JD Lewis et al. Clinical Gastroenterology and Hepatology. 2024; Volume 22, Issue 12, 2475 – 2486.e14. Open Access ! Provider Specialization in Inflammatory Bowel Diseases: Quality of Care and Outcomes
Methods: This was a retrospective cohort of newly diagnosed patients with IBD using data from Optum’s deidentified Clinformatics Data Mart Database (2000–2020). The study included 772 children treated by 493 providers and 2864 adults treated by 2076 providers.
Key findings:
- In adults, care from an IBD-focused provider was associated with more use of biologics, combination therapy, and imaging and endoscopy, and less mesalamine use for Crohn’s disease (P < .05 for all comparisons)
- In children, none of the associations between provider focus and process or outcome measures were significant. Although not statistically significant among children, the OR for mesalamine use was 0.64, suggesting a similar association as that seen among adults
My take: This study indicates significant treatment disparities between IBD-focused care providers and providers without an IBD focus in the care for adults, but not in the care of children. This could be related to improved collaboration among pediatric care providers, better training, and parental involvement.
In addition, this study focused on patients with newly-diagnosed disease. Treatment is more complicated in patients who have not responded to initial treatments; as such, IBD-focused providers may be more important in this population.
Related blog posts:
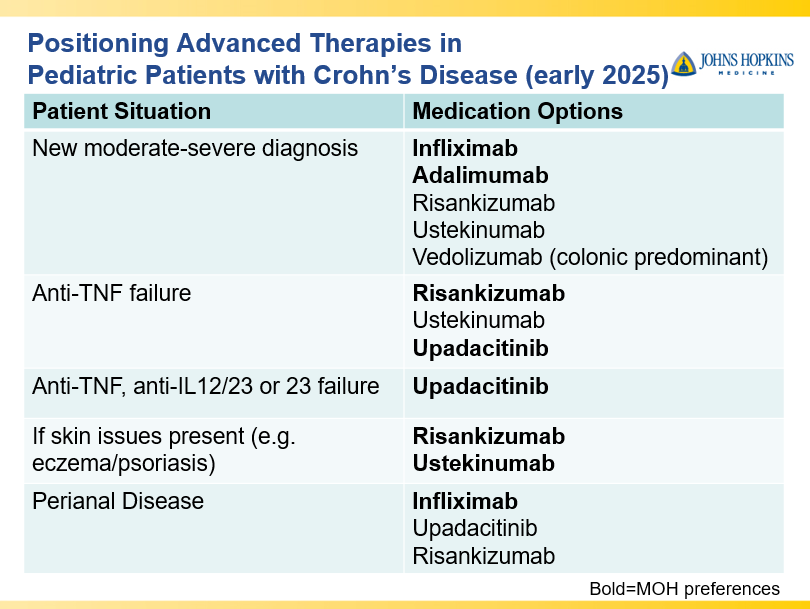
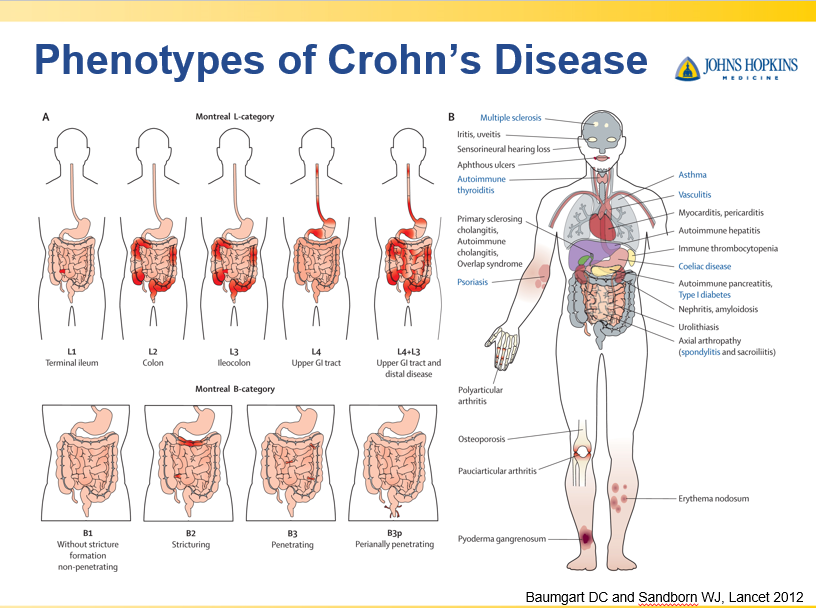
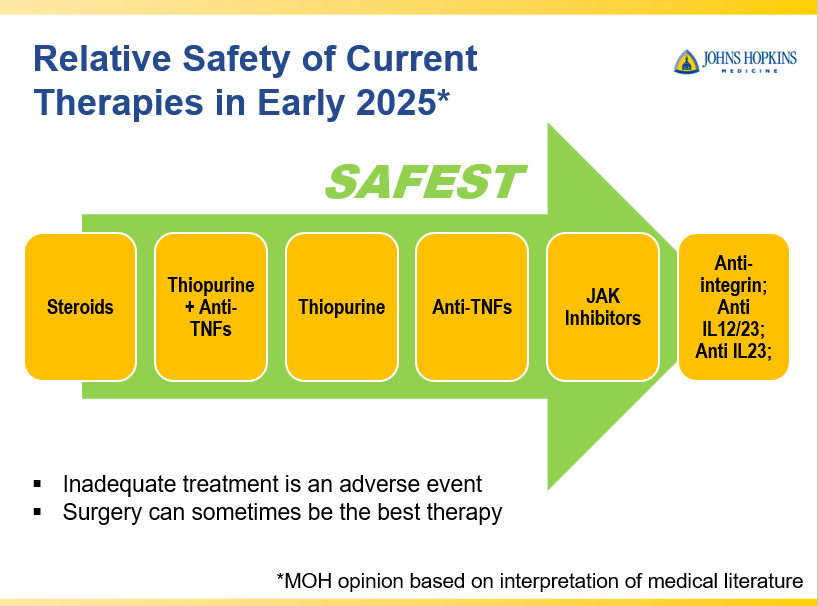
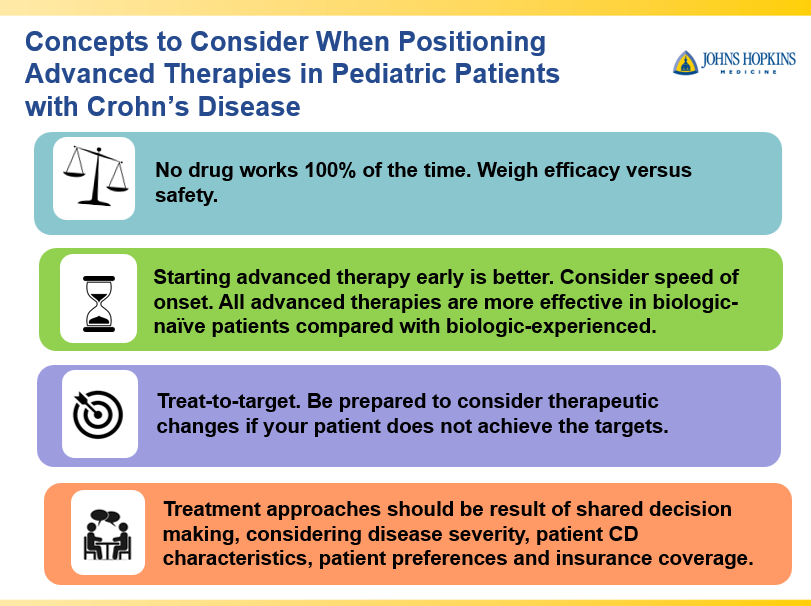
- Dr. Maria Oliva-Hemker: Positioning Therapies for Pediatric Crohn’s Disease
- Dr. Joel Rosh: Positioning Therapies for Pediatric Ulcerative Colitis
- 2021 AGA Guidelines For Crohn’s Disease
- AGA Living Guideline for Moderate-to-Severe Ulcerative Colitis –The Good and The Bad
- AGA Guidelines: Moderate to Severe Ulcerative Colitis
- AGA Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis