S Lawrence et al. JPGN 2022; 75: 601-607. Optimized Infliximab Induction Predicts Better Long-Term Clinical and Biomarker Outcomes Compared to Standard Induction Dosing
In this retrospective observational cohort study (n=140 children), patients were started on 5 mg/kg/dose during induction. 78 children had “optimized dosing” with an infliximab level drawn prior to 3rd dose. A level <15 mcg/g was considered subtherapeutic. It is noted that combination therapy was much higher in the standard (not optimized) group (95% vs 42%).
Key findings:
- Combined corticosteroid-free clinical and biomarker remission (CRP < 5 mg/L) was higher in the optimized compared to the standard cohort [65/78 (83%) vs 25/62 (40%), P < 0.001]. Remission rates correlated with trough levels; those in clinical remission had a median level of 3.6 compared to 2.0 in those without clinical remission.
- The median post-induction trough was higher in the optimized group 4.2 mg/L vs 1.9 mg/L.
- The optimized group were significantly more likely to achieve a therapeutic level (5 mg/L or greater): 44% vs 18%.
My take:
- The “optimized” group was not very well optimized –only 44% had a therapeutic level >5, but still performed much better than the standard group (which more often had combination therapy). This indicates a need to start with higher doses and reinforces the need for therapeutic drug monitoring.
- This study further shows that 5 mg/kg dosing is inadequate. In the standard group, even with combination therapy, only 18% achieved therapeutic levels.
- This article will be another one to include to try to persuade insurance companies that kids are different and need higher doses of infliximab.
- Though inconvenient for families, dosing more frequently is more effective than higher doses for improving trough levels (ie 5 mg/kg q4 wks results in better trough levels than 10 mg/kg q8 wks).
Here are some additional references on this topic (from a recent appeal):
For pediatrics, studies have shown that utilizing dosing of 5 mg/kg/dose results in subtherapeutic dosing in around 80%, especially if low albumin. This places patients at high risk for developing antibodies to infliximab and complications from Crohn’s disease.
- LE Bauman et al Inflamm Bowel Dis 2020 Feb 11;26(3):429-439. Improved Population Pharmacokinetic Model for Predicting Optimized Infliximab Exposure in Pediatric Inflammatory Bowel Disease. The authors identified 228 pediatric patients with IBD and developed a pharmacokinetic model using weight, albumin, sedimentation rate and antibodies to infliximab (ATI) to help predict infliximab dosing that would achieve a therapeutic trough level (>5 mcg/mL). In their study, they also simulated 1000 patients and found that only 24% of patients receiving 5 mg/kg q8weeks achieved a therapeutic level; this increased to 56% for 10 mg/kg q8weeks
- Frymoyer A, Piester TL, Park KT. JPGN. 2016;62(5):723-727. Infliximab dosing strategies and predicted trough exposure in children with Crohn’s disease. Only 21% of children in this modeling study achieved a trough level >3 if the albumin was 3 or lower. The goal for trough level is NOW >5.
- JM Shapiro et al. JPGN 2016; 62: 867-72. Durability of Infliximab Is Associated With Disease Extent in Children With Inflammatory Bowel Disease. In this study with 98 pediatric patients, 70% with extensive disease required dose escalation.
- Ungar B, Levy I, Yavne Y, et al. Clin Gastroenterol Hepatol. 2016;14(4):550-557.e552. Optimizing Anti-TNF-alpha therapy: serum levels of Infliximab and Adalimumab are associated with mucosal healing in patients with inflammatory bowel diseases. Getting good levels important to achieve healing/remission.
- NV Castelle et al. Clin Gastroenterol Hepatol 2022; 20: 465-467. Patients With Low Drug Levels or Antibodies to a Prior Anti-Tumor Necrosis Factor Are More Likely to Develop Antibodies to a Subsequent Anti-Tumor Necrosis Factor. Good levels are associated wtih fewer antibodies to infliximab.
Related blog posts:
- “Denials, Dilly-dallying and Despair”
- Kids Are Different: Therapeutic Drug Monitoring
- Modeling Trough Levels to Predict Optimal Infliximab Dosing
- Improving Outcomes with Proactive Therapeutic Drug Monitoring (JAMA 2021 study)
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy?
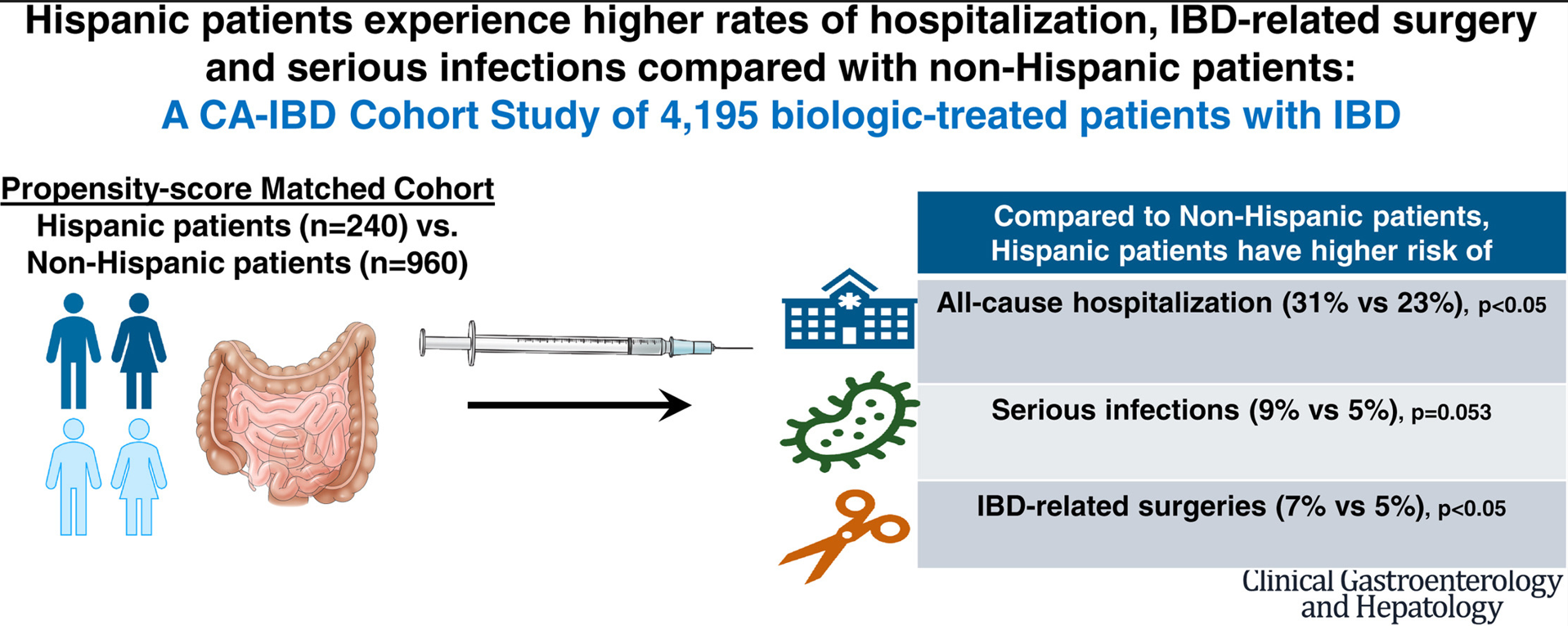
- IBD Updates: Understanding Newest IBD Therapies for Kids- Bowel Sounds, Hispanic Patients with IBD, More on Intestinal Ultrasound
- Real-World Experience with Proactive Therapeutic Drug Monitoring in Inflammatory Bowel Disease
- Here’s The Proof That Proactive Drug Monitoring Improves Outcomes in Children With Crohn’s Disease
- Combination Therapy Study Points to Central Role of Adequate Drug Levels | gutsandgrowth
- Proactive Therapeutic Drug Monitoring -Different Time Points | gutsandgrowth
- For the Next Insurance Appeal: Therapeutic Drug Monitoring in Adalimumab Treatment (Pediatrics) & Satire on Prior Authorizations
- Expert Consensus: New Recommendations for Therapeutic Drug Monitoring | gutsandgrowth

On a recent trip to Florida, we picked up more than 40 sand dollars on a morning beach walk. This was during a cold snap, at low tide and after a storm.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.