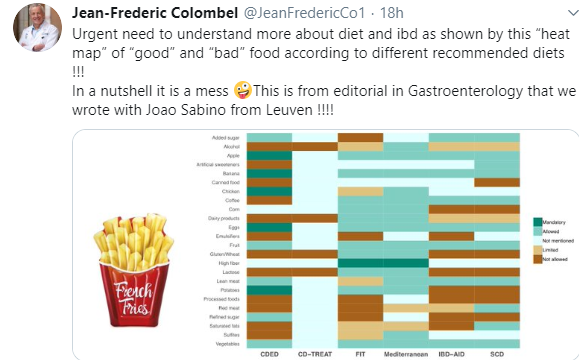
As noted in a previous blog (IBD Briefs August 2019), there have been numerous diets proposed to help with Crohn’s disease. The chart below illustrates the lack of any consensus.
Related blog posts:
- The Search for a Dietary Culprit in IBD | gutsandgrowth
- CD-TREAT Diet: Pushing the Boundaries on Diets for Crohn’s Disease
- Crohn’s Disease with Isolated Colonic Involvement Less Responsive to EEN
- Practical Advice on Enteral Nutrition | gutsandgrowth
- Head-to-Head: Enteral Nutrition vs. anti-TNF
- Gut Microbiome, Crohn’s Disease and Effect of Diet …
- Top Lecture: Enteral Nutrition for Crohn’s Disease …
- There is No Healthy Microbiome
- Why Does Enteral Nutrition Work for Crohn’s Disease? Is it due to the Microbiome?