Recent studies point to huge advances in cystic fibrosis (CF) therapy. Though as noted in a previous blog (Why Do Canadians with Cystic Fibrosis Live Longer?), medical advances may have limited effect based on a lot of issues including access to care.
Despite that note of caution, it is hard not to be excited about a couple of recent publications which show that triple cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapy has great potential to improve outcomes for CF patients.
- JC Davies et al. NEJM 2018; 379: 1599-611.
- D Keating et al. NEJM 2018; 379: 1612-20.
- Editorial: F Holguin, 1671-2
Background: In the editorial, the pathophysiology of the defect of CF is discussed and how the newer medicines either act as a potentiator of the CFTR (ivacaftor) or as corrector (lumacaftor and tezacaftor). Potentiators increase CFTR channel opening at the cell surface whereas correctors increase the amount of CFTR protein at the cell surface. One caveat has been that these therapies had not been proven effective, individually, for Phe508del CFTR mutation which occurs in “approximately two thirds of patients.” Combination therapy has helped in most of this group but not in those with Phe508del-minimal function (MF).
The new studies examine triple therapy with the addition of two new-generation small molecule correctors: VX-445 and VX-659. These new correctors target different sites of the CFTR protein.
Key findings:
- in the Davies (VX-659) trial, “4 weeks of triple therapy …increased the primary end point of predicted percentage of FEV1, in the Phe508del-MF and Phe508del-Phe508del groups by an averae of 13.3% and 9.7% respectively”
- In the Keating (VX-445) trial, triple therapy “significantly increased FEV1 in patients with those genotypes by 13.8% and 11.0% respectively.”
- Overall, triple therapy “improved the percentage of predicted FEV1 more than double-combination therapy” in patients with a Phe508del-Phe508del mutation. And reported efficacy in the patients with Phe508del-MF CFTR mutation.
- The majority of patients had at least one adverse event. 3 of the 122 in the VX-445 trial discontinue treatment due to severe adverse events.
My take: These reports “represent a major breakthrough…for improving health and possibly survival in all patients who carry the most common CFTR mutation.” Long-term outcomes will need to be followed to confirm these findings.
Related blog posts:
- Lumacaftor-Ivacaftor for Cystic Fibrosis
- Ivacaftor for Cystic Fibrosis | gutsandgrowth
- CFTR Modulators for Cystic Fibrosis
- FDA Expands Use of Cystic Fibrosis Medication | gutsandgrowth
- “Origins of Cystic Fibrosis Lung Disease”
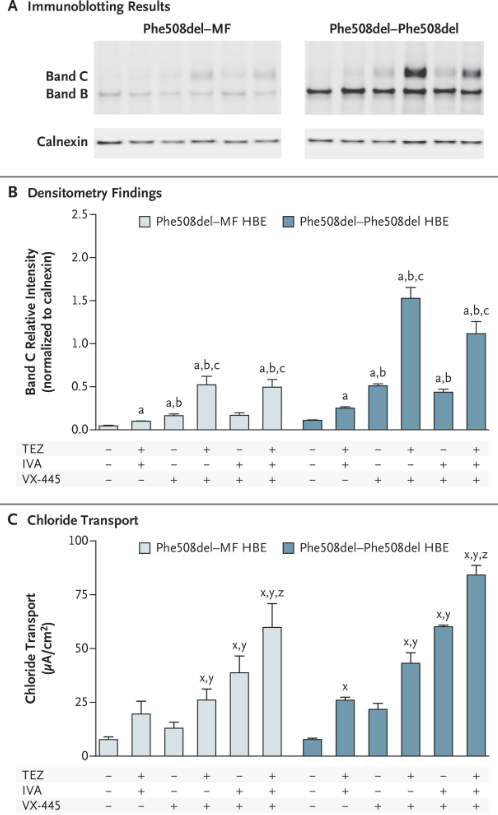
This is Figure 2 from Davies study showing immunoblot findings, densitometry findings, and chloride transport in bronchial cells. The most robust responses were with triple therapy