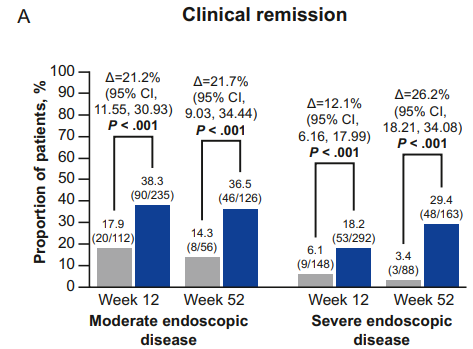
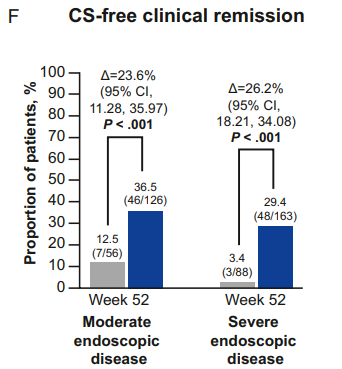
Methods: Efficacy end points were evaluated at Weeks 12 (pooled population) and 52 (ELEVATE UC 52)
Key findings:
Clinical remission in the moderate group compared to placebo: Week 12: 38.3% vs 17.9%; Week 52: 36.5% vs 14.3%
Clinical remission in the severe group compared to placebo: Week 12: 18.2% vs 6.1%; Week 52: 29.4% vs 3.4%
“Our findings were consistent with those for other UC treatments…with efficacy improvements generally being greater among patients who were naive rather than experienced with biologics and/or JAKi.12–17“
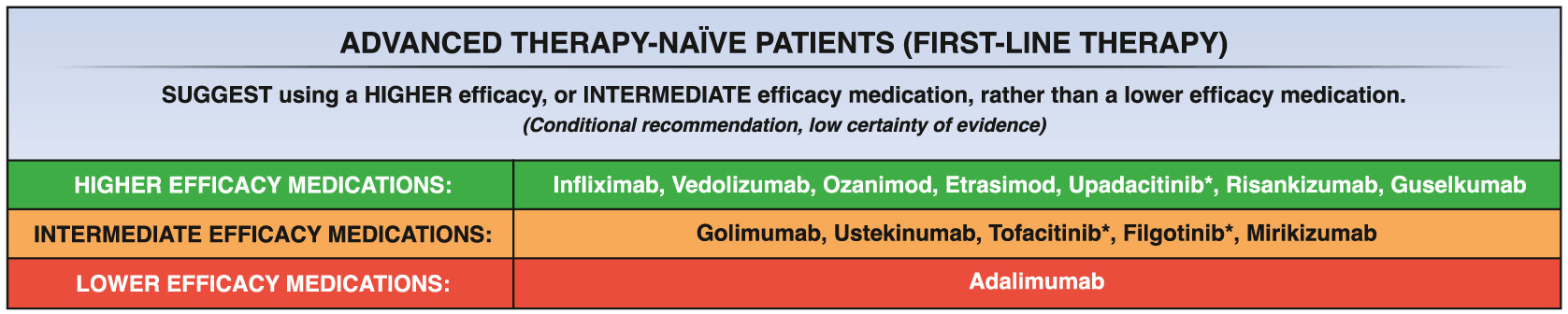
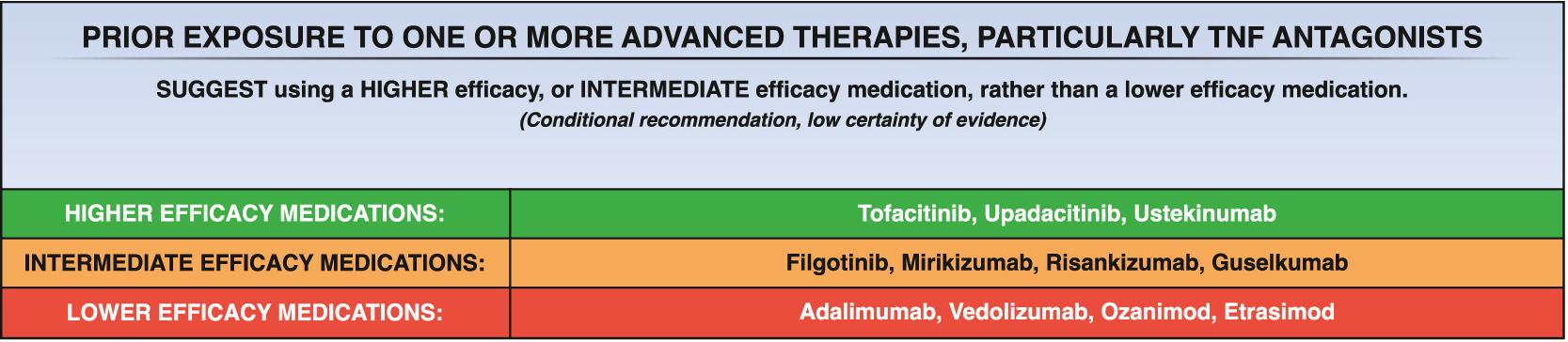
My take: Etrasimod demonstrated significant induction and maintenance efficacy over placebo in both moderate and severe endoscopic disease. Its role remains limited as there are other treatments with improved likelihood of response, especially in those with prior advanced therapies. However, it is notable that recent AGA guidelines promote etrasimod as one of the higher efficacy agents in patients naive to advanced therapies.
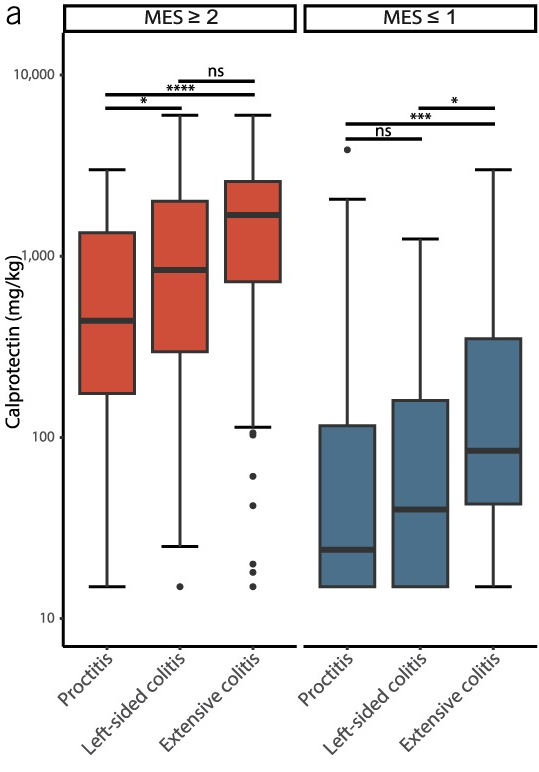
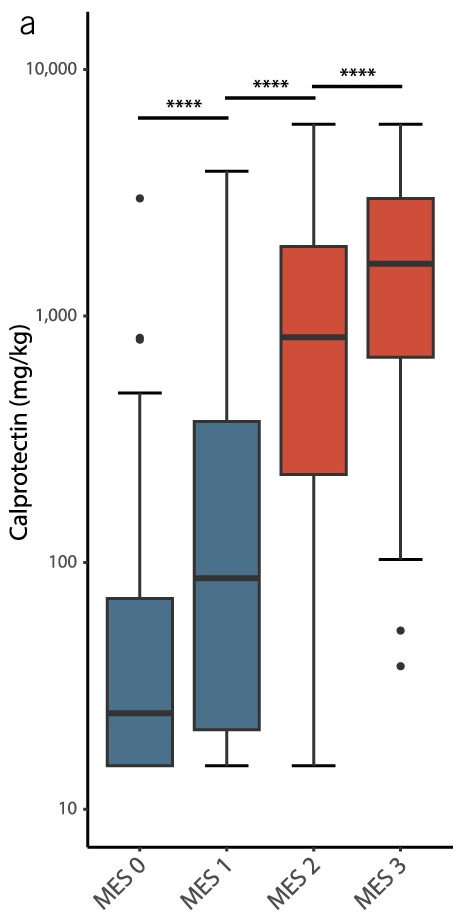
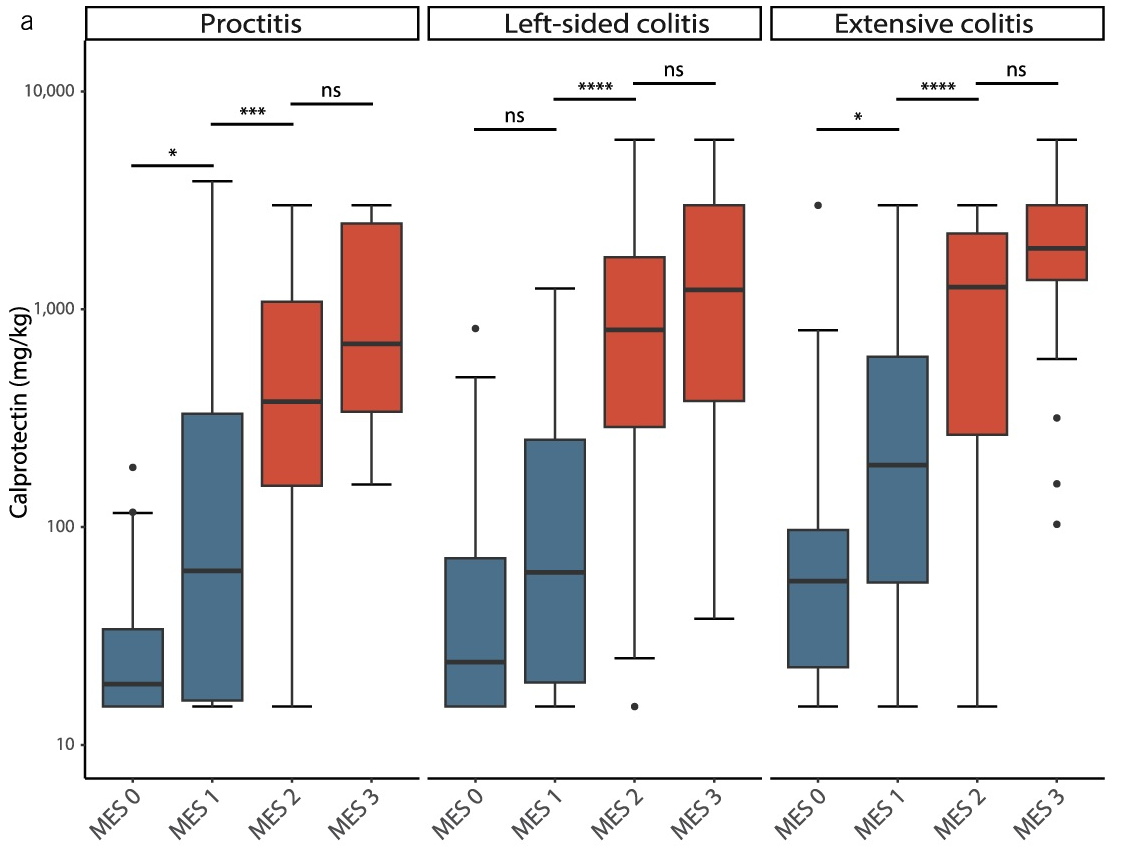
This single-center observational study (n=254) examined the correlation between fecal calprotectin (FC) levels with both disease extent and mucosal healing in ulcerative colitis. Mucosal healing was rated by the Mayo Endoscopic Score (MES).
Key findings:
Disease extent: FC levels were significantly lower in proctitis (440 mg/kg) as compared with left-sided colitis (840 mg/kg) or pancolitis (1,690 mg/kg)
Mucosal healing: In MES ≤1, FC levels were significantly lower in proctitis (24) compared to left-sided colitis (40) or pancolitis (85)
My take: Fecal calprotectin levels are clearly affected by the extent of disease involvement. However, the increase in calprotectin values associated with disease activity was significantly larger than the differences attributed to disease extent.
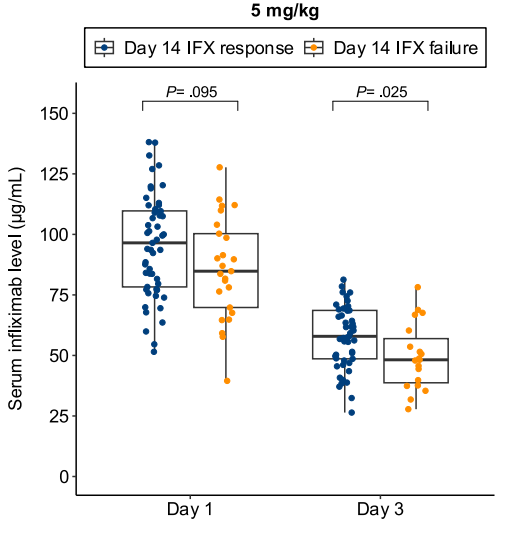
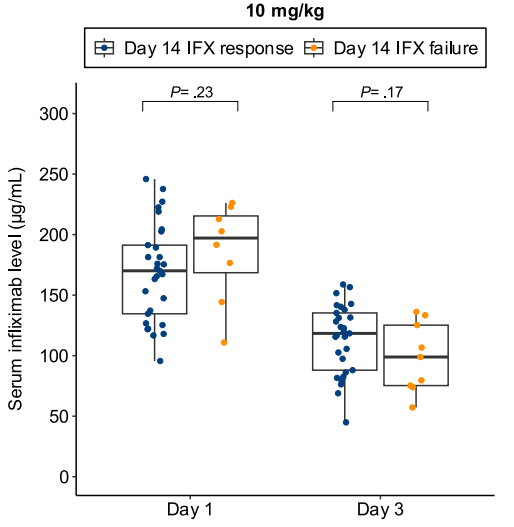
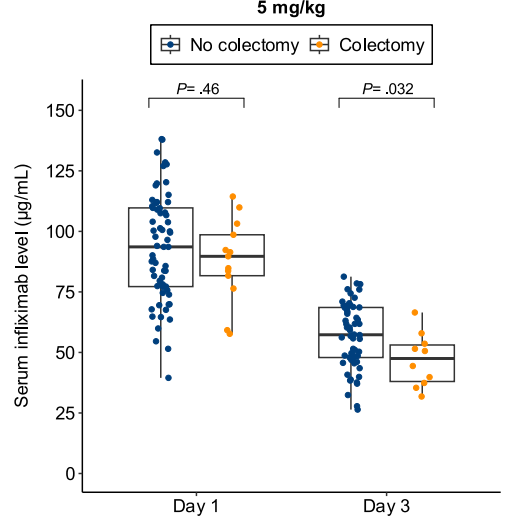
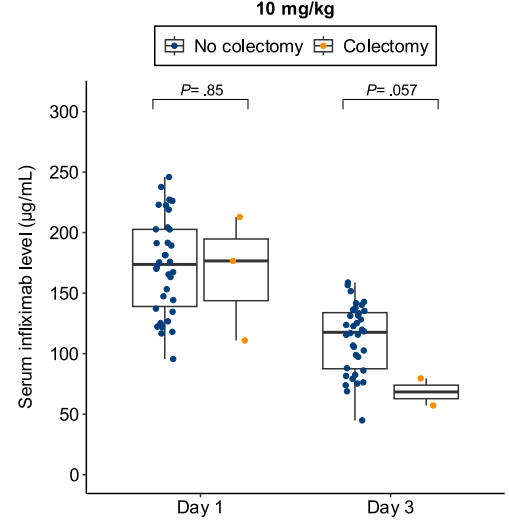
CFD Li Wai Suen et al.Gastroenterology, Volume 170, Issue 1, 118 – 131. Early Infliximab Levels and Clearance Predict Outcomes After Infliximab Rescue in Acute Severe Ulcerative Colitis: Results From PREDICT-UC
Methods: Data, including serum and stool testing, was extracted from from 135 patients (ages 24-42) enrolled in the PREDICT-UC prospective, randomized controlled trial
Key findings:
Lower day 3 serum infliximab levels predicted infliximab failure on day 14 and colectomy by 3 months; a threshold of ≤57.9 μg/mL had 83% sensitivity, 67% specificity, 24% positive predictive value, and 97% negative predictive value for colectomy
In patients with high clearance who did not respond to the first infliximab dose, day 14 response rate was higher with a second 10 mg/kg vs 5 mg/kg dose (38% vs 11%; risk ratio, 3.43)
Day 3 fecal infliximab levels correlated with endoscopic severity and was associated with day 7 nonresponse (P = .016)
Discussion points:
“Early infliximab levels and clearance predict outcomes in ASUC. Additionally, we are the first to demonstrate that a high early infliximab clearance can be overcome by additional dosing. These results demonstrate the potential of early infliximab TDM [therapeutic drug monitoring] to guide decision-making in ASUC and for the first time provide an evidence base for intensified infliximab dosing in clinical practice.”
My take: While the authors suggest TDM as a potential strategy to overcome low levels, an alternative approach would be using higher dosing and more frequent dosing, especially as infliximab levels may not be quickly available. Higher dosing is particularly important in the pediatric age group where studies have shown that “standard” dosing of 5 mg/kg result in insufficient levels of infliximab in ~80%.
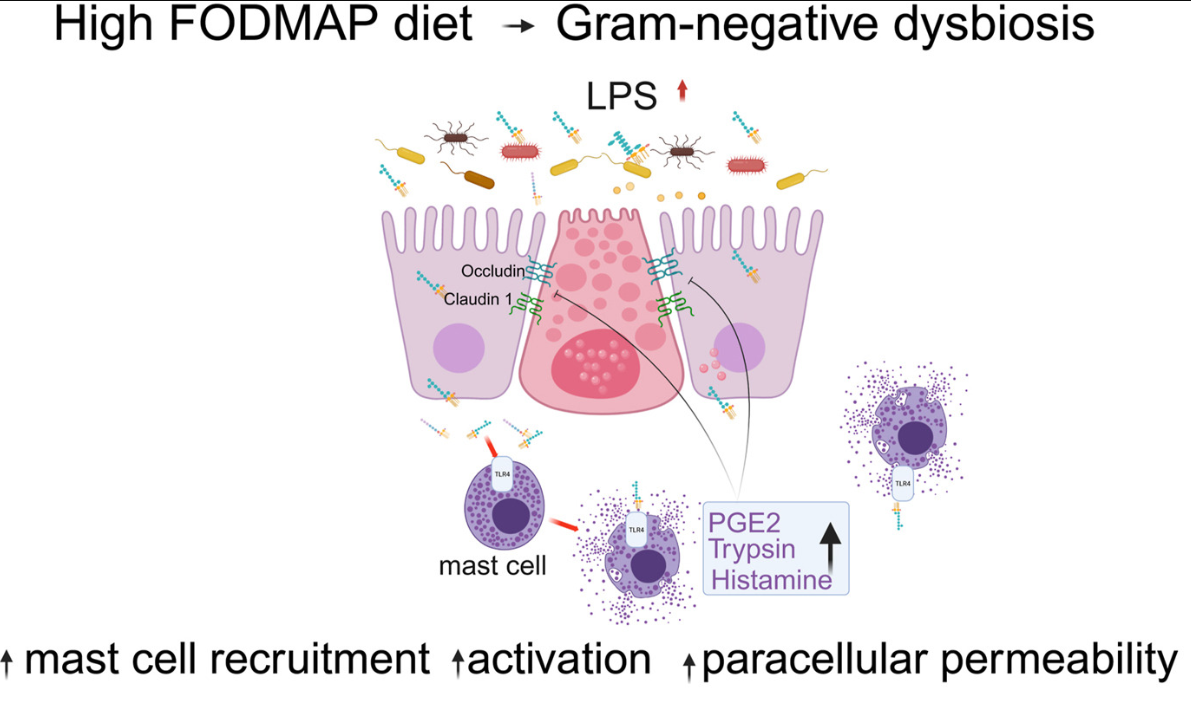
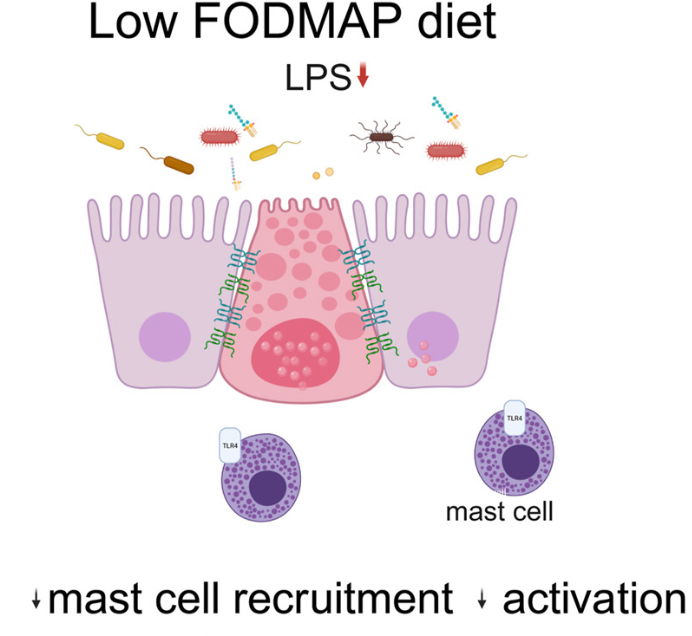
Background: “Mechanisms by which fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAPs) drive pathophysiology of irritable bowel syndrome (IBS) are not well understood.”
Methods: 42 patients with “Rome IV diarrhea-predominant IBS (IBS-D) underwent barrier function evaluation pre- and post-LFD along with assessment of mast cell number and activation profile. Finally, fecal supernatants (FS) were administered intracolonically to wild-type mice with and without pharmacologic inhibition, toll-like receptor 4 (tlr4)–/– mice, and mast cell-deficient mice with/without mast cell reconstitution.”
Key findings:
This is a highly technical study and would recommend reviewing the findings directly (open access article).
To summarize:
“Patients with IBS-D had significant improvement in colonic barrier structure and function, mast cell number, and levels of mast cell mediators post-LFD (low FODMAP diet). The magnitude of physiological changes did not correlate with the magnitude of clinical response.”
“This study showed the complex interplay among food, microbiome, local immune activation, and epithelial physiology in IBS by demonstrating that FODMAPs increase fecal lipopolysaccharide levels, which activates colonic mast cells to causes barrier dysfunction in diarrhea-predominant IBS.”
My take: By understanding the GI effects of a low FODMAP diet in patients with IBS-D more precisely, it may improve dietary approaches as well as other treatments like mast cell stabilizers.
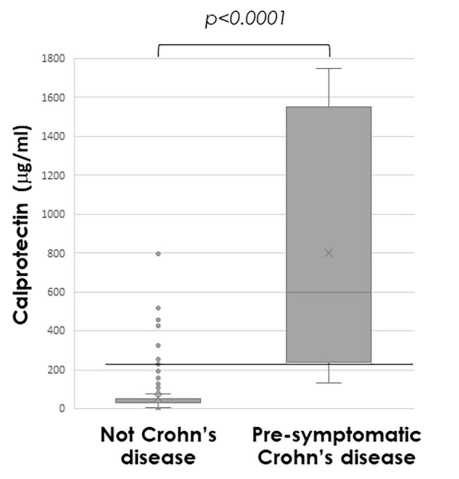
Methods: “Faecal calprotectin was measured in asymptomatic FDRs aged 6–38 years; those with persistent elevation, defined as >70 µg/g in at least two separate tests, were offered panenteric video capsule endoscopy or ileocolonoscopy”
Population: 331 (35%) first-degree relatives (FDRs) (from a group of 950) agreed to be screened: 63 (19%) had persistently elevated calprotectin, of whom 42 underwent further evaluation
Key findings:
From the initial screened cohort of 331 patients, nine (2.7%) had endoscopic appearance compatible with presymptomatic CD, and 22 (6.6%) had non-specific macroscopic mucosal changes
Median calprotectin was significantly higher in those with presymptomatic CD (772µg/g (IQR 279–1685)) compared with others (31µg/g (IQR 30–61), p<0.0001)
Calprotectin >225 µg/g predicted presymptomatic CD (area under the receiver operating characteristic curve 0.97 (95% CI 0.94 to 1.0; p<0.001; sensitivity 89%, specificity 94%)
Discussion Points:
“There is no universally accepted definition for preclinical stages of CD, and the distinction between these stages remains partly subjective.”
“The lack of longitudinal follow-up is also a limitation, but this will be completed as part of the PIONIR trial.”
My take (borrowed in part from the authors):
Identification of pre-symptomatic CD “can facilitate designing targeted interventions and defining inclusion criteria for prevention trials.” The disease may be more modifiable in the early stages of disease.
This trial suggests the calprotectin threshold of >70 is too low to target screening. For specificity, the study showed that persistent elevation above 225 merits investigation; though, it has been our practice to use a threshold of >150 for children older than 5 years.
Approximately 5% of asymptomatic FDRs of CD patients have evidence of pre-symptomatic CD and approximately 10% more have non-specific mucosal changes when evaluated
This article summarizes the recent changes in the treatment options for Clostridioides difficile (C diff).
Key points:
Fidaxomicin targets C diff with limited collateral microbiome disruption. This leads to significantly lower recurrence rates compared to vancomycin. Thus, it is preferred 1st line therapy for initial and recurrent C diff. In “the coming years, fidaxomicin is expected to come off patents” which will improve access and affordability.
Bexlotoxumab which lowered recurrence rate is no longer being produced
FMT via Openbiome is no longer available. In those in which FMT was used, options include the following:
live-jslm (REBYOTA), a broad consortium enema-based formulation
live-brpk (VOWST), a narrow consortium of Firmicutes in an encapsulated form. This treatment in adults: four capsules daily for three days
Both treatments are not recommended for patients who are severely immunocompromised. In these patients, prolonged vancomycin course with taper or using every other day therapy with fidaxomicin for days 7-25 could be considered
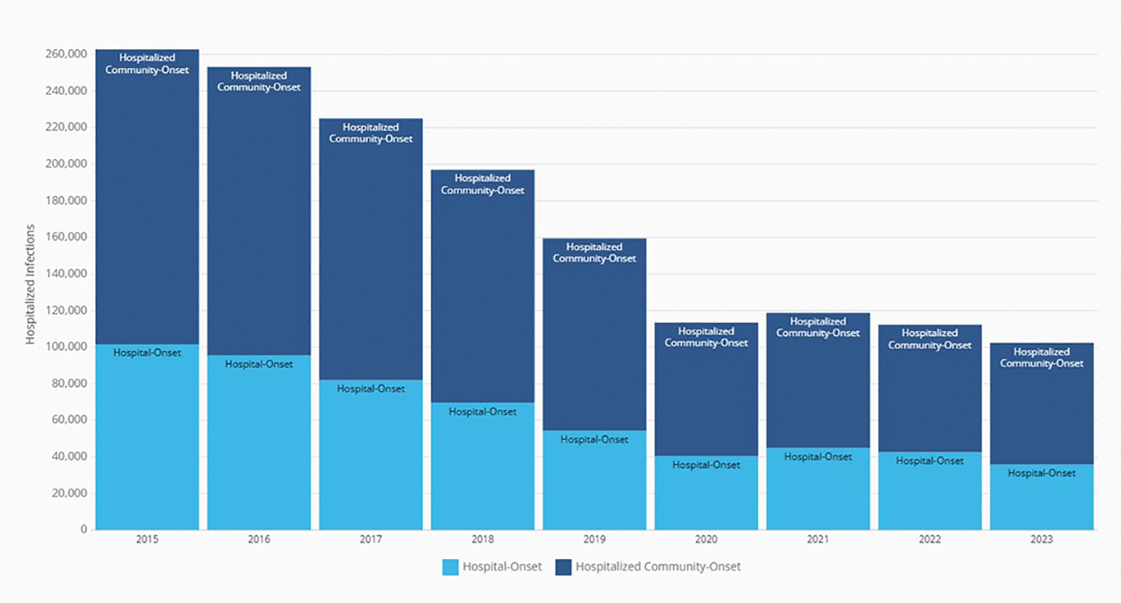
My take: I have been seeing less C diff cases recently. This may be due to better antibiotic stewardship, changes in C diff strains, or improved testing approaches.. My observation is supported by recent reports:
Annual number of hospitalized community-onset and hospital-onset CDI events reported to the National Healthcare Safety Network, 2015 to 2023. (From CDC’s Antibiotic Resistance & Patient Safety Portal (Available at https://arpsp.cdc.gov/profile/nhsn/cdi).)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
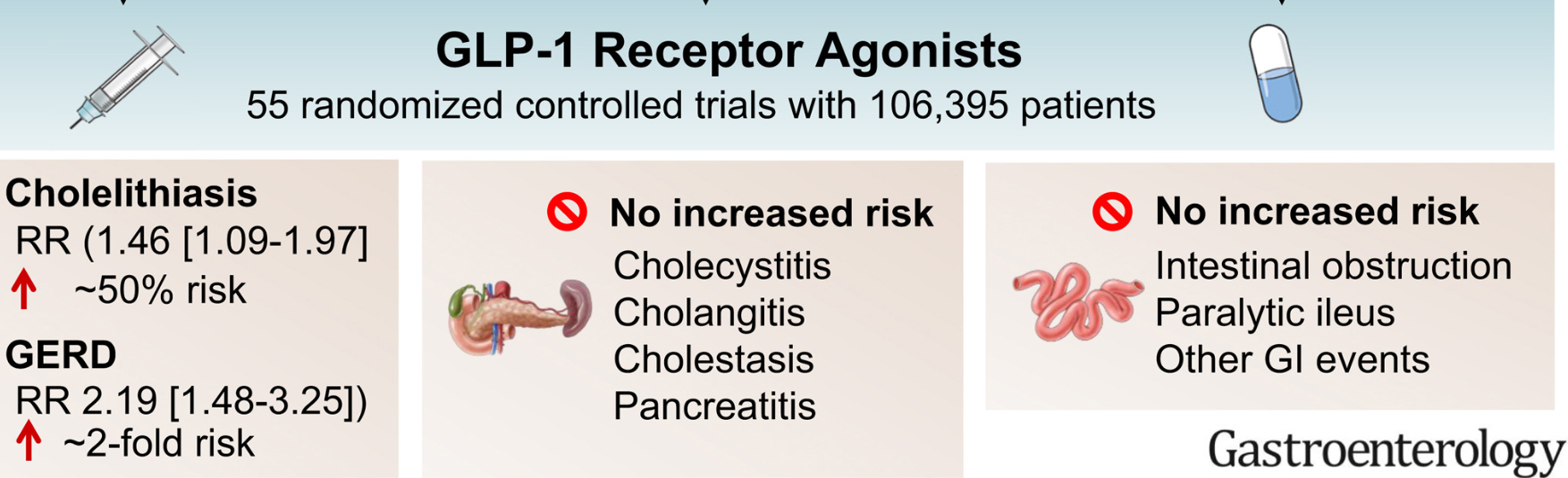
With the widespread adoption of GLP-1 RAs, there have been increasing reports of adverse effects. This systematic review/meta-analysis (with 55 randomized controlled trials involving 106,395 participants) more fully describes the likelihood of GI adverse events.
Key findings:
GLP-1RAs increased the risk of cholelithiasis (risk ratio [RR], 1.46; 95% CI, 1.09–1.97; 2 more cases per 1000) and probably increased the risk of GERD (RR, 2.19; 95% CI, 1.48–3.25; 4 more cases per 1000) compared with placebo
GLP-1RAs probably have little or no effect on the risk of other gastrointestinal or biliary events
Figures 2 & 3 use a Forest plot to look at a large number of potential adverse gastrointestinal/biliary events. For example, cholecystitis and cholangitis had increased RR at 1.17 and 1.54 respectively. However neither reached statistical significance.
My take: GLP-1 RAs definitely cause adverse gastrointestinal effects, especially nausea, vomiting, diarrhea, bloating and reduced appetite. More severe adverse effects are quite uncommon and are unlikely to influence the decision to use these medications.
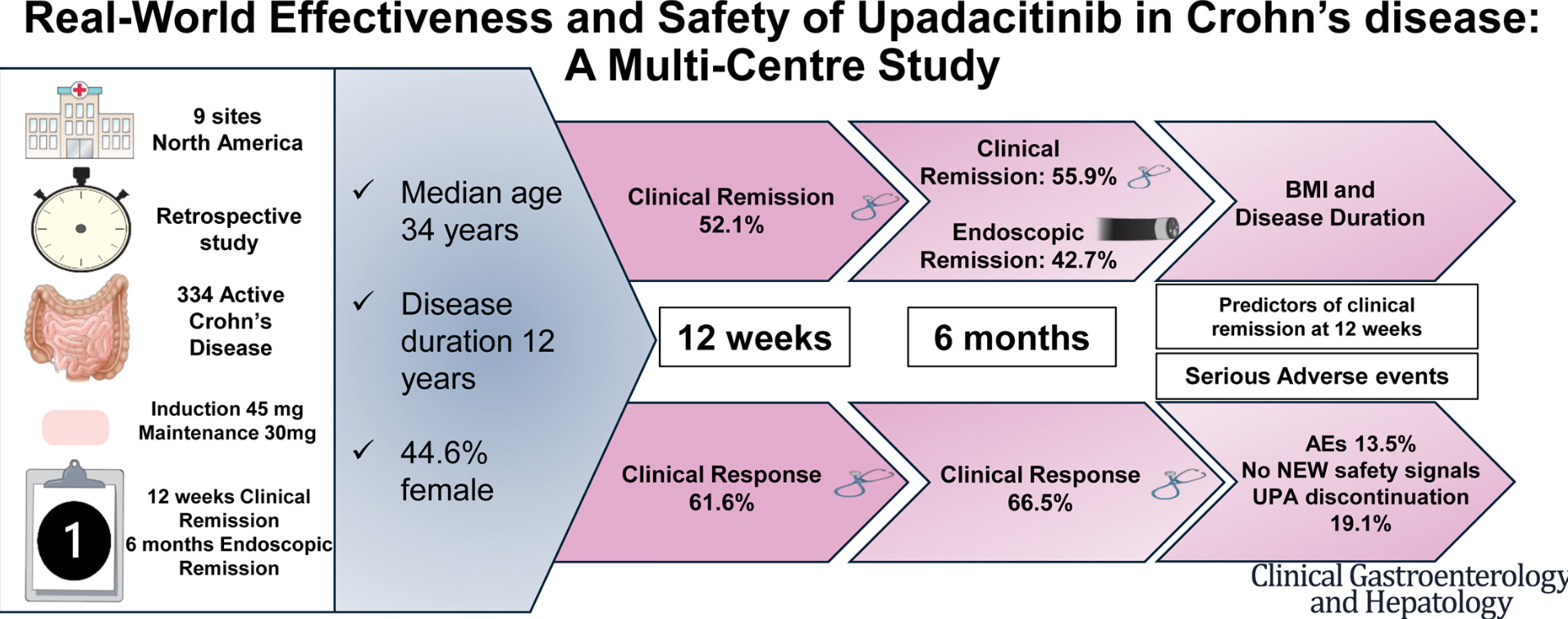
This was a multicenter, retrospective, case-control study of patients hospitalized with ASUC who underwent colectomy, comparing patients treated with tofacitinib (n=41) prior to colectomy with infliximab-treated controls (n=68).
Key findings:
Compared with tofacitinib-treated patients, infliximab-treated patients had higher overall rates of overall (44 [64.7%] vs 13 [31.7%]; P = .002) and serious (19 [27.9%] vs 3 [12%]; P = .019) postoperative complications
My take: This study supports the safety of JAK inhibitor therapy for ASUC. It showed a significantly lower rate of overall postoperative complications in ASUC patients treated with tofacitinib compared with infliximab; the authors note that “these findings can likely be extrapolated to upadacitinib, a selective JAK inhibitor, given its similar mechanism of action.”
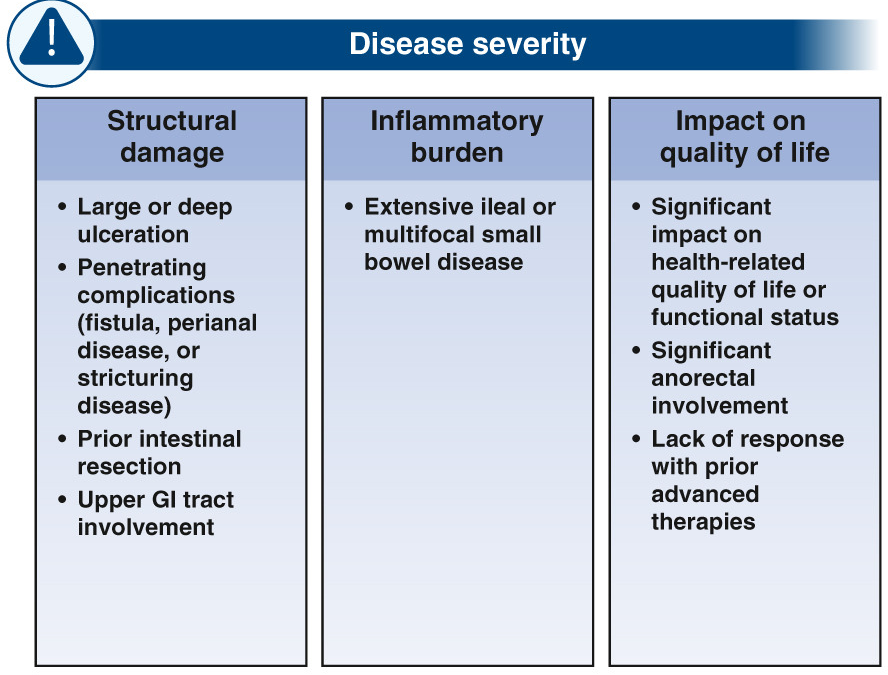
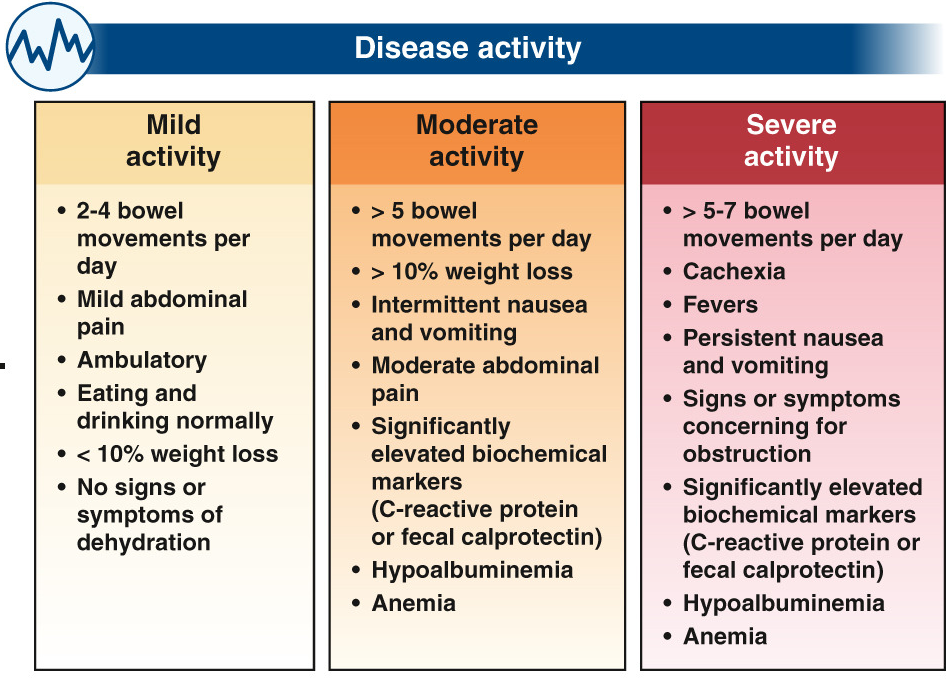
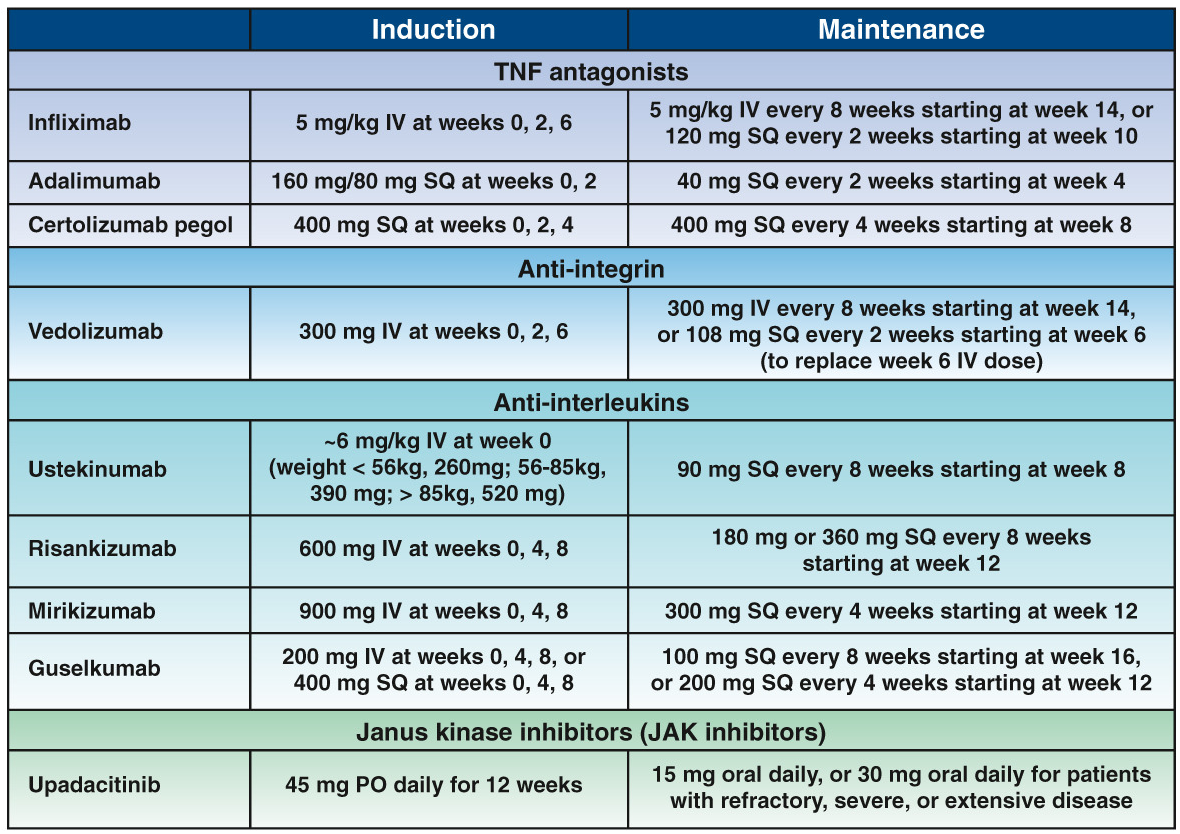
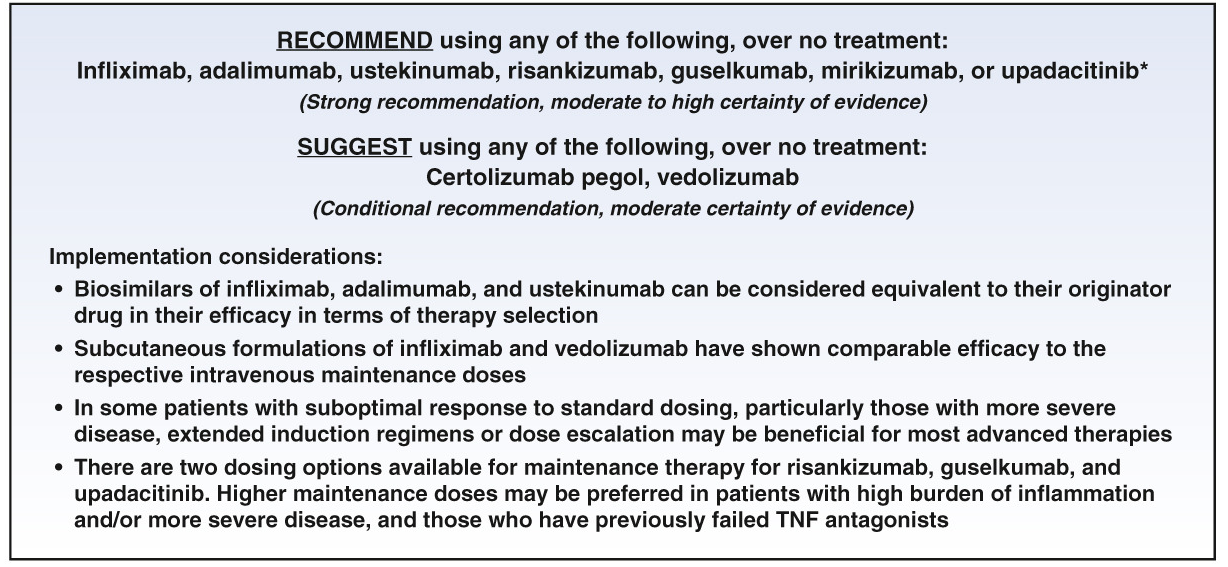
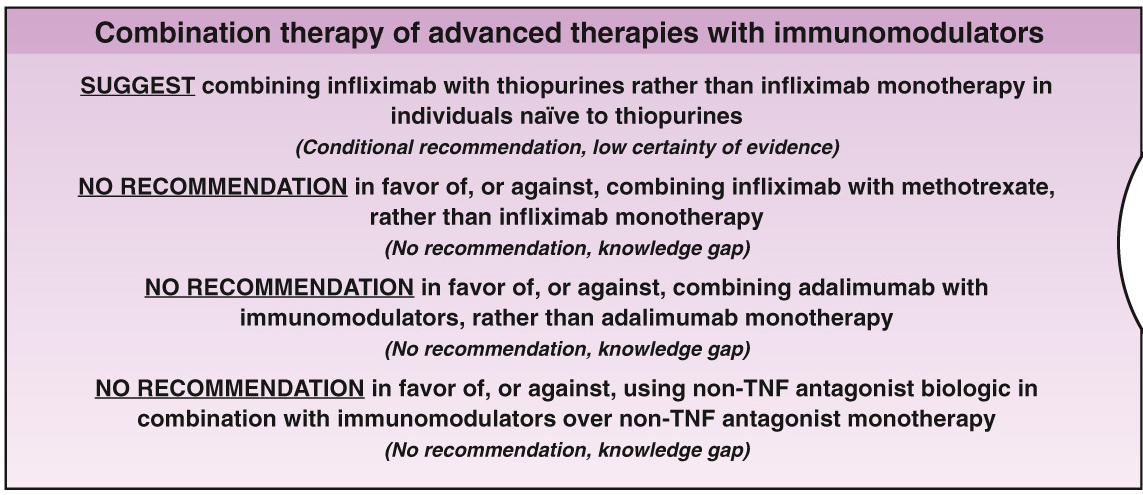
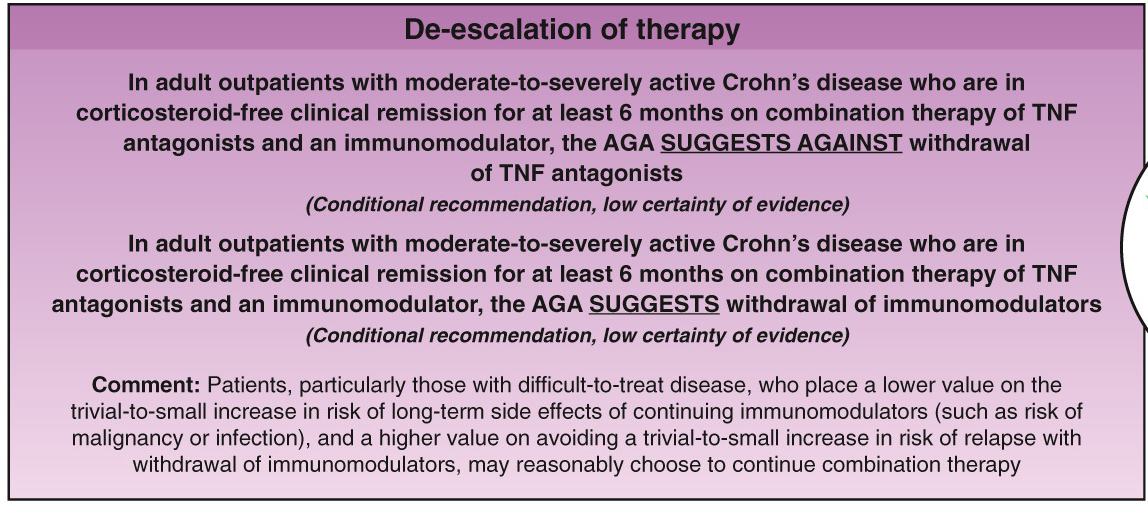
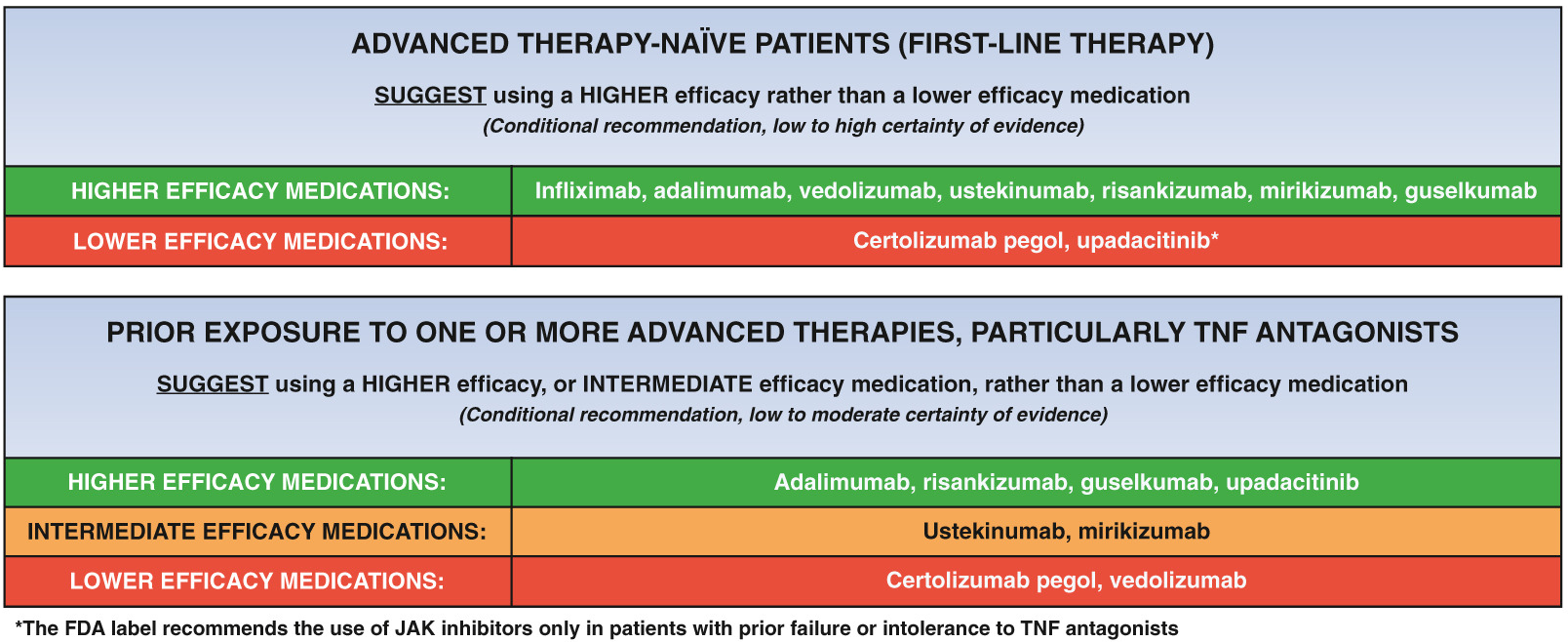
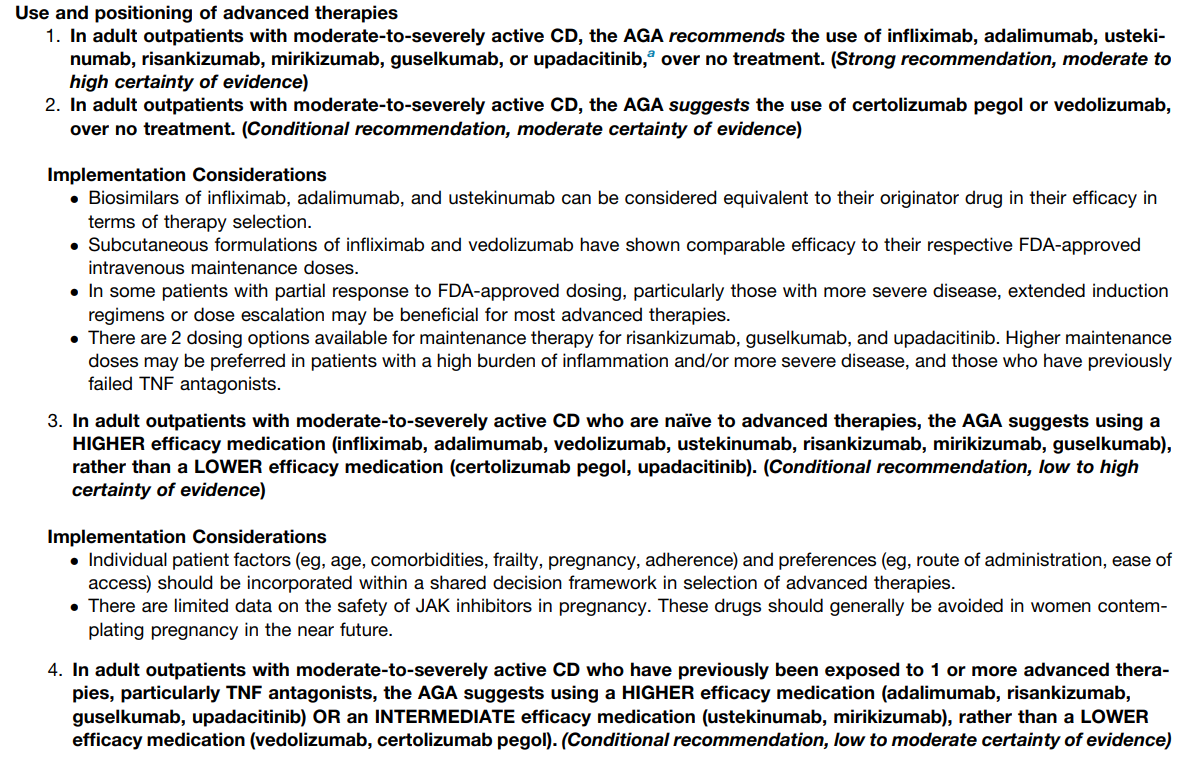
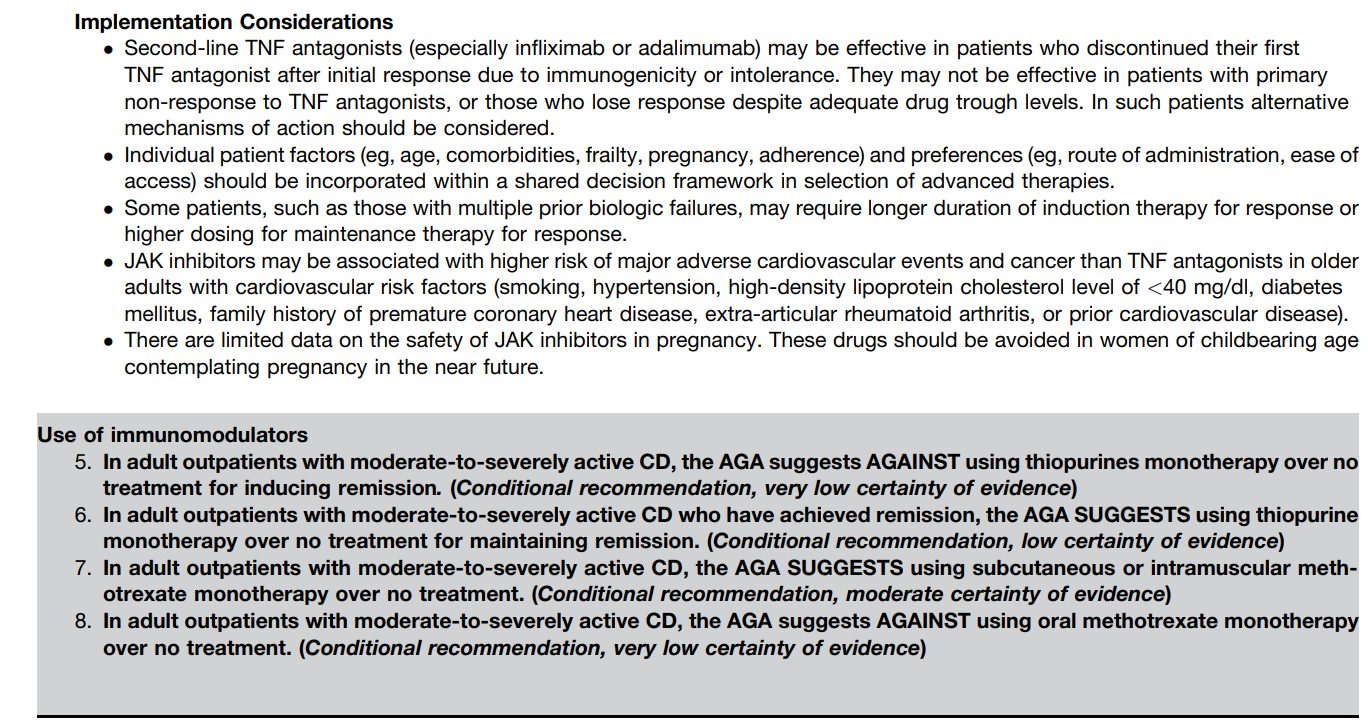
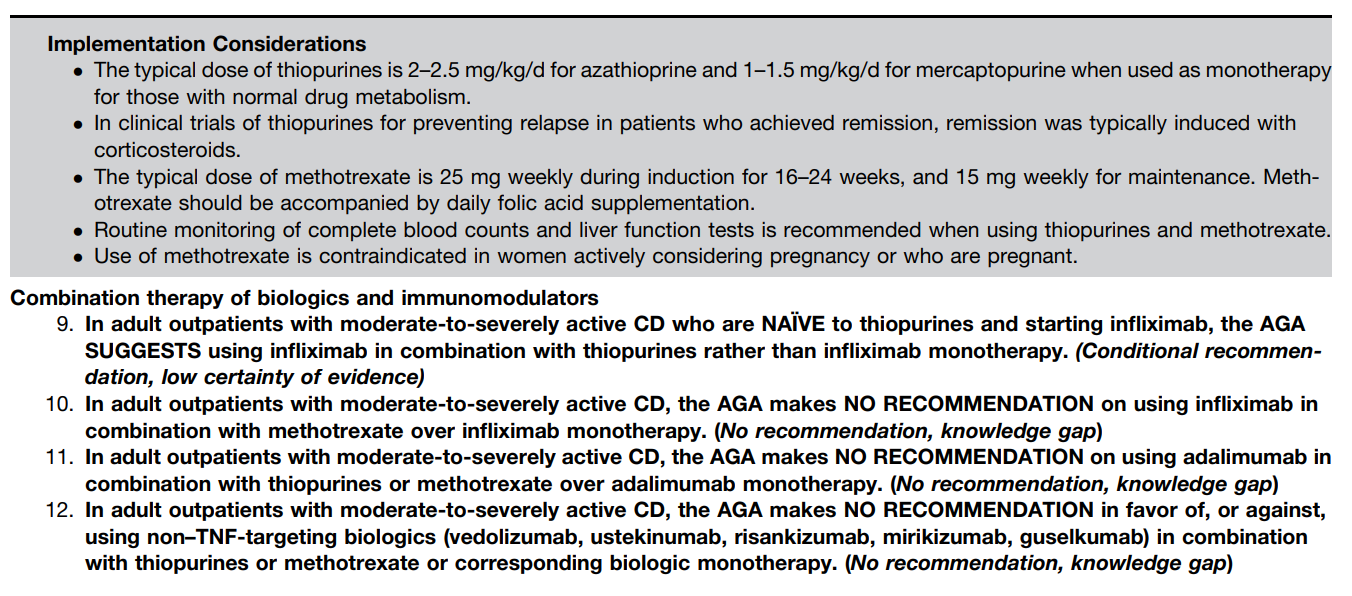
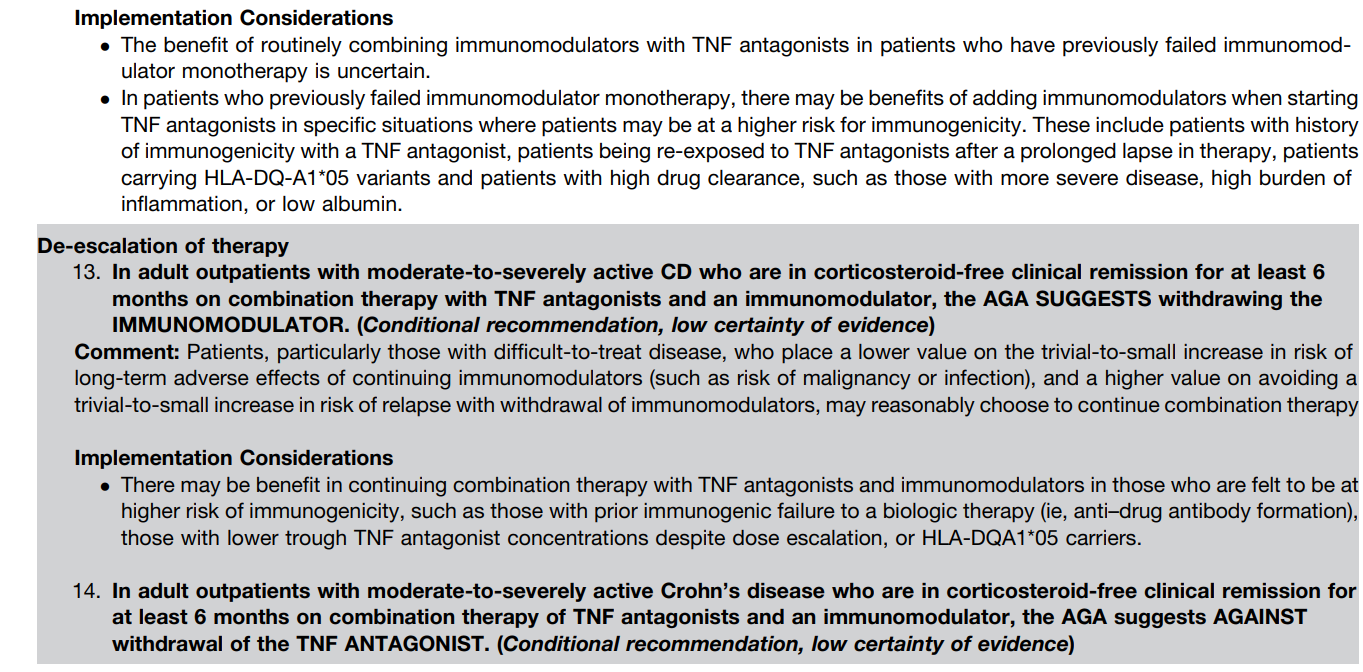
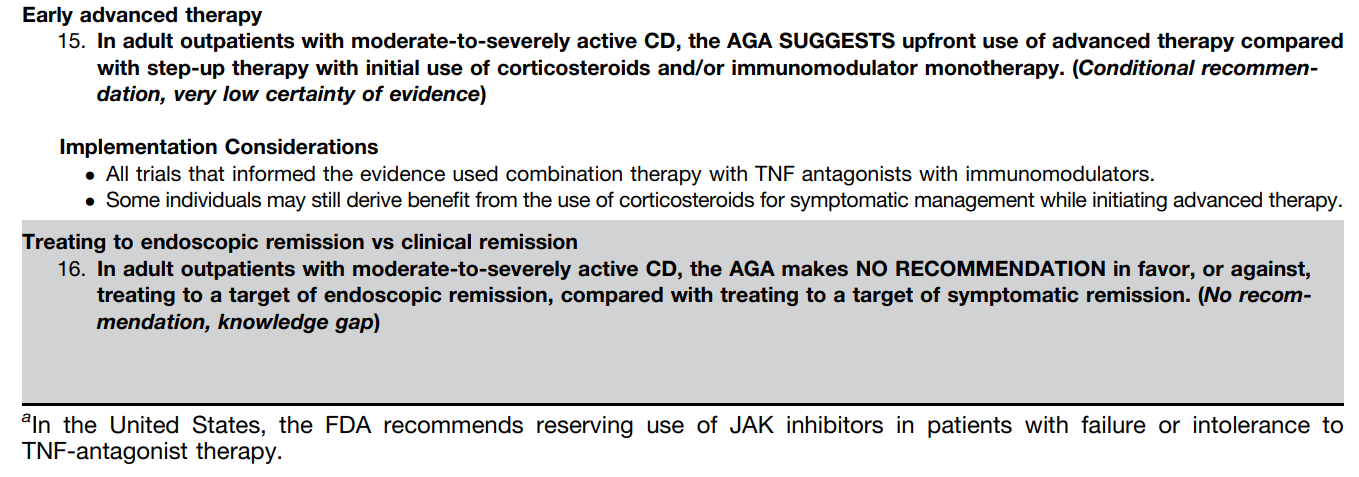
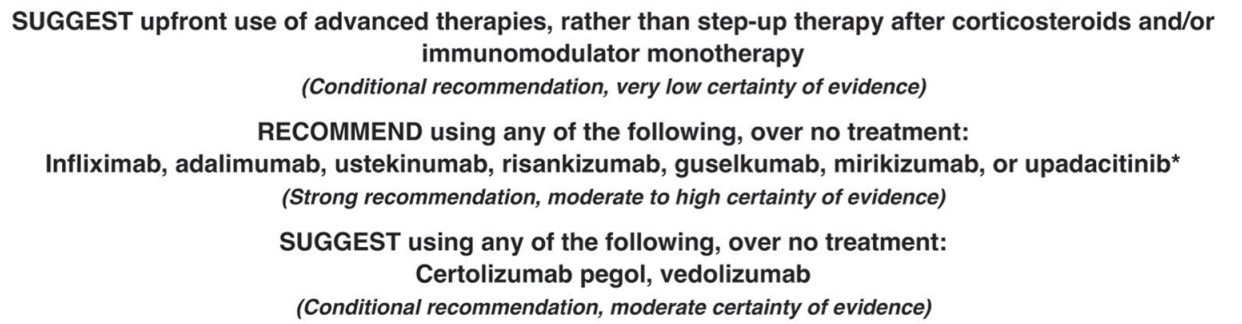
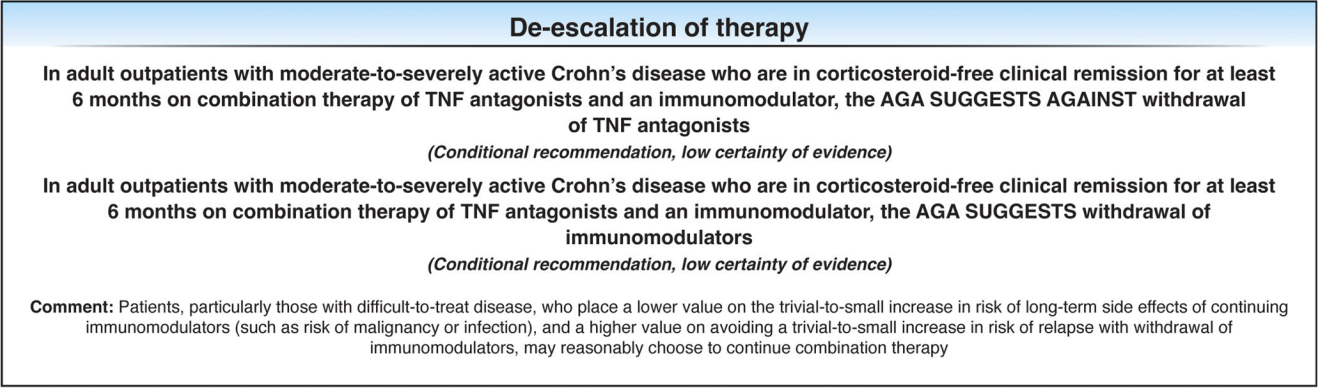
The guideline panel agreed on 16 recommendations. This highly-detailed report provides a comprehensive, patient-centered, evidence-based approach to the pharmacologic management of adult patients with moderate-to-severely active CD. Table 1 summarizes this lengthy 53-page report. Tomorrow’s post will be the “spotlight” summary which presents the recommendations in easier to read graphic.
Key Points:
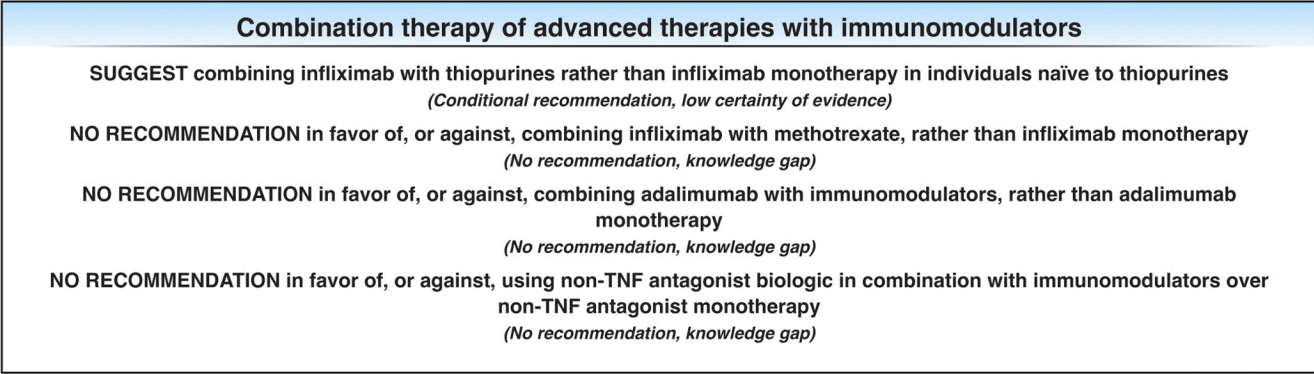
The guidelines are overall very helpful. They identify higher efficacy medications and recommend them. In addition, they support the use of combination therapy with thiopurines (which are less frequently used in pediatrics). It is interesting that the sixteenth recommendation clashes with prior expert recommendations. The sixteenth recommendation in this report makes no recommendation on using endoscopic surveillance compared to symptomatic clinical remission. Most experts advise “treat-to-target” therapy approaches.
In the discussion of this, the authors state the followiing:
“Recent position statements from an international consortium of experts have advised that longitudinal targets for the management of IBD should include not only clinical remission but also endoscopic resolution of inflammation.31 Several studies have demonstrated that patients who achieve endoscopic remission (vs those with ongoing endoscopic activity) have favorable long-term outcomes…
There are limited RCTs assessing whether there is actual benefit in systematically treating toward endoscopic remission target vs symptomatic remission targets (ie, testing whether the target has been achieved, followed by algorithmic treatment adjustment, including escalating index therapy, adding an immunomodulator, followed by switching to an alternative advanced therapy and surgery). There was significant heterogeneity among the 2 reviewed studies, both in terms of the advanced therapy used, algorithms for therapy modification, and the cadence and frequency of endoscopic monitoring that challenge interpretation. Based on the significant uncertainty of evidence with regard to improving maintenance of remission or reducing the risks of adverse events, the guideline panel could not make a recommendation in relation to selecting endoscopic targets over clinical targets.
It is worth emphasizing that in both of the included trials, the majority of individuals in the endoscopic healing arms were not able to meet the goal of endoscopic healing despite an algorithmic approach. For example, in STARDUST, only 11% of individuals achieved endoscopic remission.149…There are specific patient populations, such as those who have recently undergone intestinal resection,155 in which endoscopic evaluation may be particularly valuable in clinical decision making...
The benefit of a monitoring strategy incorporating biochemical monitoring over clinical monitoring alone was demonstrated in the CALM trial,152 and has been addressed in previous AGA guidelines on the role of biomarkers in patients with CD.12“
My take: These “living” guidelines are likely to be quite influential in selecting Crohn’s disease therapy. In pediatrics, ImproveCareNow provides a similar role of guiding treatment.





06160-8/asset/17e8b821-1efa-4c66-adce-db270f9e7629/main.assets/fx1_lrg.jpg){kind=link}