N Norris et al. J Pediatr 2025; 276: 114329. Liberal Fluid Resuscitation is Associated with Improved Outcomes in Pediatric Acute Pancreatitis
This single-center retrospective study with 227 patients (2013-2023) examined the role of liberal fluid administration/type of fluid administration and outcomes in children with acute pancreatitis. Overall, 100 patients received normal saline (NS) and 41 received lactated ringers (LR). Liberal fluid management was considered to be >1.5x the maintenance.
Key findings:
- Patients who received liberal fluids were less likely to be admitted or transferred to the intensive care unit compared with those receiving conservative management (OR, 0.32)
- The liberal NS fluid group with early feeding had the lower rates of moderate/severe manifestations of AP compared with other combinations of diet and fluid orders except the conservative LR group
- Moderate/severe AP was highest in the conservative NS group (14/37 [38%]), followed by liberal LR (6/31 [19%]), liberal NS (9/63 [14%]); it was lowest in conservative LR group (0/10 [0%]).
In the discussion, the authors note that adult studies have supported a more moderate approach to IVFs (1.5 mL/kg/hr) given the risks of fluid overload in WATERFALL trial.
My take:
- It is surprising that so few patients received LR in this study; there has been some evidence that LR is better than NS for AP since 2014 (see blog posts below)
- Especially in those receiving NS, more liberal use of IVFs appears beneficial. Reasonable to start at 1.5 x maintenance (as recommended by Dr. Freeman)
- Though children generally tolerate liberal IVFs better than adults due to better cardiovascular function, a prospective randomized study is needed to determine which fluid strategy is optimal.
- Early enteral feeding is beneficial in most cases

Related blog posts:
- Why an ERCP Study Matters to Pediatric Care (2014)
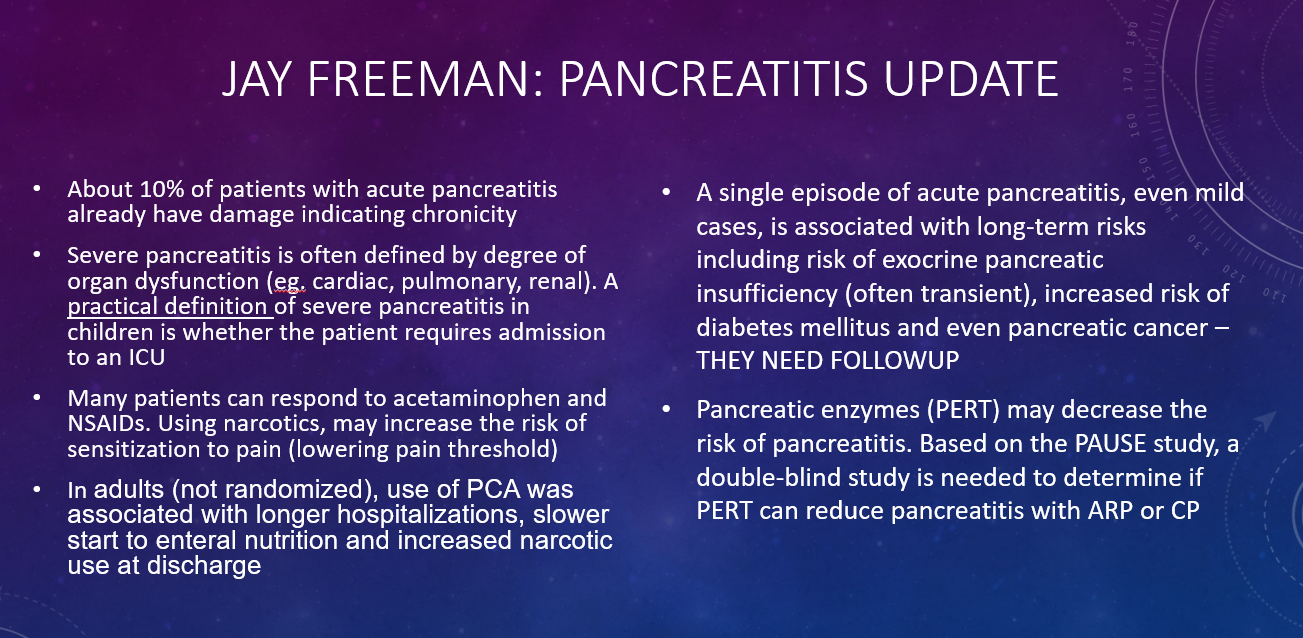
- How to Upgrade Pancreas Care –Jay Freeman MD (Part 2) (2024)
- How to Upgrade Pancreas Care –Jay Freeman MD (Part 1) (2024)
- Common Mistakes When Managing Acute Pancreatitis (2024)
- Acute Pancreatitis Review (2016)
- Acute Pancreatitis: Clinical Report from NASPGHAN (2018)
- More Data Supporting Lactated Ringers for Acute Pancreatitis (2021)
- Pediatric Pancreatitis -Working Group Nutritional Recommendations (2018)
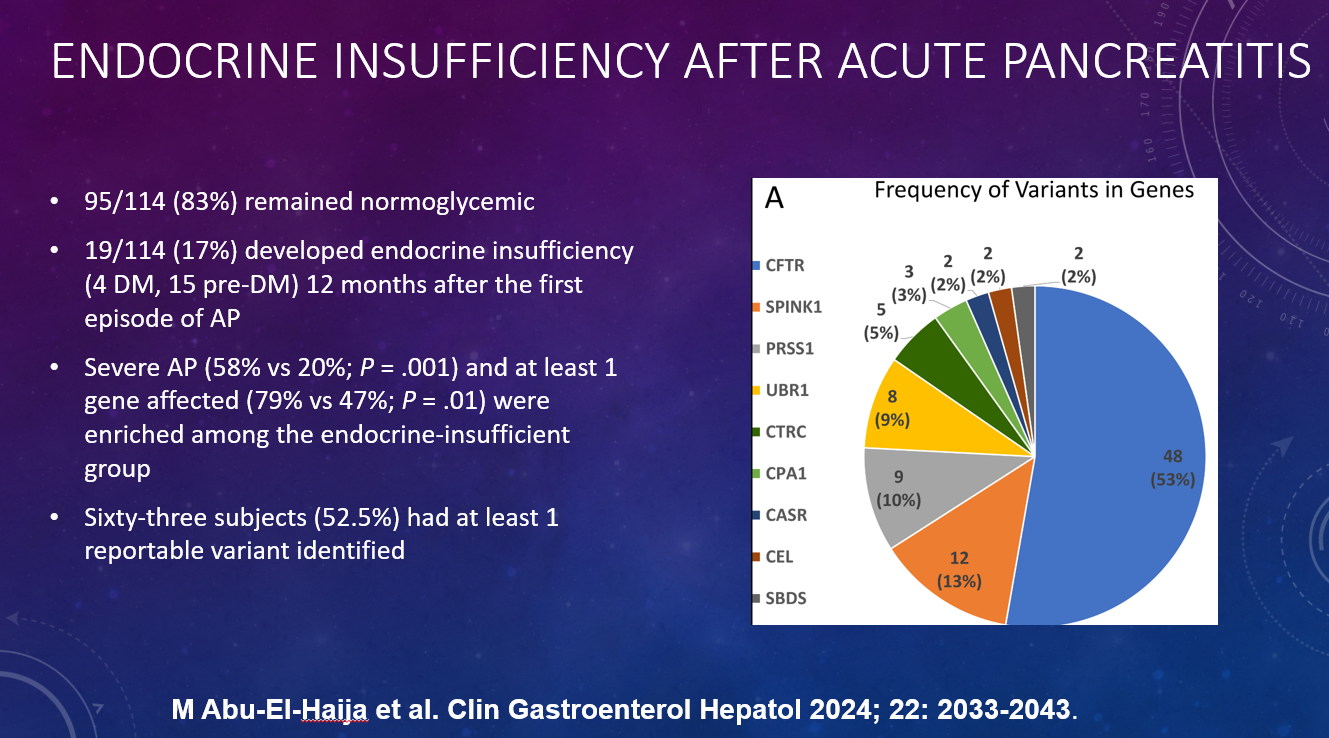
- Here’s the Data: Endocrine Insufficiency After Acute Pancreatitis in Children (2024)
- #NASPGHAN18 Abstract: LR for Pancreatitis & Pumpkin Shot (2018)