About gutsandgrowth
I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
The clever title is derived from an editorial (KE Burke, AN Ananthakrishan. Clin Gastroenterol Hepatol 2019; 17: 1438-40) regarding three recent publications regarding Tofacitinib, a non-selective inhibitor of janus kinase (JAK) enzymes 1,2 and 3 which was FDA-approved in May 2018 for moderate to severe ulcerative colitis. This report was published prior to recent FDA warning regarding blood clots: FDA Warning on Tofacitinib
Two of the reports have been summarized previously on this blog:
The third study examines the safety of tofacitinib: W Sandborn et al. Clin Gastroenterol Hepatol 2019; 17: 1541-50
Methods: This study analyzed data from phase 2 and phase 3 trials with 1157 patients who had a median treatment of 1.4 years (1613 person-years). More than three-fourths were receiving 10 mg BID.
Findings:
- Serious infections were infrequent but there was a dose response relationship associated with herpes zoster infections. At 10 mg BID, the frequency was 5% whereas the rate was 1.5% in those receiving 5 mg BID and 0.5% in placebo-treated patients. This is likely related to interference of interferon production related to JAK inhibitor disruption.
- Sandborn et al conclude that the “safety profile of tofacitinib for patients with UC appeared similar to that reported for patients with rheumatoid arthritis and for patients with UC treated with biologic agents, except for the higher incidence rate of herpes zoster infection.”
The editorial recommends NOT using tofacitinib for acute severe ulcerative colitis (ASUC); it “should be encouraged only in selected patients and preferably in the context of a research study.” “Infliximab and cyclosporine [should be used] for steroid refractory UC;” however, they suggest that “one can consider initiating tofacitinib PRIOR to patients becoming steroid refractory. “It could be used upfront on day 1.”
Related blog posts -Tofacitinib:
Related blog posts -ASUC:

Ciutedella Park, Barcelona
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent retrospective study (J Webster et al. Clin Gastroenterol Hepatol 2019; 17: 1509-14) with 673 children with newly diagnosed (biopsy-proven) celiac disease (CD) (median age 10.6 y) evaluated DXA studies at time of diagnosis.
Key findings:
- Approximately 7% (n=46) had a low lumbar spine areal bone mineral density (aBMD) z-score (less than -2)
- Of those with abnormal aBMDs, 18 had repeat studies. 11 of 18 normalized after institution of dietary management. Mean time for repeat DXA was 2.3 years
- Of note, mean BMI z-score at time of repeat DXA was 0.005 (this includes 90 who had followup studies after a normal baseline DXA).
- Low body mass index (BMI) with z-score of -0.4 identified a >10% risk of an abnormal aBMD
The authors acknowledge than DXA screening is controversial. The current study’s strength is its large size. Limitations include the inability to correlate with clinical factors including adherence to a gluten-free diet.
My take:
- Based on this study, it is likely that only 2-3% of pediatric patients with celiac disease will have a persistently abnormal DXA after institution of a gluten free diet for 2 years; it is likely that even more will improve with time if receiving appropriate dietary treatment.
- I am not likely to recommend obtaining a baseline DXA study in pediatric patients with newly diagnosed celiac disease; the treatment for low bone mineral density in the setting of celiac disease is the same as for all children with celiac disease. If one were inclined to look for low BMD, optimal timing would likely be AFTER being adherent on a gluten free diet for at least two years particularly in those who had low BMI at presentation.
Related blog posts:

Columbus Monument, Barcelona
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
A recent case report described a patient who developed acute pancreatitis and acute kidney injury folllowing a competitive eating contest.



K Clarkston et al. JPGN 2019; 69: 68-74. This pediatric study with 72 children/young adults with Crohn’s disease examined infliximab trough levels; 70 received infliximab monotherapy & 88% received “standard” dose of 5 mg/kg
Key findings:
- Infliximab level ≥18 mcg/mL at week 6 was strongly associated with clinical and biologic response as well as achieving an infliximab level ≥5 mcg/mL at week 14 (AUC 0.85).
- A week 6 level ≥18 mcg/mL had 82% sensitivity, 82% specificity, 56% PPC, and 94% NPV for having a therapeutic level at 4th infusion.
- Median infliximab levels for clinical responders was 27.8 mcg/mL at 2nd infusion and 14 mcg/mL at 3rd infusion.
- The authors reported that only 22% of their cohort achieved a week 14 infliximab level ≥5 mcg/mL. The median infliximab level at this time point was 2.1 mcg/mL.
My take: In this study, the standard dose of infliximab (5 mg/kg) was not adequate in ~80% of patients in achieving a therapeutic trough level. If using the standard low-dose, it may be worthwhile to check a trough level prior to 3rd infusion or at week 10 to help determine if the level will be sufficient to start maintenance treatment at week 14 or whether an earlier infusion is warranted.
Related blog posts:

Barcelona
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
A recent study (JF Colombel et al. Clin Gastroenterol Hepatol 2019; 17: 1525-32) examines the effect of combination therapy and drug levels in achieving corticosteroid-free remission at week 26 (CSFR26).
The authors performed a post hoc analysis from 206 patients with Crohn’s disease (CD): 97 monotherapy with infliximab & 109 with combination infliximab/azathioprine
Key findings:
- The proportions of patients achieving CSFR26 were not significantly greater among those receiving combination therapy vs monotherapy within the same serum infliximab concentrations
- Mean trough infliximab concentrations in the combination therapy were higher than for monotherapy: 3.54 mcg/mL vs. 1.55 mcg/mL
- Higher levels of antidrug antibodies were seen with monotherapy: 35.9% vs 8.3% of those with combination therapy. Antidrug antibodies were detected only in those with lowest quartile of infliximab trough levels.
My take: This study indicates that combination therapy’s higher efficacy is due to favorable pharmacokinetics rather than drug synergy. If good infliximab trough levels can be achieved with infliximab monotherapy, this may obviate the need for combination therapy. The uncertain factor is whether closer attention to trough levels will minimize the development of antidrug antibodies as effectively as the use of combination therapy.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.

Sagrada Familia, Barcelona
In a recent study (A Fritscher-Ravens et al. Gastroenterol 2019; 157: 109-18) uses confocal laser endomicroscopy (CLE) for “real-time detection and quantification of changes in intestinal tissues” related to food challenges. The authors previously had used this technique in a feasibility study (Gastroenterol 2014; 147: 1012-20). In this study, two-thirds of patients with CLE+ IBS showed improvement of IBS symptoms after a 12-month exclusion diet.
In the current study, the authors prospectively examined patients (n=108 completed study) who had irritable bowel syndrome and were convinced that this was triggered by foods (with negative IgE food allergy testing). The CLE testing evaluated four food components
Key findings:
- 76 of 108 (70%) had abnormal CLE; 46 of these reactions were to wheat
- In those with CLE+ reactions, intraepithelial lymphocytes were significantly higher compared to those with CLE-negative (normal evaluations).
- Other biomarkers associated with CLE+ included increased claudin-2 expression from crypt to villous tip, lower levels of occludin, and higher eosinophilic cationic protein.
Abnormal CLE indicated abnormal mucosal appearance including formation of epithelial leaks/gaps and widening of the intervillous spaces after food challenge.
My take: This study shows that in individuals with a strong suspicion of food-triggered IBS, immediate reactions in the mucosa can be detected with CLE in more than 50%. Whether this type of approach could/should be developed for wider use in targeting a specific diet is unclear. More studies are needed.
Related blog posts:

Sagrada Familia, Barcelona
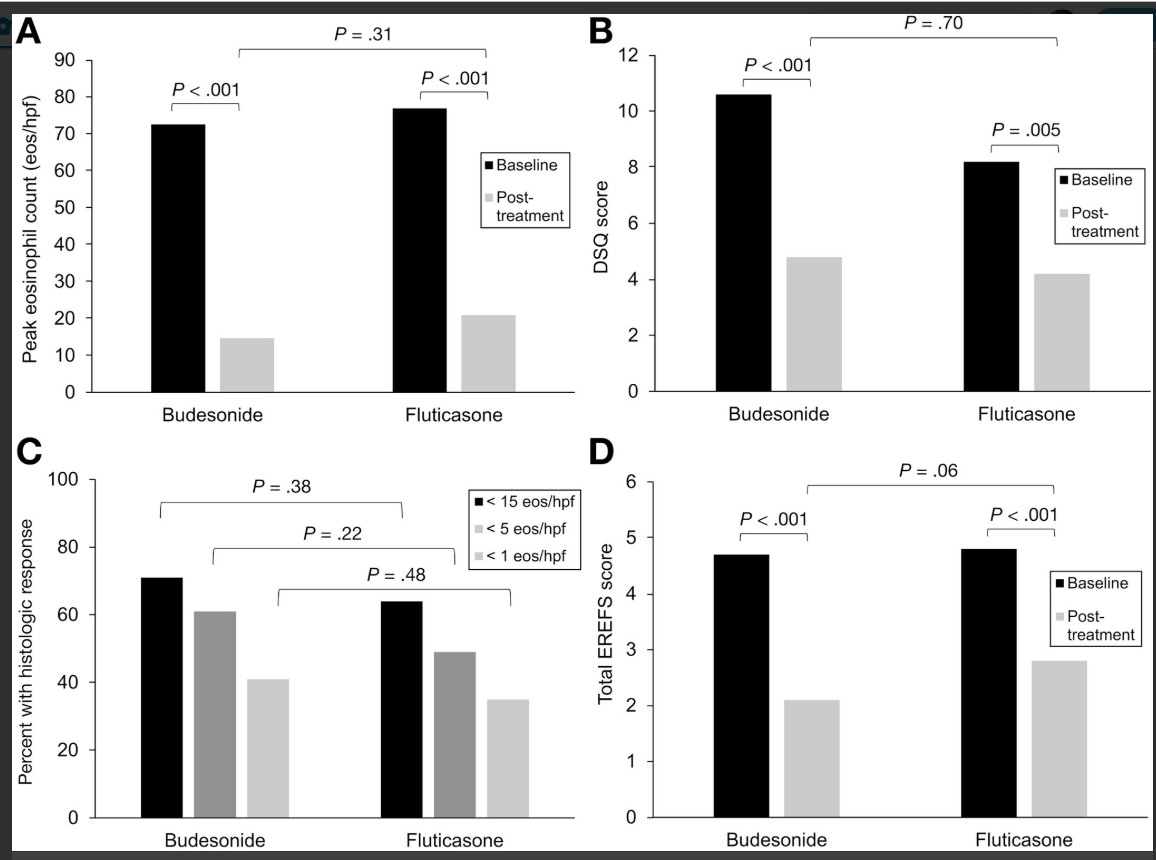
A recent double-blind, double-dummy study (ES Dellon et al. Gastroenterol 2019; 157: 65-73) found similar efficacy between budesonide and fluticasone for newly-diagnosed eosinophilic esophagitis. They had hypothesized that an oral viscous budesonide would be more effective due to increased esophageal contact time.
Methods: The authors compared an oral viscous budesonide OVB) at 1 mg BID (n=56) to fluticasone (swallowed) MDI dosed at 880 mcg BID (n=55). Patients aged 16-80 years, with mean of 37 years.
Baseline characteristics:
- ~95% in both groups with dysphagia
- ~75% with any atopic condition
- ~50% with dilatation required at baseline
Key findings:
- Similar drop in eosinophil count: 73 (OVB) and 77 (MDI) eos/hpf at baseline to 15 and 21 respectively
- Histologic response (<15 eos/hpf) rates of 71% (OVB) and 64% (MDI).
- Response to <5 eos/hpf occurred in 61% OVB and 49% MDI; response to <1 eos/hpf was noted in 41% and 35% respectively
- Symptom scores (DSQ) responded similarly as well
- Similar degree of candidiasis 12% for OVB and 16% for MDI
In the associated editorial, the authors speculate that one reason for similar efficacy was the detailed instructions given for patients taking the MDI.
My take: This study supports both topical steroid therapies; practical issues like cost and insurance coverage could be influential in selecting the specific treatment for an individual patient.
Related blog posts:

From AGA twitter feed
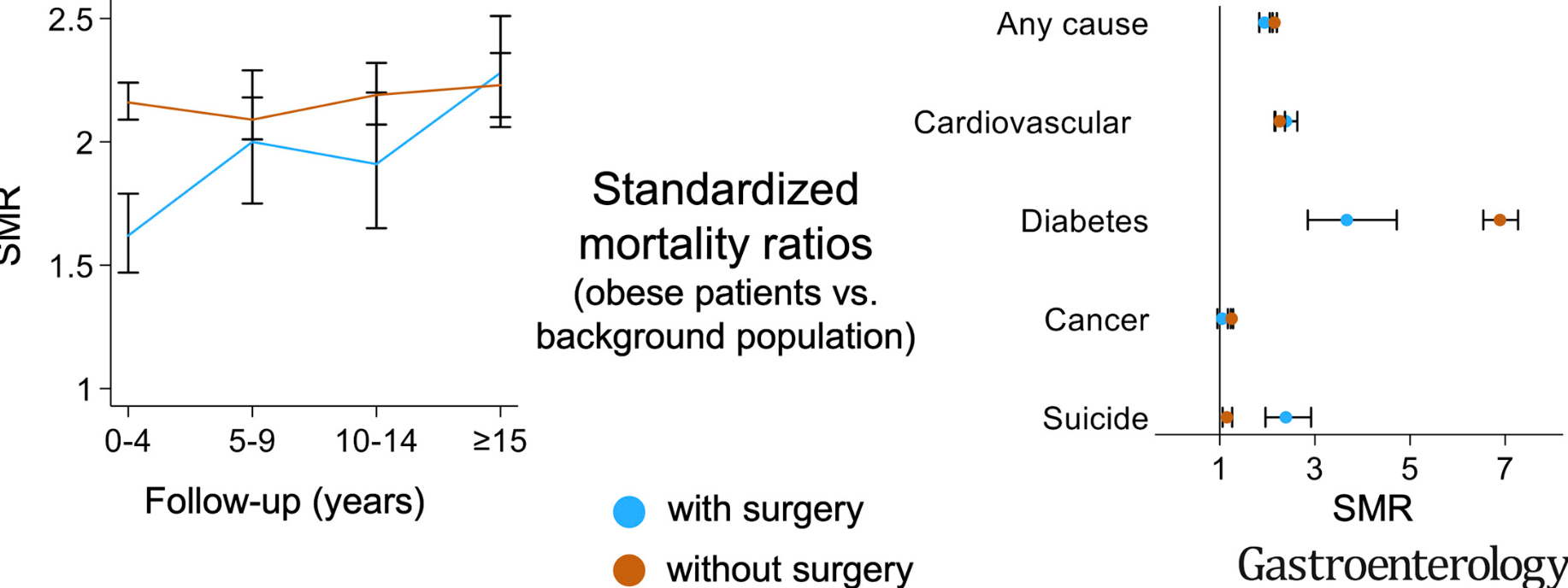
A recent population-based cohort study (JH Kauppila et al. Gastroenterol 2019; 157: 19-27) examined the effects of bariatric surgery on survival from Nordic countries between 1980-2012.
Link: Effects of Obesity Surgery on Overall and Disease-Specific Mortality in a 5-Country Population-Based Study
Among 505,258 obese individuals, 49,977 had bariatric surgery.
Key findings:
- Overall mortality rates were lower in the surgery group during the first 14 years but higher after 15 years (HR 1.20 with CI 1.02-1.42). Thus, overall, obese patients who underwent bariatric surgery had longer survival times than obese patients who did not have surgery. Both groups had higher mortality than the general population
- The improved survival compared to those without surgery was related to decreased mortality from cardiovascular mortality, diabetes and cancer. However mortality due to suicide was increased.
- Limitations: lack of detailed data including BMI, smoking and alcohol consumption

Graphical abstract (available online)
Related blog posts:
A recent randomized study (L Albenberg et al. Gastroenterol 2019; 157: 128-36) examined whether a diet low in red or processed meats could reduce rates of Crohn’s disease (CD) flares.
Methods: Adults with CD were recruited into the FACES (Food and Crohn’s Disease Exacerbation Study) trial from 2013 to 2015. Participants were recruited from an internet-based cohort (n=15,600). Eligible participants (consumed red meat at least once a week & in remission) were randomly assigned to high meat, n=118 (minimum of 2 servings per week) or low meat, n=96 (no more than 1 serving per month). Outcomes were based on changes in sCDAI scores or need for treatment (new medication or surgery)
Key findings:
- Any relapse occurred in 62% of participants in the high meat group compared to 42% in the low meat group. This was not statistically significant.
- At week 20, 18 participants in each arm had a stool calprotectin with the high meat group having a higher median: 74.5 mcg/g compared to 36.0 mcg/g (P=.13)
- The high meat group did consume at least 2 servings per week in 98.5% of observed weeks compared to 18.8% of the low meat group.
Limitations:
- Small number of diet participants
- Study was not blinded and only a subset included more objective markers of response
- Whether complete avoidance of red meat/processed meats would be more effective is unclear
- In those in remission at baseline, it could take longer for the benefits of a dietary intervention to become evident
My take: Limiting consumption of red and processed meats (particularly if meat is not lean) has been shown to have cardiovascular benefits. While this study does not show a statistically-significant improvement in relapse rates in this cohort with Crohn’s disease, there are still strong arguments that a diet with increased fruits/vegetables and less red/processed meats would be beneficial.
Related Blog Posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Sagrada Familia, Barcelona
From FDA: 7-26-19 FDA approves Boxed Warning about increased risk of blood clots and death with higher dose of arthritis and ulcerative colitis medicine tofacitinib (Xeljanz, Xeljanz XR)
An excerpt:
The U.S. Food and Drug Administration has approved new warnings about an increased risk of blood clots and of death with the 10 mg twice daily dose of tofacitinib (Xeljanz, Xeljanz XR), which is used in patients with ulcerative colitis…
Health care professionals should discontinue tofacitinib and promptly evaluate patients with symptoms of thrombosis. Counsel patients about the risks and advise them to seek medical attention immediately if they experience any unusual symptoms, including those of thrombosis listed above. Reserve tofacitinib to treat ulcerative colitis for patients who have failed or do not tolerate tumor necrosis factor (TNF) blockers. Avoid tofacitinib in patients who may have a higher risk of thrombosis. When treating ulcerative colitis, use tofacitinib at the lowest effective dose and limit the use of the 10 mg twice daily dosage to the shortest duration needed
- 19 cases of blood clots in the lung out of 3,884 patient-years of follow-up in patients who received tofacitinib 10 mg twice daily, compared to 3 cases out of 3,982 patient-years in patients who received TNF blockers
Related blog posts:

University of Virginia