NPR 3/25/23: ‘Live free and die’? The sad state of U.S. life expectancy
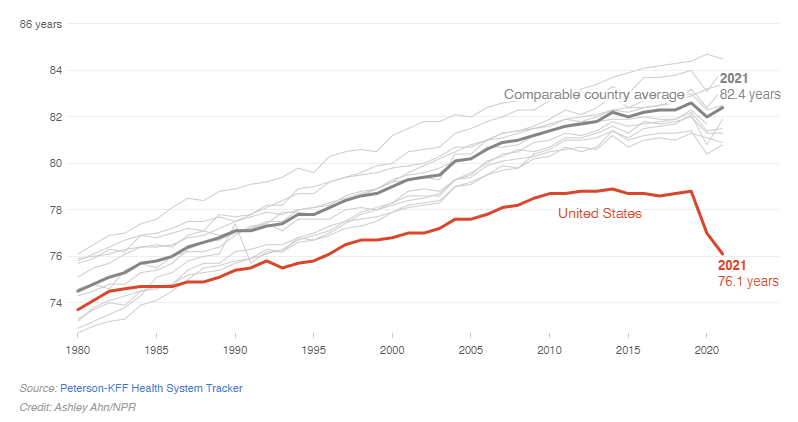
Most peer countries rebounded by 2021, while the U.S. continued to decline.
An excerpt:
- Just before Christmas, federal health officials confirmed life expectancy in America had dropped for a nearly unprecedented second year in a row – down to 76 years. While countries all over the world saw life expectancy rebound during the second year of the pandemic after the arrival of vaccines, the U.S. did not….American life expectancy is lower than that of Cuba, Lebanon, and Czechia.
- Then, last week, more bad news: Maternal mortality in the U.S. reached a high in 2021. Also, a paper in the Journal of the American Medical Association found rising mortality rates among U.S. children and adolescents…
- The panel looked at American life and death in terms of the public health and medical care system, individual behaviors like diet and tobacco use, social factors like poverty and inequality, the physical environment, and public policies and values. “In every one of those five buckets, we found problems that distinguish the United States from other countries.”
- Yes, Americans eat more calories and lack universal access to health care. But there’s also higher child poverty, racial segregation, social isolation, and more. Even the way cities are designed makes access to good food more difficult.
- “Two years difference in life expectancy probably comes from the fact that firearms are so available in the United States,” Crimmins says. “There’s the opioid epidemic, which is clearly ours – that was our drug companies and other countries didn’t have that because those drugs were more controlled. Some of the difference comes from the fact that we are more likely to drive more miles. We have more cars,” and ultimately, more fatal crashes.
My take (from authors): “the focus should… be on the fact that every other rich country has been able to figure out how to help people live longer, healthier lives. That means that Americans could do it too.” Meanwhile, lawmakers across the country are protecting kids from harm by stopping drag shows, banning books, and preventing care for transgender kids.
Related blog posts:
- No Exaggeration: Too Many Children Are Dying in the U.S.
- Firearms: #1 Cause of Pediatric Deaths & Households with Guns =More Deaths
- Opioid Epidemic -Devastating Impact on Children (images and Link)
- Today’s Children in Crisis: YOYO
- “Crossing Lines” and Why Firearm Deaths are The Leading Cause of Death in Children
- “A Smarter Way to Reduce Gun Deaths” Plus Two
- Suicide Rate Up 33% in Last 20 Years & Can We Stop It?