S Harpavat et al. Pediatrics Pediatrics (2025) 155 (3): e2024070077. (Open Access!) Guidance for the Primary Care Provider in Identifying Infants With Biliary Atresia by 2–4 Weeks of Life: Clinical Report
Recommended Screening:
- Office visit at 2-4 weeks of age (by 4 weeks of life)
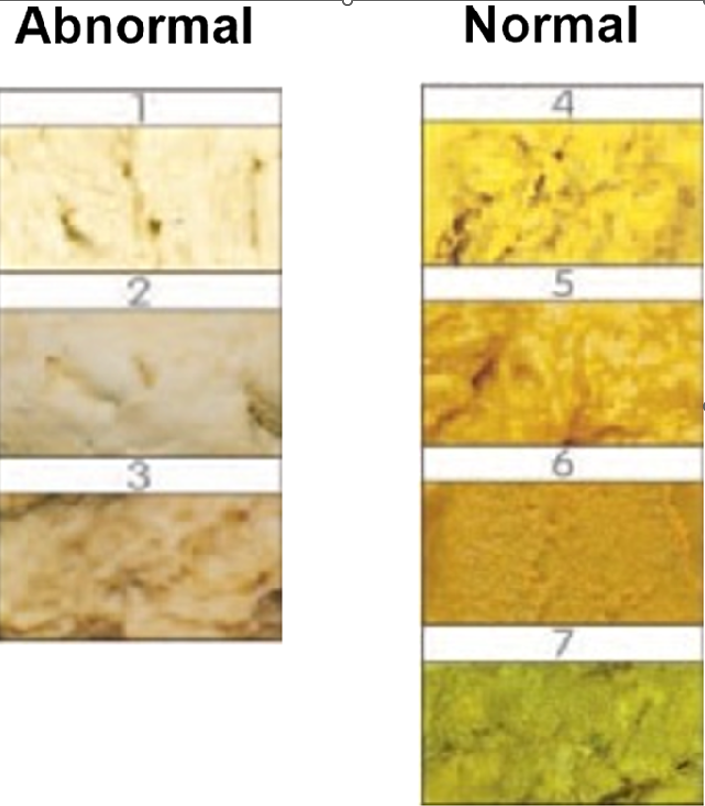
- Check fractionated bilirubin: If there is any pale, gray or white stools, If there is any jaundice in eyes or skin, or If there is a prior history of abnormal direct or conjugated bilirubin*
- If direct or conjugated bilirubin is 1 mg/dL or higher, urgent consult to GI

“The most important result is the initial direct or conjugated bilirubin level, which will be “high” in BA starting at birth.11,17,18 “High” is defined as exceeding the laboratory’s derived reference range, even if only by 0.1 mg/dL In the period before 2 weeks of life, “high” is not defined by exceeding a fixed cut-off or exceeding a bilirubin ratio.”
Additional Recommendations:
- The authors indicate that followup blood testing is NOT needed if the following: 1. Any prior direct or conjugated bilirubin level that was normal (in reference range) or 2. Prior direct or conjugated bilirubin levels that were all abnormal but equivalent or decreasing over time. In this instance, equivalent or decreasing is defined as both (i) less than or equal to the initial level; and (ii) <1 mg/dL
- “Consider adding direct or conjugated bilirubin testing when serum total bilirubin testing is performed. As mentioned earlier, many centers measure at least 1 serum total bilirubin level via heel stick or venipuncture to assess risk for bilirubin encephalopathy. Direct or conjugated bilirubin levels can be measured from the same heel stick or venipuncture sample, without needing an additional blood draw.”
My take: Any child with an elevated direct or conjugated bilirubin (above reference range) in the first two weeks of life needs to be carefully followed. This guideline also recommends using abnormal stool color and prolonged jaundice/icterus as prompting bloodwork.
In the past, it was consider normal in newborns to have elevated direct bilirubin IF there was a low ratio of direct bilirubin to total bilirubin (less than 20% in those with bilirubin >5 mg/dL). However, this can result in missed cases of biliary atresia.
Related blog posts:
- Landmark Study on Universal Screening for Biliary Atresia -It Works!
- Online Aspen Webinar (Part 5) -Biliary Atresia Diagnosis and Screening (2020)
- MMP-7 Helps Sort Out Biliary Atresia from Parenteral Nutrition-Associated Liver Disease
- Don’t Put the Cart Before the Horse: Biliary Atresia Screening
- Updated Diagnostic Accuracy of Serum Matrix Metalloproteinase-7 (MMP-7) for Biliary Atresia
- Dried Blood Spot Testing for Biliary Atresia
- How Often Is Surgical Treatment for Biliary Atresia Delayed Beyond 60 Days?