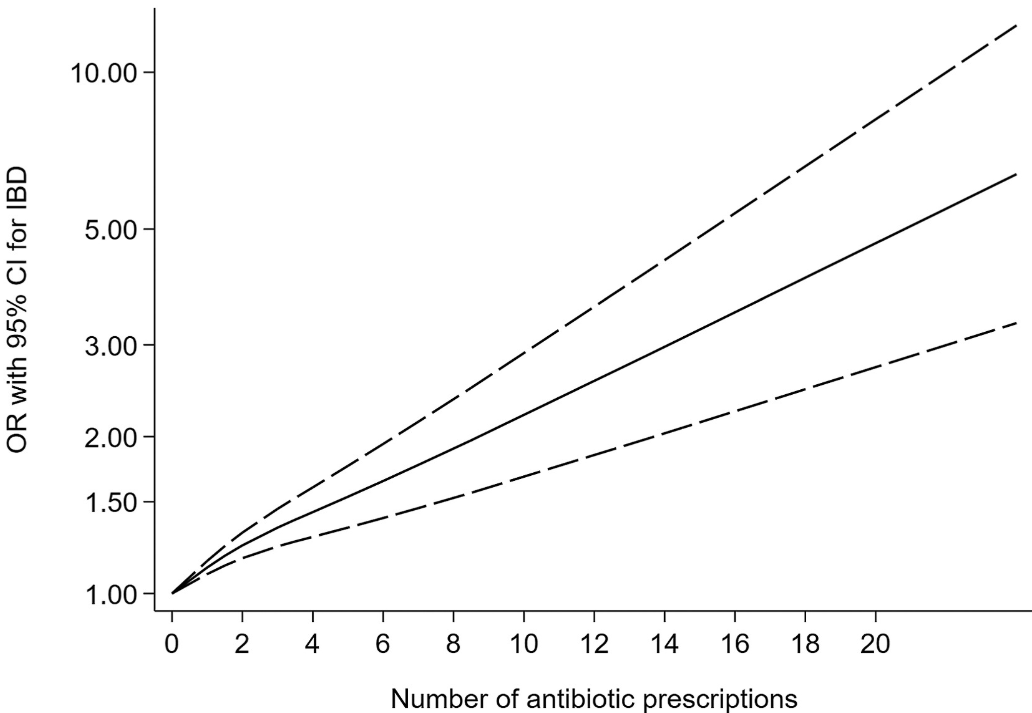
R Duan et al. Clin Gastroenterol Hepatol 2025; 23: 45-58. Open Access! Antibiotic Exposure and Risk of New-Onset Inflammatory Bowel Disease: A Systematic Review and Dose-Response Meta-Analysis
Twenty-eight studies involving 153,027 patients with IBD were included.
Key findings:
- Antibiotic exposure was significantly associated with an increased risk of new-onset IBD for prescription-based studies (pooled OR, 1.41; 95% CI, 1.29–1.53) and for questionnaire-based studies (pooled OR, 1.35; 95% CI, 1.08–1.68). ‘
- This association existed for both Crohn’s disease and ulcerative colitis, as well as in children and adults for prescription-based studies.
Some of the limitations:
- There was statistical heterogeneity was high in the primary analysis, possibly because of inconsistencies in study design
- Most studies included a clear lag time, yet an inadequate lag time still creates the possibility of reverse causality.
- The authors could not disentangle the risk of antibiotics from the risk of infection in leading to the development of IBD.
My take: This is another study showing an association between antibiotic use and new-onset IBD. While this study does not prove causation, it is another reason for good antibiotic stewardship.
Related blog posts:
- IBD Brief Updates: Anti-TNF Loss of Response, Upadacitinib for ASUC, Risk Factors for Developing IBD
- Risk Factors for Inflammatory Bowel Disease: Antibiotics (Part 2)
- Early Antibiotics -Minimal Risk for Crohn’s Disease
- Efficacy of Anti-TNF Agents for Internal Fistulas and Study of Antibiotics and Development of IBD