I want to thank all of you who take an interest in my blog, particularly those who give suggestions, references, and encouragement. The following posts were the most popular from the past year.
Methods: Single course of oral encapsulated fecal microbiome from 4 healthy lean donors or saline placebo.
Key findings:
In this randomized, double-masked, placebo-controlled trial of 87 adolescents with obesity, FMT alone did not lead to weight loss at 6 weeks.
There were no observed effects on insulin sensitivity, liver function, lipid profile, inflammatory markers, blood pressure, total body fat percentage, gut health, and health-related quality of life
In post-hoc exploratory analyses among participants with metabolic syndrome at baseline, FMT led to greater resolution of this condition (18 to 4) compared with placebo (13 to 10) by 26 weeks (adjusted odds ratio, 0.06; 95% CI, 0.01-0.45; P = .007)
This study looked at 105 patients receiving combination therapy; the a median duration of combination therapy was 2.1 years, with infliximab and either methotrexate (53) or azathioprine (52). 89 patients had Crohn’s disease.
Key findings:
11 (10.5%) patients experienced a clinical relapse over a median duration of follow-up of 12.0 months after stopping the immunomodulator.
In the patients who did not relapse, the median IFX trough level at IM discontinuation was 6.2; the IFX trough level was 3.8 μg/mL in those who relapsed.
In their discussion, the authors urge caution in discontinuation of immunomodulators in those with clinically-severe Crohn’s disease and those with low infliximab levels.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
Collinson S, Deans A, Padua-Zamora A, Gregorio GV, Li C, Dans LF, Allen SJ. Link to website with PDF availability: Probiotics for treating acute infectious diarrhoea. Cochrane Database of Systematic Reviews 2020, Issue 12. Art. No.: CD003048. DOI: 10.1002/14651858.CD003048.pub4. Thanks to Kipp Ellsworth for this reference.
This review identified “82 studies in 12,127 people (included 11,526 children) with acute diarrhea.” Key findings:
The number of children with diarrhea longer than 48 hours was not different between those taking a probiotic and those taking a placebo
“It was unclear whether taking probiotics shortened the time spent in hospital compared with taking a placebo or no additional treatment .”
My take: Probiotics probably make little or no difference in the setting of acute gastroenteritis/diarrhea. This analysis is based on large trials with low risk of bias.
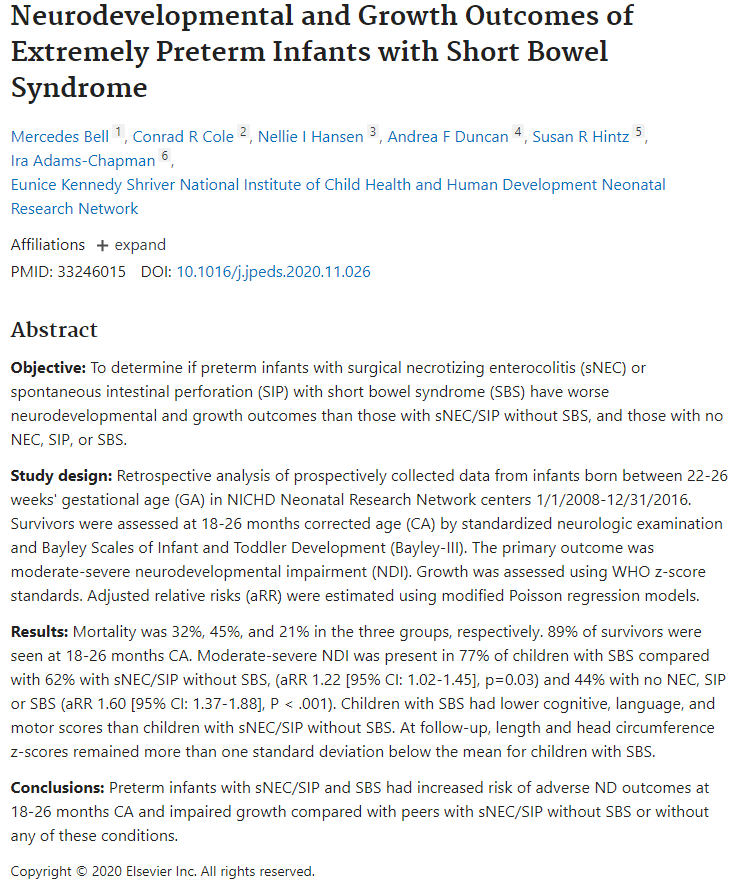
Moderate-severe neurodevelopmental impairment was present in 77% of children with extreme prematurity and with short bowel syndrome compared to 44% with extreme prematurity without necrotizing enterocolitis, spontaneous intestinal perforation or short bowel syndrome.
One of the authors, Ira Adams-Chapman, recently passed away (link to obituary: Ira Adams-Chapman, 1965-2020). She and I were residents together in Cincinnati. She was a terrific person.
“Randomized controlled trials published more than a decade ago demonstrated that exclusive enteral nutrition, wherein all table foods are eliminated from a diet and the patient relies on an elemental diet alone for nutrition, was effective in not just inducing clinical remission but also improving inflammatory biomarkers.”
“More recent rigorous studies have demonstrated that the effects of exclusive enteral nutrition can be mimicked either by a selected, less-restrictive diet (such as CD-TREAT4), which is more sustainable, or by combining partial enteral nutrition with an elimination diet that is quite diverse (such as CDED5).”
“Exclusive enteral nutrition (EEN) has been studied the most rigorously of all diets in IBD and has demonstrated the greatest benefit, compared with other diet studies in IBD. EEN requires the intake of elemental, semi-elemental, or polymeric formulas to meet all nutritional requirements without additional intake of food for 6-8 weeks. Studies have been performed mostly in pediatric populations and have shown effectiveness in induction of remission with reduction in inflammatory markers, including C-reactive protein, erythrocyte sedimentation rate, and fecal calprotectin, and even mucosal healing. EEN has not worked out as well for adult populations, because of the poor tolerability of exclusive intake of enteral formulas.”
“Beyond EEN, there are many diets that have been considered … only the SCD and Crohn’s disease exclusion diets have shown improvement in clinical remission and reduction in inflammatory markers.”
“Most dietary studies are underpowered, lack a control arm, and do not include endoscopic endpoints. The current body of evidence remains insufficient to support the use of diet alone for the treatment of IBD.”
My take: Except for exclusive enteral nutrition (EEN) which is quite challenging, dietary therapies have not been proven as effective long-term stand-alone treatments. In patients who choose dietary therapy, careful monitoring is particularly important.
In this systematic review, a total of 995 adult patients were included from 18 observational studies (4 prospective and 14 retrospective), 1 nonrandomized controlled trial, and 1 subgroup analysis of a randomized controlled trial.
Key findings:
Biologic dose de-escalation was associated with relapse rates as high as 50% at 1 year. Overall, clinical relapse occurred in 0%–54% of patients who dose de-escalated biologic therapy (17 studies).
Lower rates of relapse (10%–25%) were reported in studies involving patients with endoscopic and/or histologic remission
These results are in agreement with a previous meta-analysis, which found a 1-year risk of relapse after discontinuation of anti-TNF therapy of 36% in CD and 28% in UC ( Gisbert JP, et al.. Am J Gastroenterol 2016;111:632–47).
My take: This study shows that dose de-escalation of biologic therapy in IBD seems to be associated with high rates of clinical relapse
In this national multicenter retrospective cohort study in 207 adult patients with either active or inactive perianal Crohn’s disease (pCD) who received ustekinumab (2017-2018). The majority had received multiple biologics (~85% had at least 2 anti-TNF agents, 28% had received vedolizumab) and prior anal surgeries (mean 2.8).
Methods: Success of ustekinumab was defined by (i) clinical success at 6 months of treatment assessed by the physicians’ judgment, with (ii) no need for dedicated medical treatment for perianal lesions (antibiotics and/or topics) nor (iii) unscheduled surgical treatment. For perianal disease evaluation, clinical success was defined in the study protocol, by the absence of draining pus for fistulas, and no anal ulcers
Key findings:
In patients with active pCD, success was reached in 57/148 (38.5%) patients.
Among patients with setons at initiation, 29/88 (33%) had a successful removal.
In patients with inactive pCD at initiation, the probability of recurrence-free survival was 86.2% and 75.1% at weeks 26 and 52, respectively.
The absence of ustekinumab optimization was associated with upper odds of success (OR 2.74). “We can suppose in our present study that optimization of treatment was needed in severe refractory patients with no or insufficient response to ustekinumab. Thus, in these nonresponders, success was not achieved despite optimization.”
My take (partly borrowed from authors): “This large multicenter dedicated study adds substantial evidence to the growing literature on ustekinumab effectiveness in refractory CD.” For pCD, optimization of ustekinumab has a low likelihood of improving response.
This was a small study with 15 patients, with 9 patients having very elevated fecal calprotectin (FC) (>250) and the median level was 713 mcg/g for the entire cohort at baseline. After treatment with lumacaftor/Ivacaftor, median FC level was 102 mcg/g.
This pilot study is intriguing and makes the point that intestinal inflammation is commonly seen in children with cystic fibrosis. However, this study has some striking differences from prior studies.
My take: This study suggests that Lumacaftor/Ivacaftor is associated with a significant decrease in intestinal inflammation. When one looks at prior studies, the FC values presented in this study at baseline are much greater which could indicate significant selection bias.