




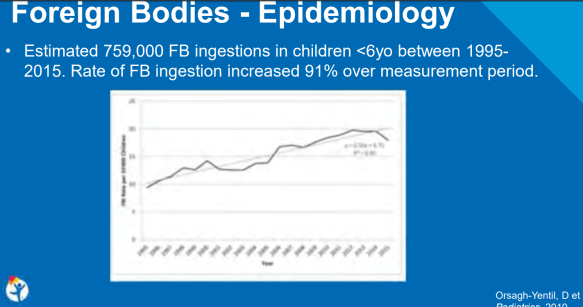
A recent retrospective study (D Orsagh-Yentis) Pediatrics 2019; 143: pii:320181988) examined children <6 years of age (n=759,054) and presentation to an emergency department in the U.S. for a foreign body ingestion (FBI) from 1995-2015. This study was reviewed at our recent national meeting by David Brumbaugh -related blog post: #NASPGHAN19 Postgraduate Course (Part 1) (Slides below).
Key findings:
Related blog posts:

A recent analysis (MG Warren et al J Pediatr 2019; 214: 41-6) examined gastrostomy tube (GT) placement among 4569 extremely low birthweight (ELBW) infants (birth wt <1000 gm) who were enrolled in the National Instittue of Child Health and Human Development Neonatal Research Network (25 centers).
Key findings:
In the discussion, the authors note the well-recognized associations between feeding difficulties and language delays in ELBW infants. In addition, “behavioral and emotional problems have …been described in children with feeding problems.”
The authors also state, without evidence, that the high rate of GT placement after discharge suggests that “a large proportion of ELBW infants were first discharged from the NICU orally feeding but could not maintain these skills.” Alternative explanations include the following:
My take: This study indicates that 7% of ELBW infants undergo GT placement and that about one-third out-grow the need for GT supplementation after ~2 years.
Related blog posts:

Quebec City
A recent retrospective study (N Nguyen et al. Clin Gastroenterol Hepatol 2019; 17: 2455-2462) describe the feasibility of unsedated transnasal endoscopy (TNE) for monitoring eosinophilic esophagitis (EoE) in children (n=190, subject ages 3-22 years).
TNE was facilitated by distraction with either video google or virtual reality (starting 2016). NPO time was 2 hours before the TNE.
Key points:
The authors recommend that TNE be offered starting at age 5 years in those without a known stricture.
My take: I am looking forward to less invasive/less costly ways of monitoring treatment response in EoE. I think TNE can lower costs –though I am a little surprised that the cost of TNE in their institution was still more than $4000. In our outpatient endoscopy center, costs for an upper endoscopy/biopsy with anesthesia are typically about one-third the cost of an EGD in their study and about three-fourths the cost of a study TNE.
Related study: A Krigel et al. Clin Gastroenterol Hepatol 2019; 17: 2489-96. This study showed increasing use of anesthesia assistance (AA) for colonoscopy in adults from 16.7% in 2006 to 58.1% in 2015. This data was derived from the Premier Perspective database with more than 4.6 million patients who had an outpatient colonoscopy. AA was associated with a median increase in cost of $182 for patients with commercial insurance.
Related blog post: Waiting for the String Test for EoE

“80 percent of success is just showing up” —Woody Allen
Reading a recent (brief) study (BA Blansky et al. Clin Gastroenterol Hepatol 2019; 17: 2503-4) reminded me of the quote from Woody Allen. This study of children with Celiac disease (CD) demonstrates a high rate of children who were lost to follow-up at a leading Children’s hospital.
Key findings:
My take: These numbers should not be surprising to most clinicians. If clinicians want to improve follow-up and outcomes, then families will need more nudging; EMRs can be configured to help in this task.
Related blog posts:

Quebec City
SR Gupta et al. JPGN 2019; 69: 544-50. This article reports on preliminary experience in 54 children who received external (non-hospital) infliximab infusions. The average age was 17.6 years. The authors noted no serious safety concerns. Prior to arranging these infusions, the authors insisted on the following:
BN Limketkai et al. Inflamm Bowel Dis 2019; 25: 1828-37. This study, using Truven Health MarketScan database (2007-16) reviewed proactive or reactive mucosal monitoring after biologic initiation in IBD. Early (< 6 months) proactive monitoring (88% endoscopy-based) was performed in 11% (n=2195/19,899) of patients with Crohn’s and 12.8% (925/7247) of patients with ulcerative colitis.
RZ Cohen, BT Schoen, S Kugathasan, CG Sauer. JPGN 2019; 69: 551-6. In this chart review, the authors identified anti-drug antibodies (ADA) in 24.8% (n=58) of patients undergoing therapeutic drug monitoring (n=234) with both infliximab and adalimumab. 54% of this group had antibody suppression with dose optimization. Of note, 37 patients had detectable ADA at time of initial drug monitoring. Dose optimization was 10 mg/kg every 4 weeks with infliximab or 40 mg weekly with adalimumab. Patients who were switched to a second anti-TNF agent (n=23) were not more likely to develop ADA to the second agent (small sample size). Also, the authors caution that in the five patients with ADA levels (>10 U/mL), dose optimization failed and patients required a therapeutic switch. My take: This study provides some useful information about the frequency of ADA. My view is that the actual drug level is more critical than the presence of ADA; though, the presence of high ADA often precludes the ability to deliver a therapeutic drug level.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
About two years ago, James Franciosi presented research at NASPGHAN meeting indicating that the main difference between children with eosiniophilic esophagitis (EoE) who respond to proton pump inhibitiors (PPIs) compared to those who do not was related to their metabolism of PPIs and not related to the nature of their underlying EoE.
Related blog: #NASPGHAN17 Eosionophilic Esophagitis Session
Now, more has been published on this topic: EB Mougey et al. JPGN 2019; 69: 581-7.
In this study with 92 patients, data was collected from participants in a prospective clinical trial of high-dose PPI for EoE.
Key findings:
Discussion:
My take: This study indicates that genotype-guided dosing of PPIs for the treatment of EoE is likely to be worthwhile.

View from Yonah Mountain, GA
A recent retrospective study (FWT Vergouwe et al. JPGN 2019; 69: 515-22) with 57 children with esophageal atresia (EA) found most children have a normal reflux index.
This study, analyzing data between 2012-2017, reviewed all 24-hour pH-impedance (MII) studies in children at ≤18 months and 8 year olds with EA. “All children with EA born in our hospital are offered a 24-hour pH-MII study at the age of 0.5 years and 8 years.” In this institution, PPI treatment is given for at least 6 months after surgery. Of the 57 in the cohort, 20 had completed pH-MII at <18 months of age and 32 at age 8 years.
Key findings:
My take: This study showed that reflux in this cohort of children with EA was similar to the general population and likely indicates that a substantial portion of patients with EA do not need indefinite PPI therapy. In children with more complex EA, PPI therapy is likely to be more beneficial.
Related blog posts:
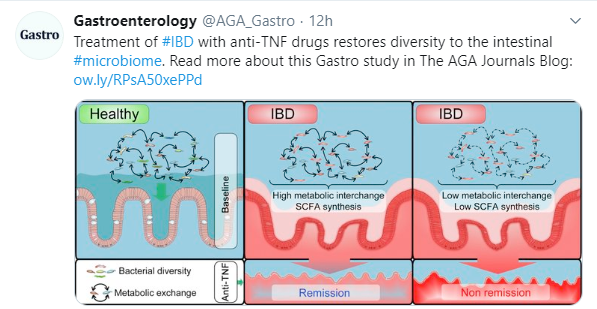
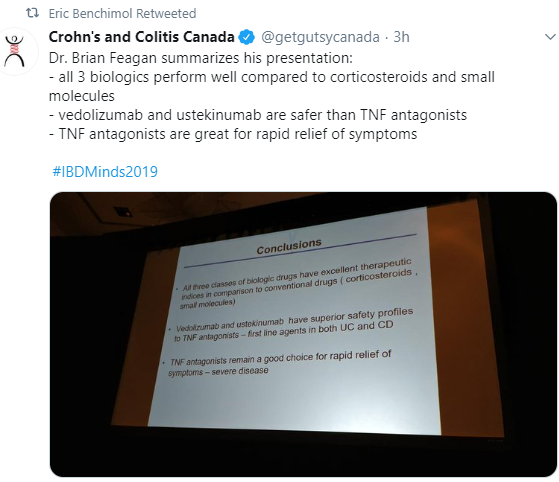
Recent (November 4th) GI-Related Tweets:

Briefly noted: MD Bellin et al. JPGN 2019; 69: 599-606.
Using the INSPPIRE database with 397 children with either acute recurrent pancreatitis or chronic pancreatitis, the authors examined the frequency of diabetes mellitus (DM).
Key findings:
Related blog posts:

Frontenac Hotel, Quebec City
Previously, it has been recognized that increased rates of necrotizing enterocolitis (NEC) have been associated with viral outbreaks (eg. rotavirus, norovirus) (J Pediatr Surg. 2004;39:453–7 ,Pediatr Infect Dis J. 2010l;29: 644-7.).
A more recent study (S Panesso-Gomez et al. J Pediatr 2019; 214: 34-40) examines the association between cytomegalovirus (CMV) and NEC.
Key Findings:
One of the limitations of the study was the lack of a control group, though previous reports have found congenital CMV in 0.4% of preterm infants with very low birth weight (<1500 g) and in 0.5-1% of all liver births.
My take: This study shows an association between the presence of CMV and NEC; hence, CMV may be one of many factors which increase susceptibility to NEC.
Related blog posts:

Yonah Mountain
