to restore the intravascular volume and maintain adequate tissue perfusion. However, the study included patients with mild pancreatitis. Another issue is that the benefit shown was for secondary outcomes and, thus, these results should be taken as exploratory and hypothesis generating.”
My take: For now, lactated ringer’s is the fluid of choice in individuals with acute pancreatitis.
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
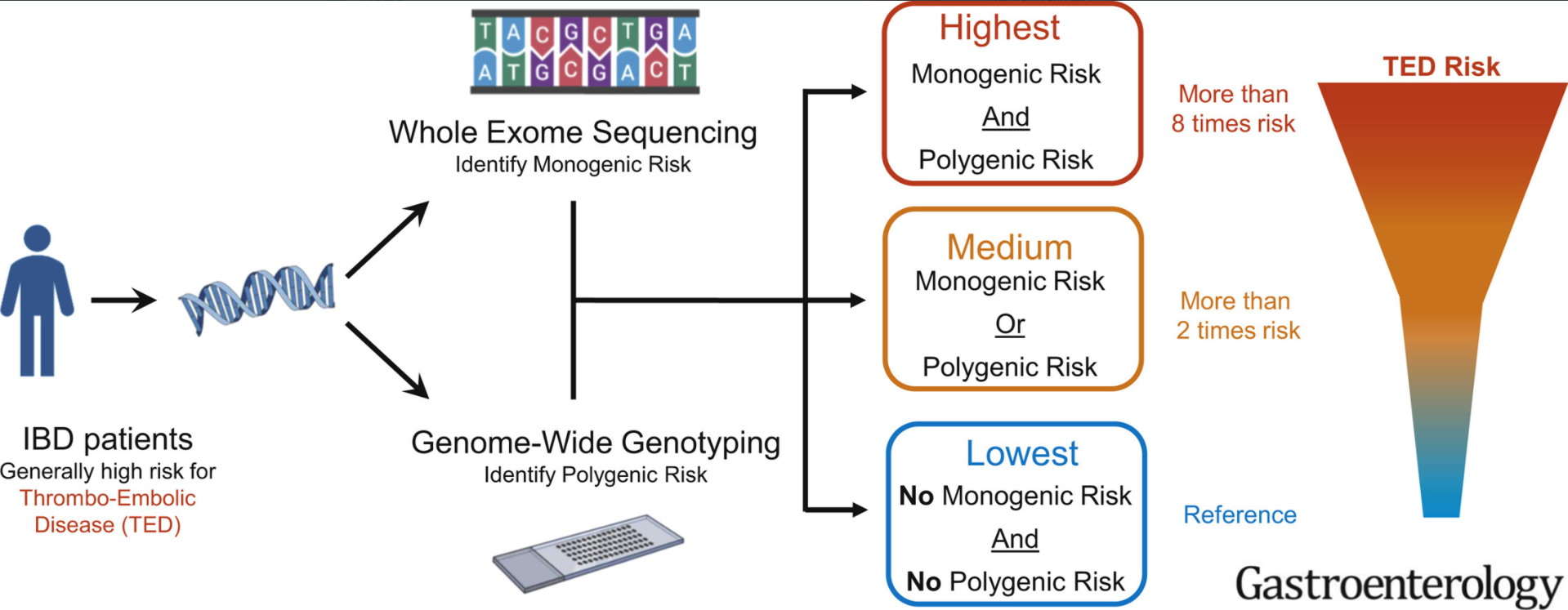
Background: 10% of healthy subjects are genetically at high risk for thromboembolic disease (TED). For adults with inflammatory bowel disease, TED is “largest cause of mortality in patients”
Key findings:
In total, this retrospective study had 792 IBD patients who had both whole-exome sequencing and genotyping data to identify thrombophilia pathogenic variants. 122 of 792 IBD patients (15.4%) as genetically high risk for TED.
Genetic TED risk was significantly associated with increased TED event (odds ratio,2.5; P ¼ .0036).
Patients with high TED genetic risk more frequently had thrombosis at multiple sites (78% vs 42%, odds ratio, 3.96; P ¼ .048)
“Our analyses demonstrate that approximately 1 in 7 patients with IBD have odds 2.5 times higher than nongenetically high-risk patients with IBD for experiencing TED.” The risk of TED in IBD is generally 3- to 4-fold higher than the general population
My take: In children, the risk of clots is much lower than in adults. Thus, the potential to identify those at highest risk would be useful in order to target interventions. Also, patients at higher risk for TED may affect choice of treatment (eg. avoiding JAK inhibitors).
70 patients completed the trial (44 PSC, 24 PBC, 2 SSC) (SSC =secondary sclerosing cholangitis). Treated patients received bezafibrate 400 mg once a day for 21 days.
For the primary end point, bezafibrate led in 45% (41% PSC, 55% PBC) and placebo in 11% to >/=50% reduction of severe or moderate pruritus (P ¼ .003).
Bezafibrate also reduced serum alkaline phosphatase (35%, P ¼ .03 vs placebo) correlating with improved pruritus (VAS, P ¼ .01) suggesting reduced biliary damage.
Serum bile acids and autotaxin activity remained unchanged.
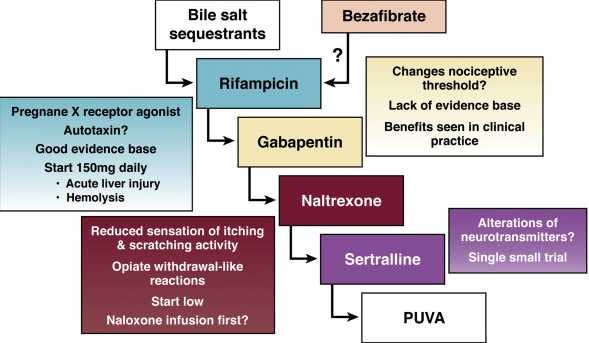
My take: While the majority of patients did not reach the primary end point, bezafibrate merits further investigation and may be a useful agent for pruritus in the setting of cholestatic liver disease. From the associated editorial (pg 649, JK Dyson et al. Bezafibrate for the Treatment of Cholestatic Pruritus: Time for a Change in Management?): “FITCH is an important study and provides novel and important data. It suggests that bezafibrate can be part of the answer to cholestatic pruritus.”
From Editorial:
“Current treatment ladder for pruritus and the potential positioning of bezafibrate in the future.“
Cases of alcoholic liver disease — which includes milder fatty liver and the permanent scarring of cirrhosis, as well as alcoholic hepatitis — are up 30% over the last year at the University of Michigan’s health system, says Dr. Jessica Mellinger, a liver specialist there….
This study had 42 patients who had alcohol detectable in blood and/or urine matched with 84 controls among patients who received liver transplantation for alcohol-associated liver disease (ALD); this study had a median follow-up of 12.9 years..
Key findings:
Long‐term survival was not different between the groups; however, rates of recurrent cirrhosis and cirrhosis‐related deaths were more frequent in the alcohol consumption group
Relapse to any alcohol consumption rate was higher in the case group (59.5%) than in the control group (38.1%, odds ratio 2.44; CI95% = [1.13; 5.27]), but sustained excessive consumption was not significantly different between the groups (33.3% versus 29.8% in case and control groups respectively, χ2 = 0.68).
My take: Yikes.! Fortunately, alcohol consumption is not a significant factor in pediatric liver disease. For adult hepatologists, this study highlights the need for patient support due to the frequency of alcohol relapse.
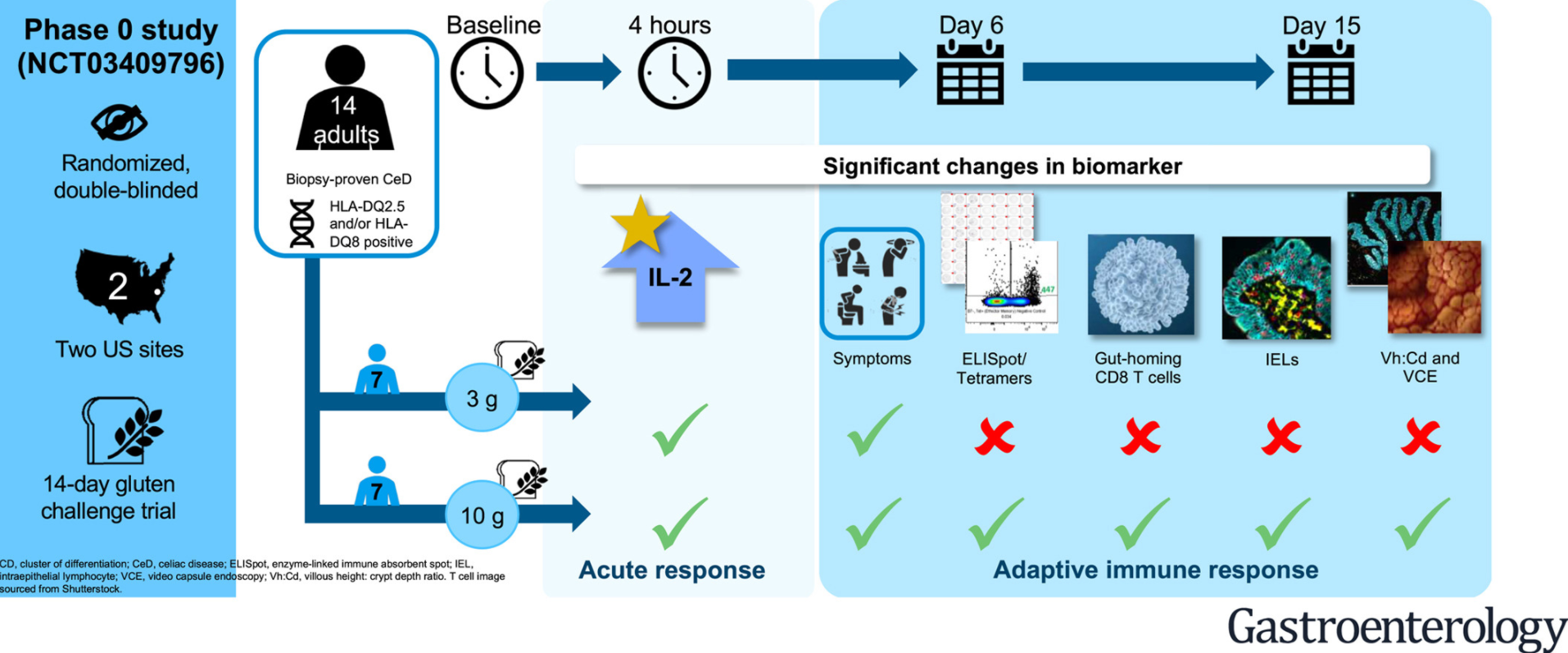
This study consisted of 14 adults with biopsy-proven celiac disease (CD) who were randomized to 3 g or 10 g gluten/day intake for 14 days. Each participant underwent extensive studies to detect histological, visible, and biochemical changes associated with gluten introduction. Data required multiple endosopic duodenal biopsies, VCEs and blood collection.
Key findings:
Symptoms and plasma interleukin-2 levels “increased significantly or near significantly at both doses.”
Interleukin-2 appeared to be the earliest, most sensitive marker of acute gluten exposure. IL-2 increases were observed 4 hours after exposure in patients with CD but not in healthy controls.
Intestinal damage is more complex and requires a longer duration and higher dose of gluten exposure. In this study, the higher dose (10 g) of gluten exposure was required for enteropathy within the study time frame.
My take: These study findings need to be confirmed in a broader patient cohort. However, in patients needing a gluten challenge, IL-2 response after a single-dose (measured at 4 hours) could be helpful. Those without IL-2 response are unlikely to have CD. Those with an IL-2 response at 4 hours, could confirm CD by completing a gluten challenge.
Diverticulitis is rarely seen in the pediatric age group. Over the course of nearly 30 years, I have encountered two cases; though, many of my partners with longer clinical experience have seen none.
Best Practice Advice 1: Computed tomography should be considered to confirm the diagnosis of diverticulitis in patients without a prior imaging-confirmed diagnosis and to evaluate for potential complications in patients with severe presentations. Imaging should also be considered in those who fail to improve with therapy, are immunocompromised, or who have multiple recurrences and are contemplating prophylactic surgery in order to confirm the diagnosis and location(s) of disease.
Best Practice Advice 3: After an acute episode of diverticulitis, colonoscopy should be delayed by 6–8 weeks or until complete resolution of the acute symptoms, whichever is longer. Colonoscopy should be considered sooner if alarm symptoms are present.
Best Practice Advice 5: A clear liquid diet is advised during the acute phase of uncomplicated diverticulitis. Diet should advance as symptoms improve.
Best Practice Advice 7: Antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a C-reactive protein >140 mg/L or baseline white blood cell count > 15 × 109 cells/L. Antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan.
Best Practice Advice 9: To reduce the risk of recurrence, patients with a history of diverticulitis should consume a high-quality diet, achieve or maintain a normal body mass index, be routinely physically active, and not smoke. Additionally, patients with a history of diverticulitis should avoid regular use (2 or more times per week) of nonsteroidal anti-inflammatory drugs except aspirin prescribed for secondary prevention of cardiovascular disease.
Methods: Sixteen callers, aged 17 to 23 years, were briefly trained in empathetic conversational techniques. Each called 6 to 9 participants over 4 weeks daily for the first 5 days, after which clients could choose to drop down to fewer calls but no less than 2 calls a week.
Key finding: A layperson-delivered, empathy-oriented telephone call program reduced loneliness, depression, and anxiety compared with the control group and improved the general mental health of participants within 4 weeks.
Advances in Cystic Fibrosis (CF) have led to improvement in longevity, now ~46 years in 2019
Newer CFTR modulator therapies need to be aligned to the specific mutations. With new therapies, a high calorie diet may not be required and instead follow a standard healthy balanced diet.
These agents appear to be driving a big drop in hospitalizations
Now some patients need counseling for obesity and NAFLD
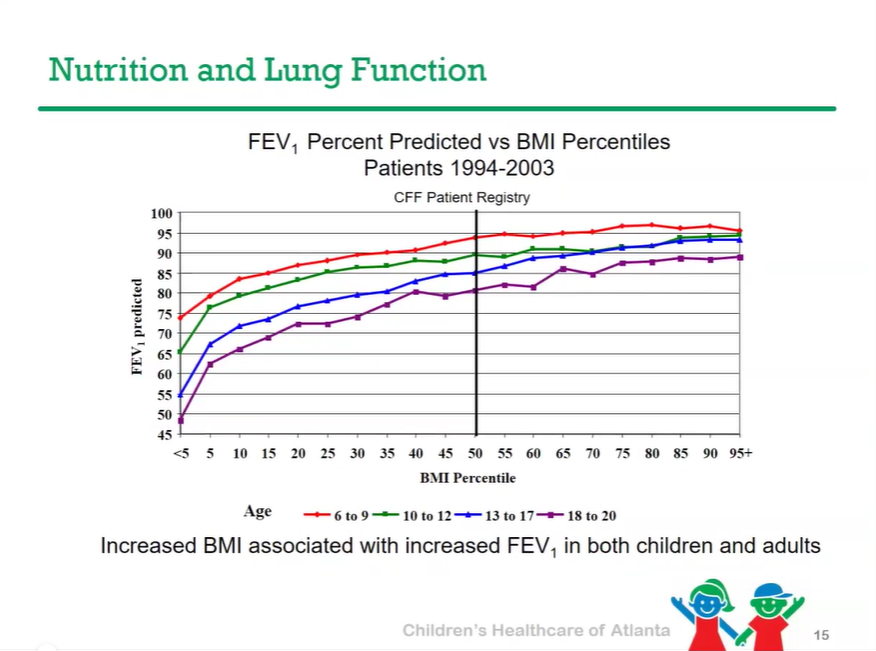
Better nutrition has been linked to better lung outcomes.
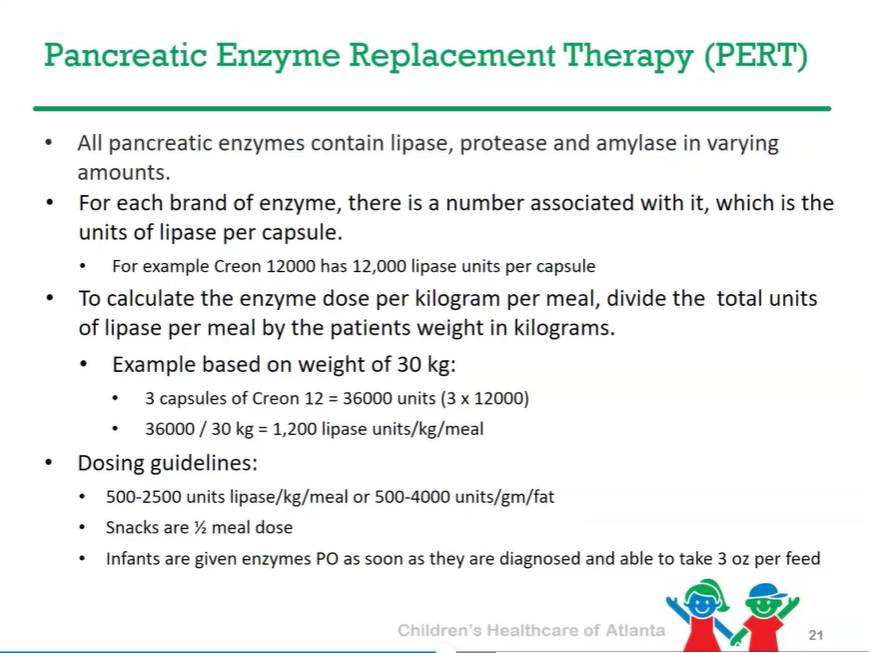
Pancreatic enzyme replacement therapy needed for 85-90% of patients with CF
CFTR modulator therapies may allow lower dosing PERT dosing
Fat soluble vitamin supplementation (A, D, E, K) is needed
Vitamin D (25-OH) goal (by CF Foundation) is >30 ng/mL
High salt diet is recommended due to excessive losses
Targeted nutritional support needs to be based on nutritional status; some patients may need G-Tube placement. CHOA algorithm developed.
High sugar diet may increase the development of CF related diabetes (CFRD)
Fibrosing colonopathy is a very rare effect of high dose pancreatic enzymes and may have been in part due to impurities in older preparations of panrcreatic enzymes.