Briefly noted from Twitter:
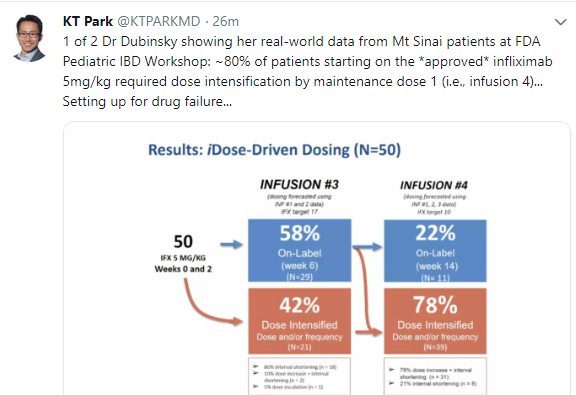
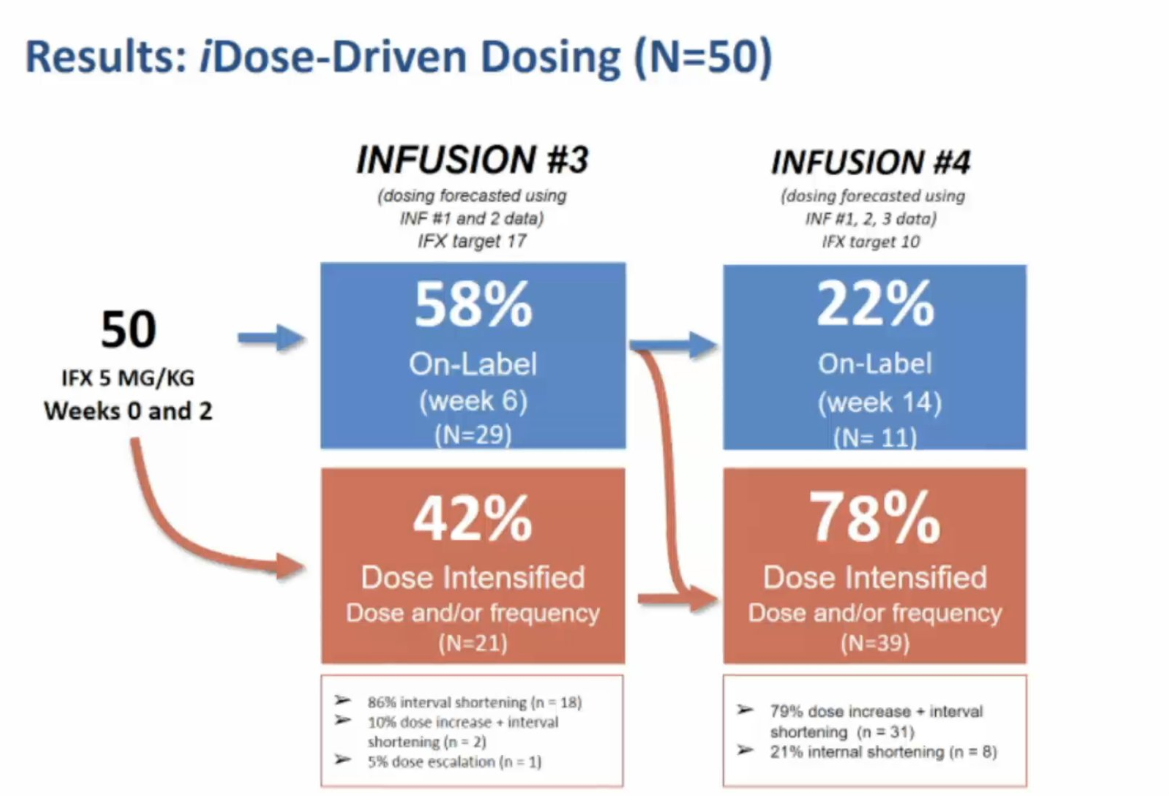
Close up of previous image
Also –with regard to Methotrexate:


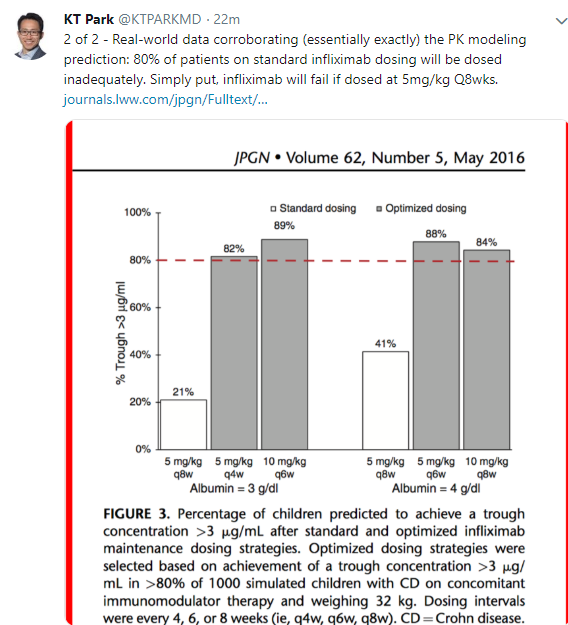
Briefly noted from Twitter:
Close up of previous image
Also –with regard to Methotrexate:
A recent study (J-W Huaman et al. Gastroenterol 2018; 155: 1004-7) examined the effects of a prebiotic (Bimuno) and a low FODMAPs diet for the treatment of functional GI disorders and their effects on the microbiome.
This was a randomized controlled 4-week trial with a 2-week followup period. Those who received the prebiotic (N=19) received a placebo diet (Mediterranean-type) and those who were randomized to a low FODMAP diet (n=21) were instructed to consume a placebo. The prebiotic contained beat-galactooligosaccharide.
Key findings:
My take: (borrowed from editorial pg 960-2): This study “may indicate that the effect of the prebiotic is mediated through its effects on gut microbiota composition, whereas the effect of the low FODMAP diets is more related to the meal composition…than to its effects on gut microbiota composition.”
Related blog posts:

From two of the missions in San Antonio



Briefly noted: SC Shah, H Khalili et al. Gastroenterol 2018; 155: 1079-89.
This study evaluated pooled data with 207,600 incident cases of IBD from a population of 478 million. Key findings:
My take: the differences indicate that genetic factors (men with a Y chromosome and only one chromosome X) along with sex hormones play a role in the pathogenesis of IBD.

Graphs depict Female/Male Incidence Rate Ratio
AGREE proceedings: Briefly noted: ES Dellon, CA Liacouras, J Molina-Infante, GT Furuta et al. Gastroenterology 2018; 155: 1022-33. This report provides updated recommendations from AGREE conference –which have been widely cited previously on this blog and elsewhere. One of the remarkable features on this report is the fact that there are 64 authors (by my count) –thus reading the affiliations and the conflict of interest disclosures alone would take some time.
For a good review on this topic:

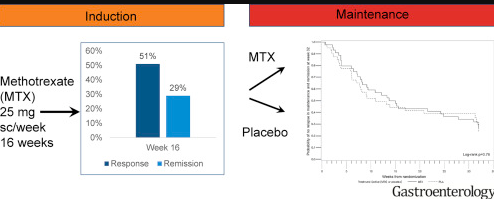
A recent study (H Hansfarth et al. Gastroenterol 2018; 155: 1098-1108) examined the use of methotrexate for ulcerative colitis (UC). The authors performed a 48-week trial (MERIT-UC trial) with 179 patients with a mean age of 42 years in the induction period. In those who improved during induction, methotrexate was continued in 44 patients and compared to 40 patients who received placebo; this was a double-blind, placebo-controlled trial.
Key findings:
The associated editorial by Dulai (pg 967-69) which reviewed this study and a prior study (METEOR) comes to the conclusion that: “there is likely no place for methotrexate monotherapy in UC.”
Related blog posts:
Briefly noted: N Chanchlani et al. JPGN 2018; 67: 513-9. The authors report on the use of infliximab biosimilar (IFX-B), n=82, compared to infliximab originator (IFX-O) in 175.
My take: This study, due to incomplete data, does not add much to our knowledge about biosimilars. It does indicate that better screening prior to infusions for HBV and tuberculosis is needed along with more well-documented experience.
Related blog posts:

Peyto Lake, Banff
G Horneff et al. J Pediatr 2018; 201: 166-75. This industry-funded analysis of 577 pediatric patients who received adalimumab (1440 patient-years) identified no new safety signals. The most common serious infection was pneumonia (0.6 events per 100 patient-years). The most common adverse events were respiratory tract infections/nasopharyngitis. Serious infections were more common in the subset of patients with Crohn’s disease (CD), (n=189), occurring in 13%.
PS Dulai et al. Gastroenterol 2018; 155: 687-95. This study, using data from GEMINI 2 phase 3 trial with 814 patients, developed a clinical prediction tool for determining the likelihood of a clinical response to vedolizumab. Common predictors for response:
R Matro et al. Gastroenterol 2018; 155: 696-704. The authors performed a prospective study of women with IBD and their infants (n=72). They “detected low concentrations of infliximab, adalimumab, certolizumab, natalizumab, and ustekinumab in breast milk samples. We found breastfed intants of mothers on biologics, immunomodulators, or combination therapies to have similar risks of infection …compared to non-breastfed infants or infants unexposed to these drugs.”

MA Manfredi et al. JPGN 2018; 464-8. This retrospective chart review describes the use of endoscopic electrocautery incisional therapy as a treatment for refractory benign esophageal anastomotic strictures (n=57) from 2011-2017.
The authors define refractory as inability to achieve an adequate esophageal lumen diameter after 5 dilatations to the following:
Key findings:
Role of this therapy/technical aspects:
My take: This is a promising treatment for a stubborn problem though its use will require advanced therapeutic experience. As an aside, I think their definition of success is at odds with common sense.
Related blog posts:

The first bear I saw in Banff
Recent studies point to huge advances in cystic fibrosis (CF) therapy. Though as noted in a previous blog (Why Do Canadians with Cystic Fibrosis Live Longer?), medical advances may have limited effect based on a lot of issues including access to care.
Despite that note of caution, it is hard not to be excited about a couple of recent publications which show that triple cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapy has great potential to improve outcomes for CF patients.
Background: In the editorial, the pathophysiology of the defect of CF is discussed and how the newer medicines either act as a potentiator of the CFTR (ivacaftor) or as corrector (lumacaftor and tezacaftor). Potentiators increase CFTR channel opening at the cell surface whereas correctors increase the amount of CFTR protein at the cell surface. One caveat has been that these therapies had not been proven effective, individually, for Phe508del CFTR mutation which occurs in “approximately two thirds of patients.” Combination therapy has helped in most of this group but not in those with Phe508del-minimal function (MF).
The new studies examine triple therapy with the addition of two new-generation small molecule correctors: VX-445 and VX-659. These new correctors target different sites of the CFTR protein.
Key findings:
My take: These reports “represent a major breakthrough…for improving health and possibly survival in all patients who carry the most common CFTR mutation.” Long-term outcomes will need to be followed to confirm these findings.
Related blog posts:
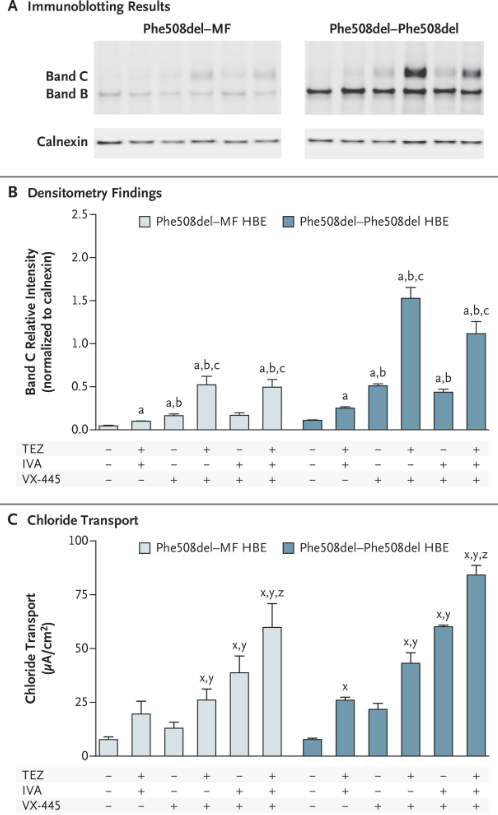
This is Figure 2 from Davies study showing immunoblot findings, densitometry findings, and chloride transport in bronchial cells. The most robust responses were with triple therapy

I did not make it to this year’s meeting but did get a chance to catch up on a lot information via the PG 2018 Syllabus and based on information posted online.
Here are a couple of highlights for me:
My favorite slide from postgraduate course -Dr. Robert Kramer
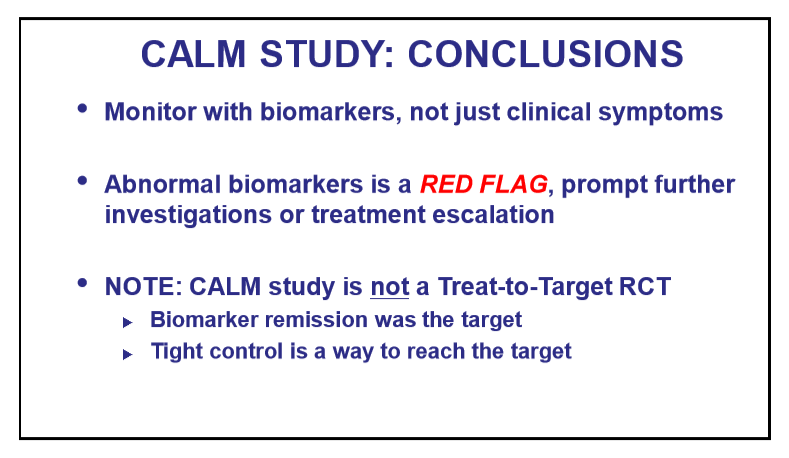
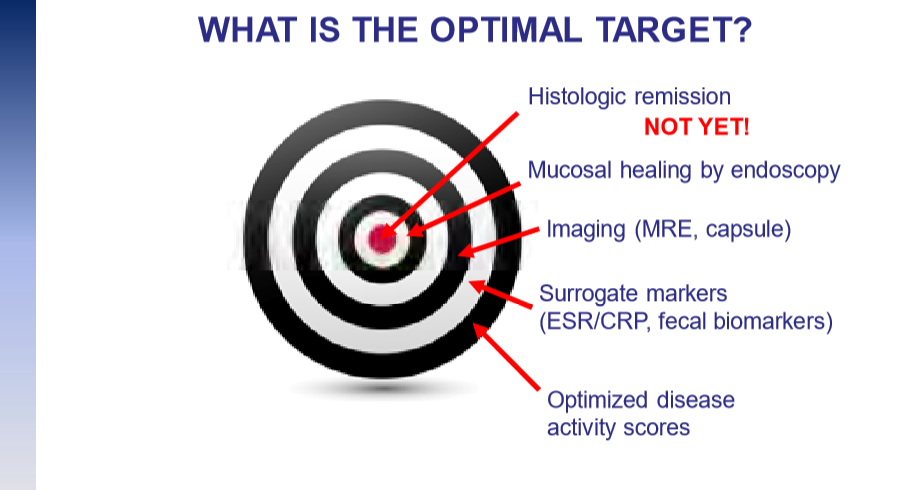
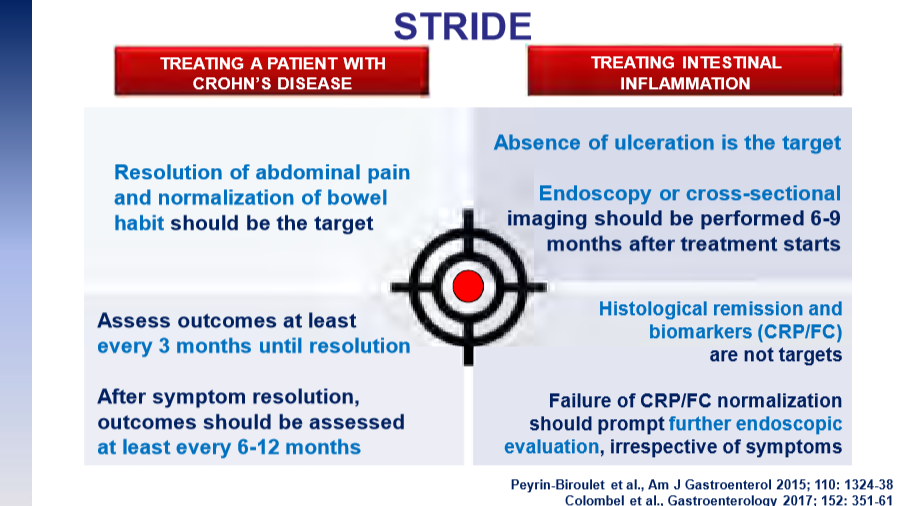
Slides regarding the topic of Treat-toTarget Dr. Eric Benchimol:
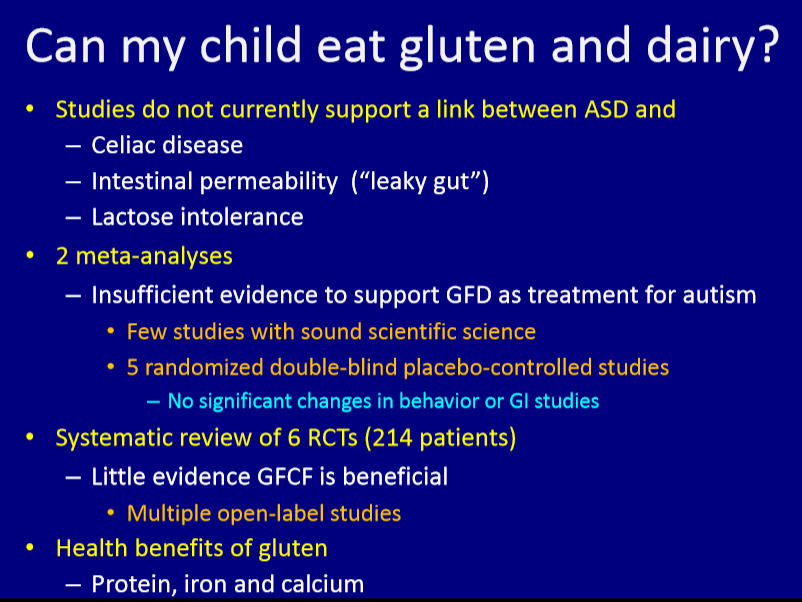
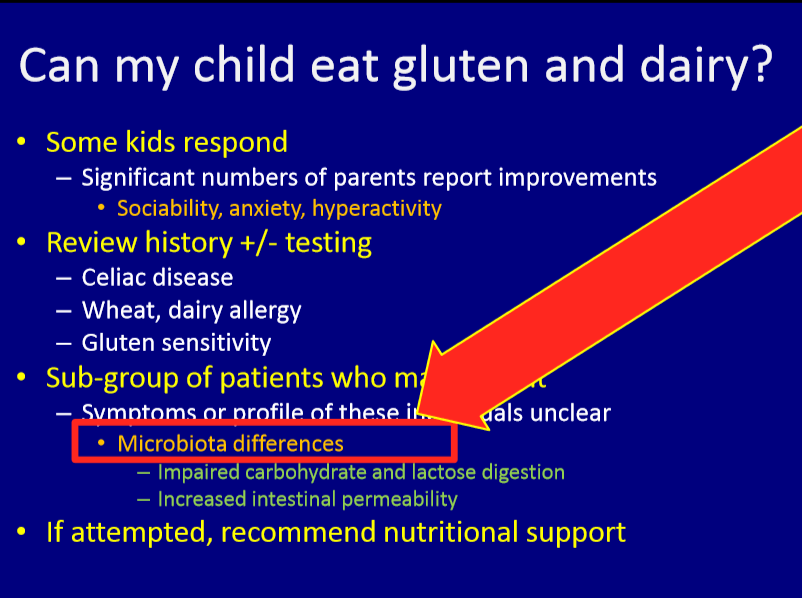
Slides regarding GI symptoms and autism from Dr. Kara Margolis:
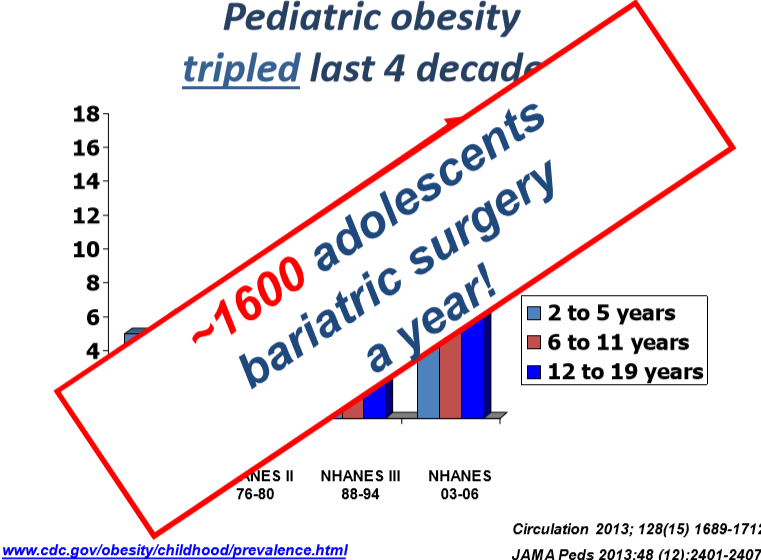
Slide regarding the frequency of bariatric surgery: Dr. Rohit Kohli:
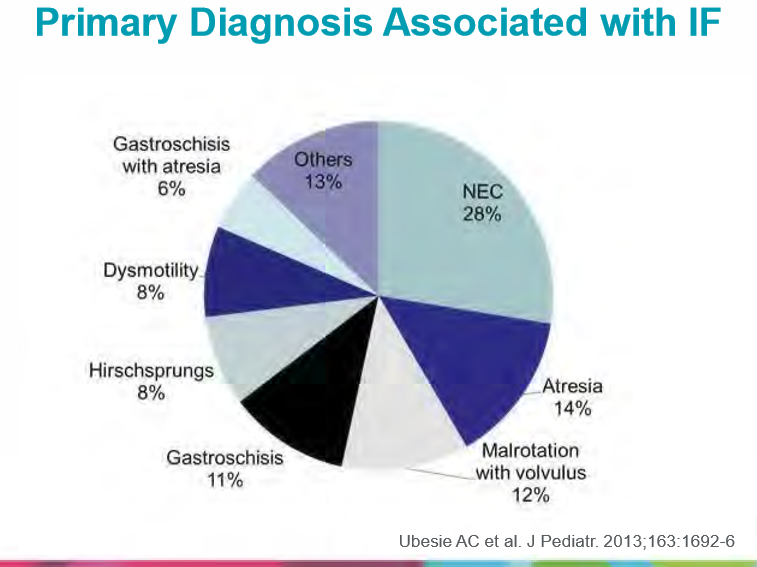
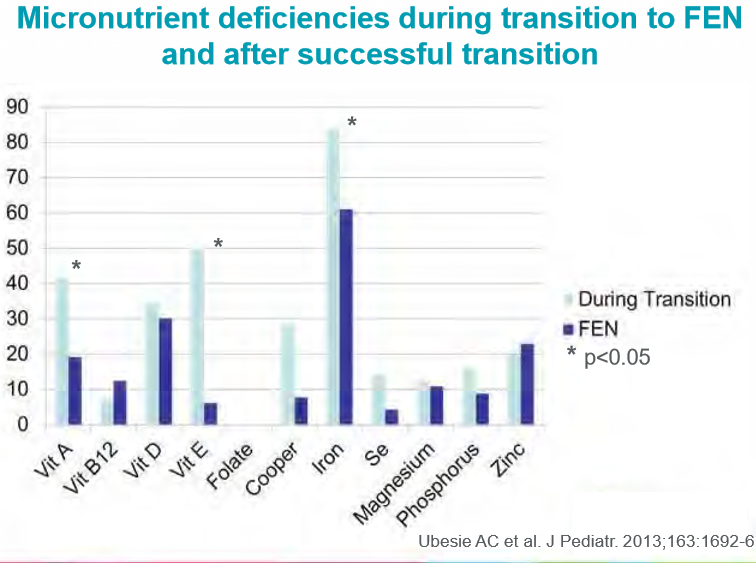
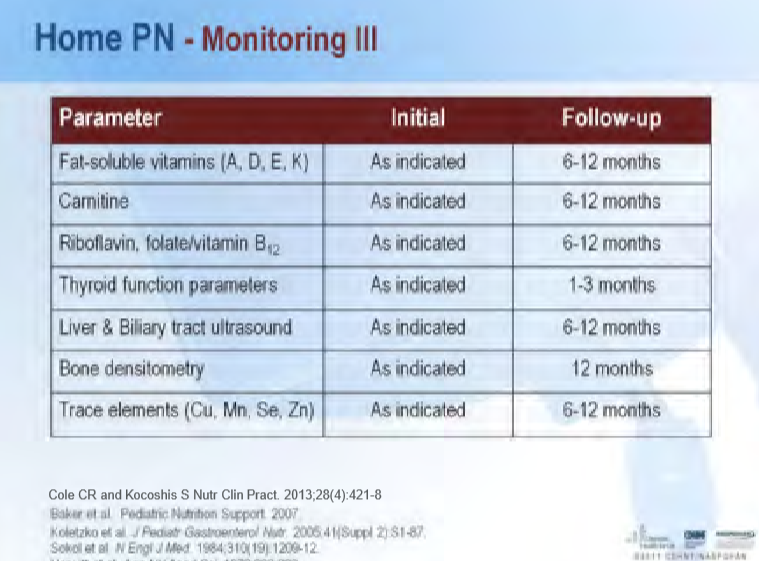
Slides regarding intestinal failure population from Dr. Conrad Cole:
From Dr. Miranda van Tilburg regarding psychological therapies for functional GI disorders:

Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
I did not make it to this year’s meeting but did get a chance to catch up on a lot information via the PG 2018 Syllabus and based on information posted online.
Here are a couple of highlights for me:


Slides from postgraduate course on CVS from Dr. Katja Kovacic



The slide from Dr. Lightdale (pg 22 in Syllabus) below suggests it is OK for scope if platelets >20K and OK for biopsies if platelets >50K. It is worth noting that some adult data indicate that even lower biospy thresholds are reasonable for biopsies (Post: Lower Endoscopic Thresholds for Thrombocytopenia). As always, one needs to consider carefully the risks compared with the benefits.
From Postgraduate Course



Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
