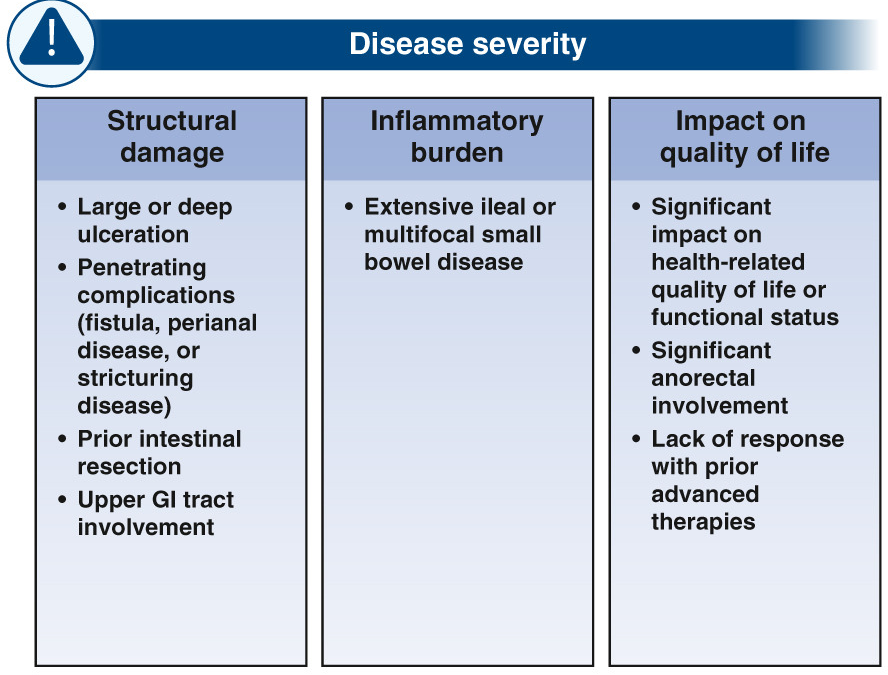
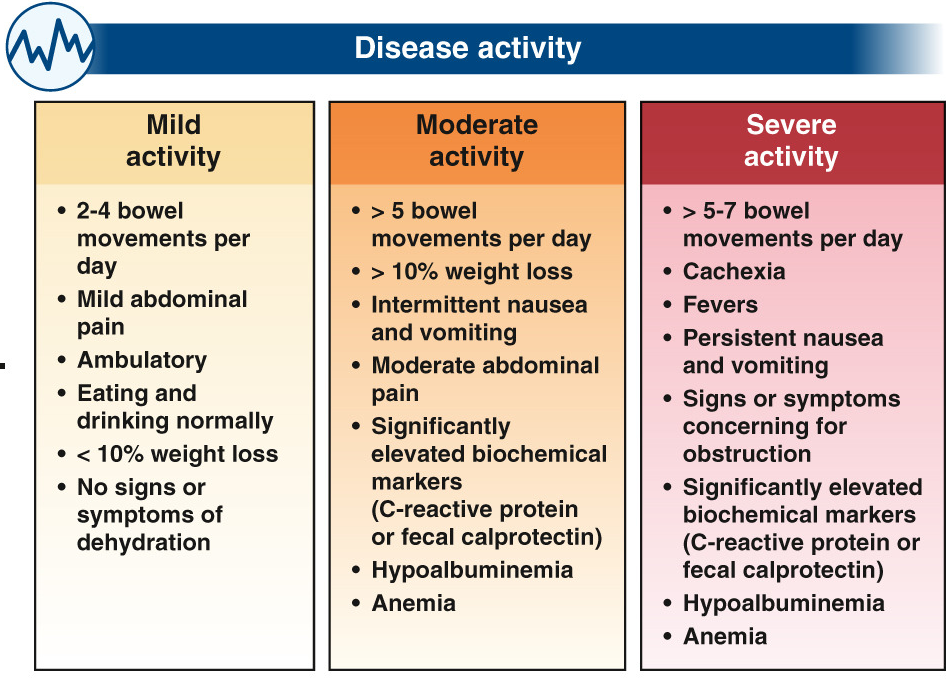
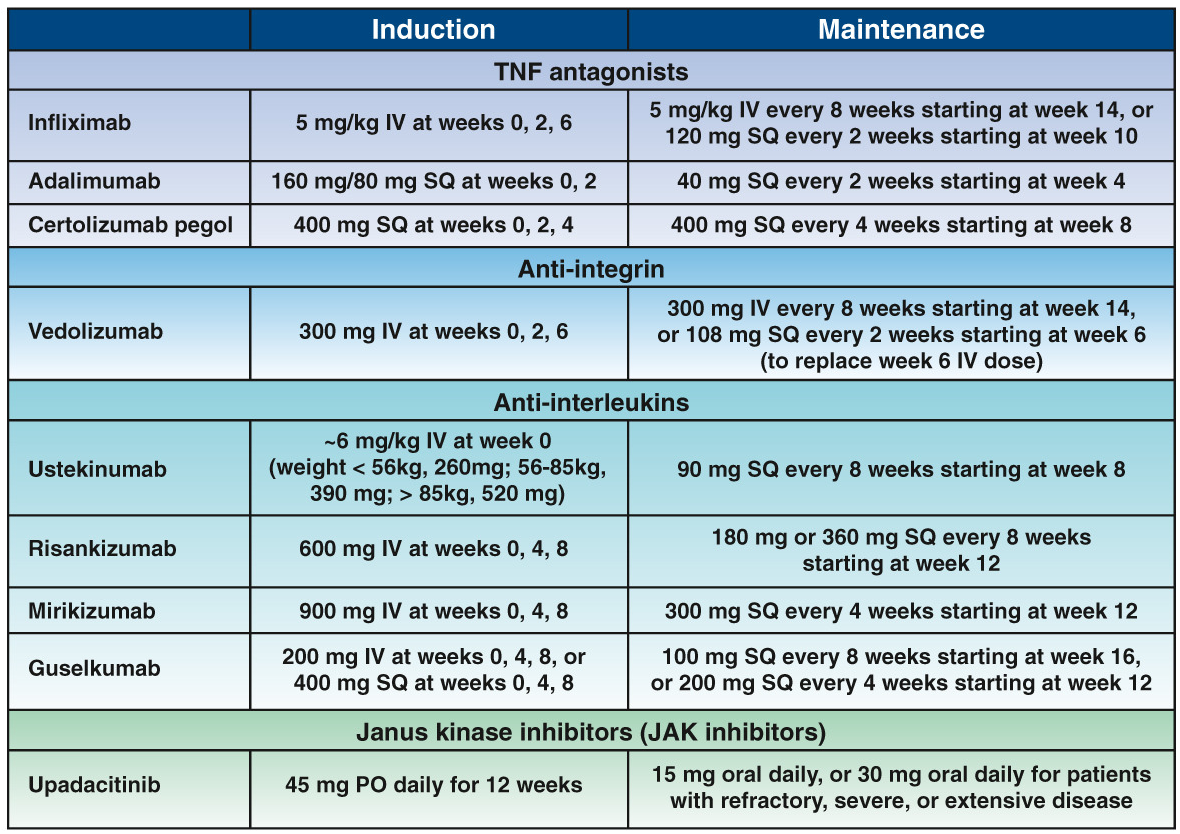
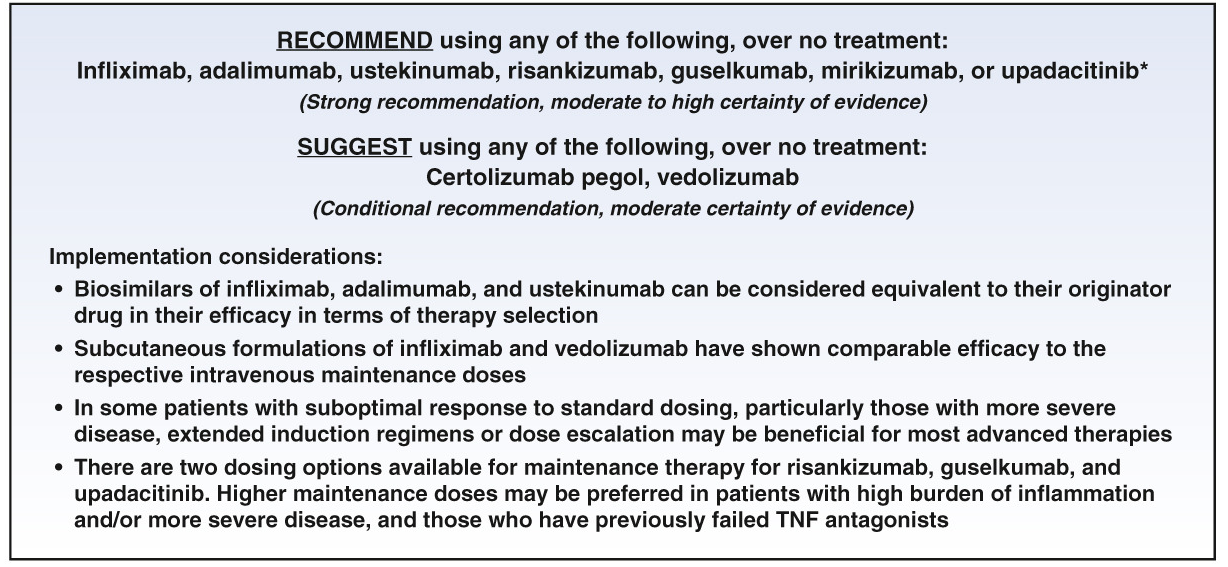
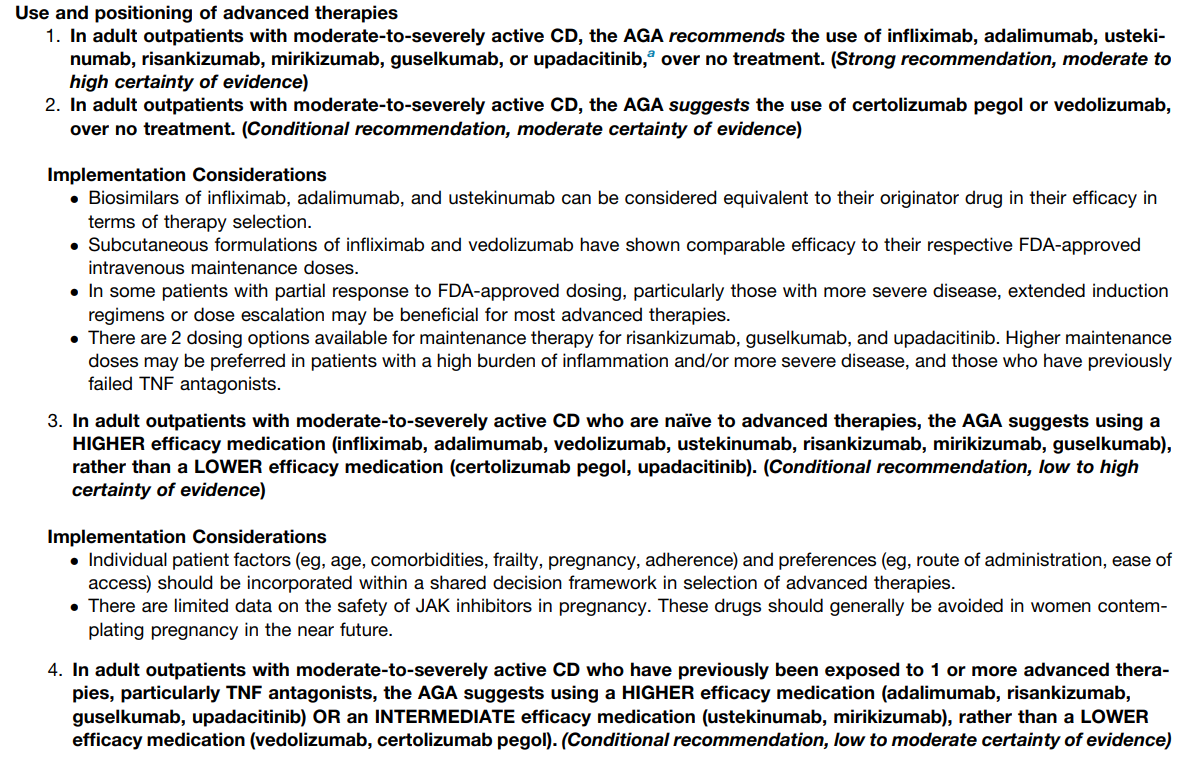
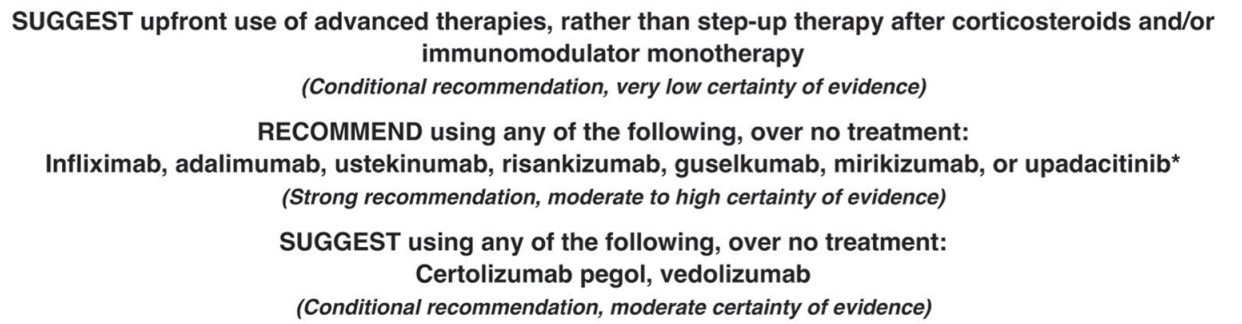
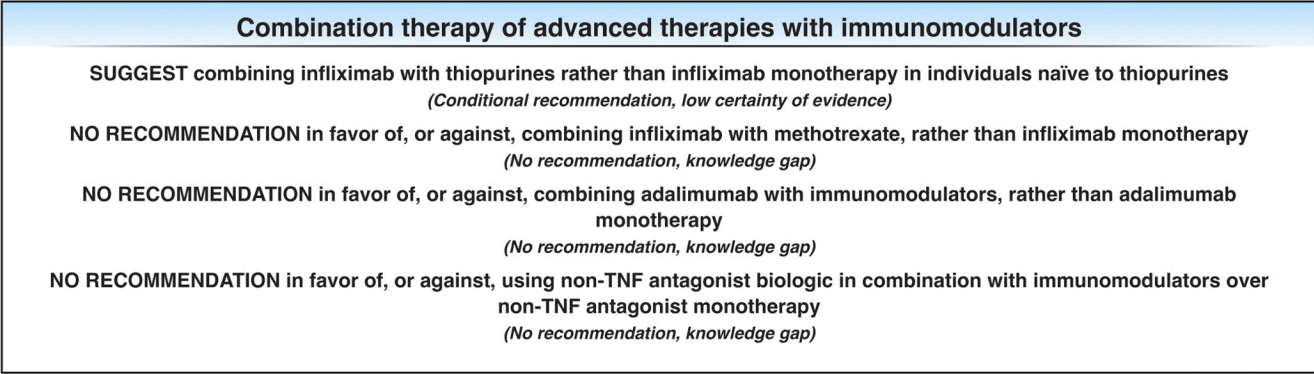
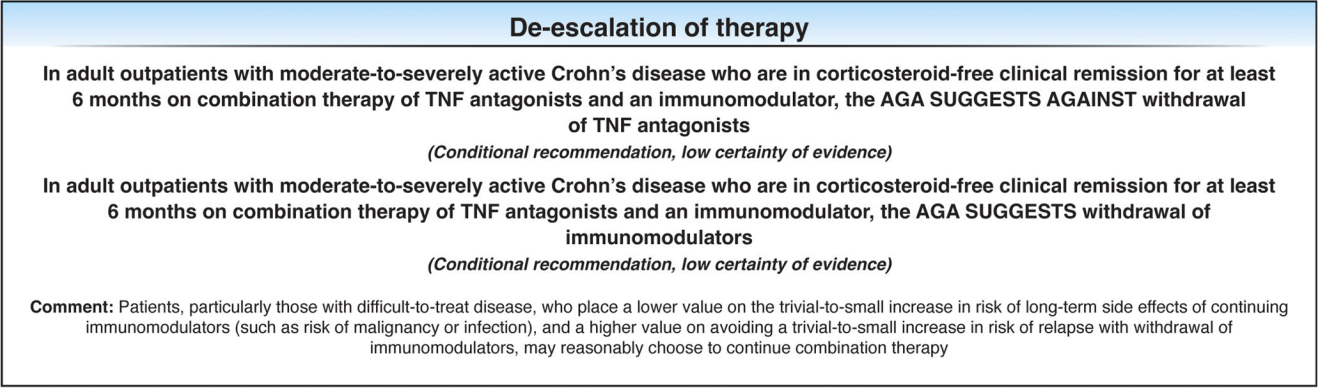
The guideline panel agreed on 16 recommendations. This highly-detailed report provides a comprehensive, patient-centered, evidence-based approach to the pharmacologic management of adult patients with moderate-to-severely active CD. Table 1 summarizes this lengthy 53-page report. Tomorrow’s post will be the “spotlight” summary which presents the recommendations in easier to read graphic.
Key Points:
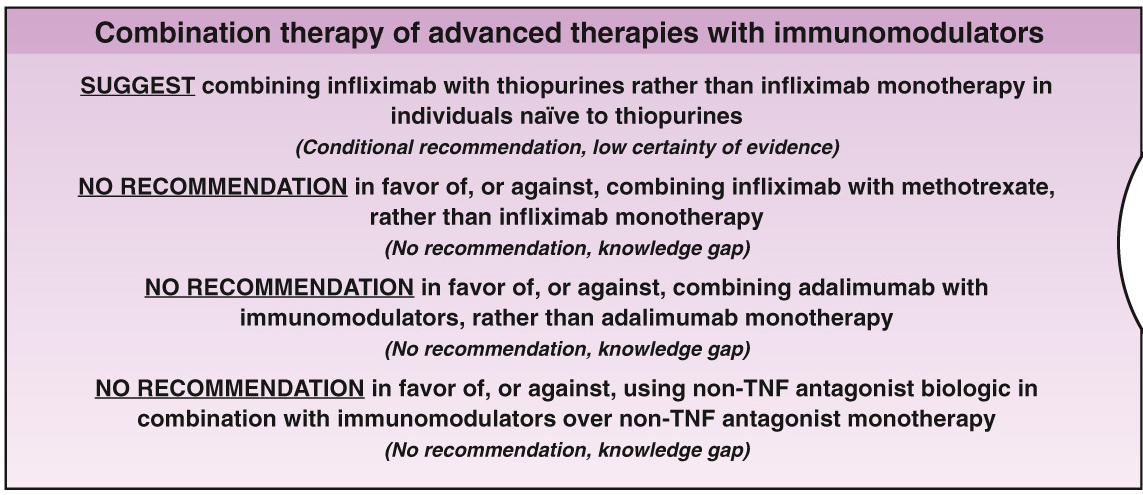
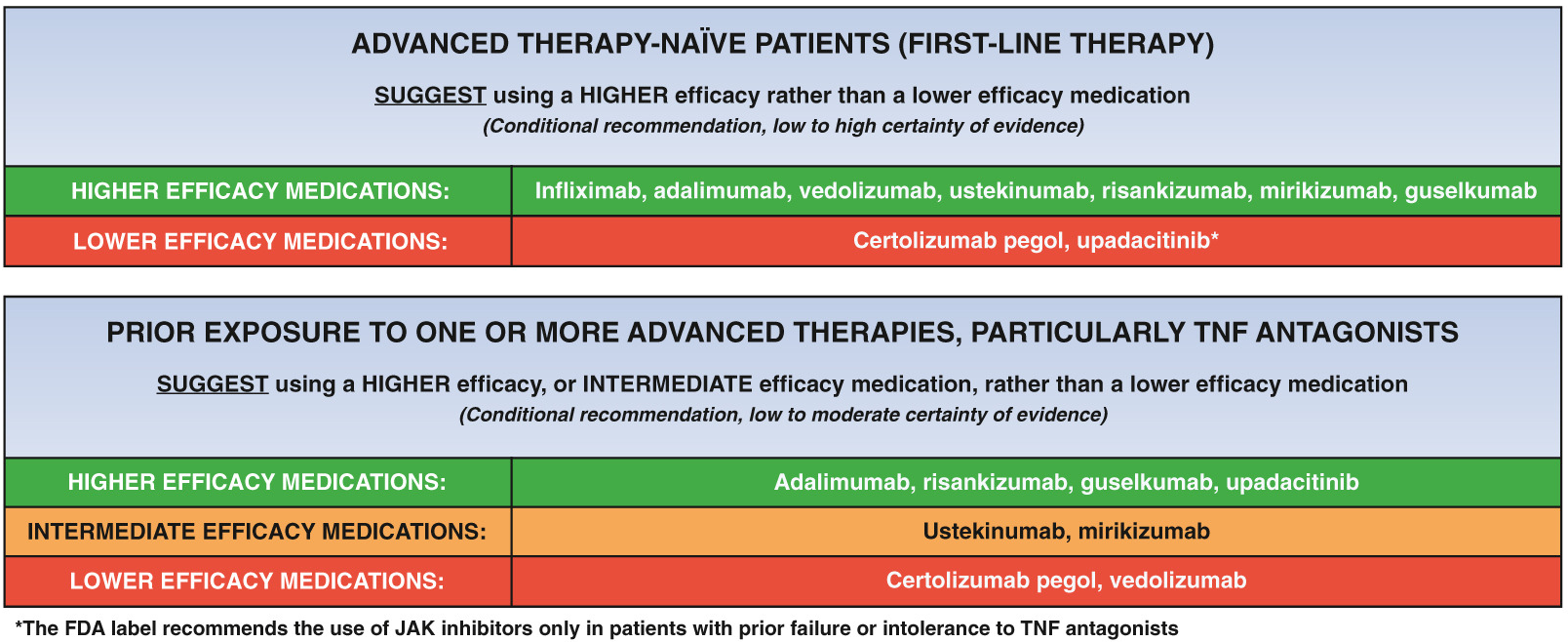
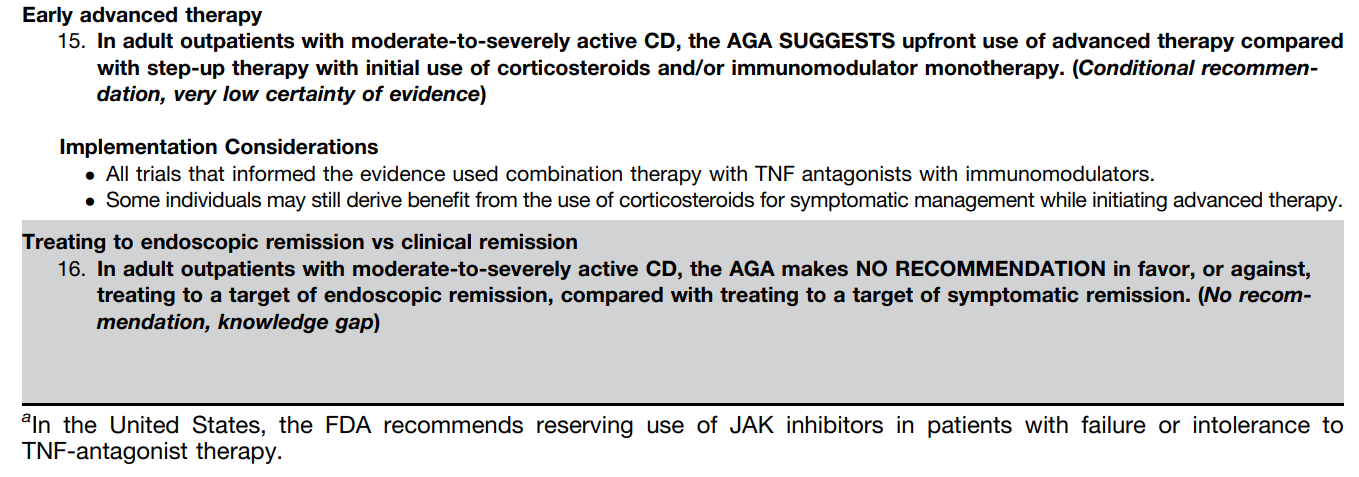
The guidelines are overall very helpful. They identify higher efficacy medications and recommend them. In addition, they support the use of combination therapy with thiopurines (which are less frequently used in pediatrics). It is interesting that the sixteenth recommendation clashes with prior expert recommendations. The sixteenth recommendation in this report makes no recommendation on using endoscopic surveillance compared to symptomatic clinical remission. Most experts advise “treat-to-target” therapy approaches.
In the discussion of this, the authors state the followiing:
“Recent position statements from an international consortium of experts have advised that longitudinal targets for the management of IBD should include not only clinical remission but also endoscopic resolution of inflammation.31 Several studies have demonstrated that patients who achieve endoscopic remission (vs those with ongoing endoscopic activity) have favorable long-term outcomes…
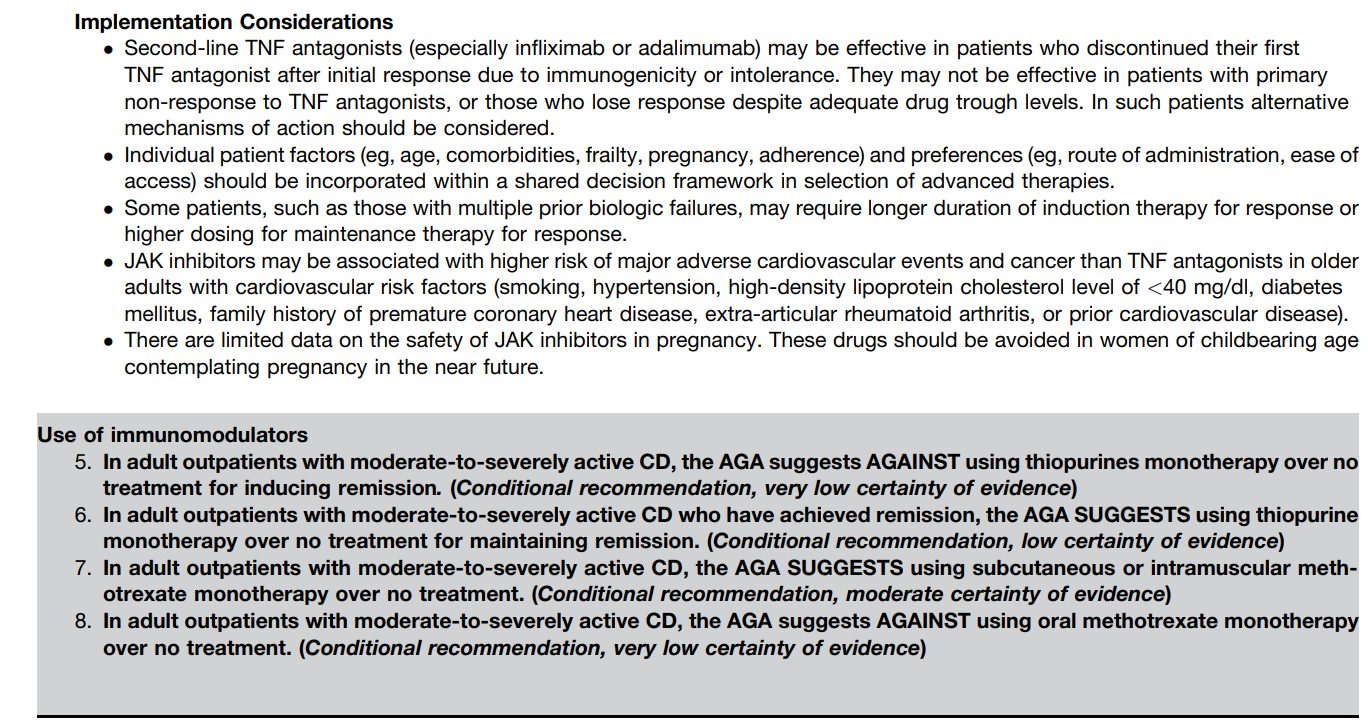
There are limited RCTs assessing whether there is actual benefit in systematically treating toward endoscopic remission target vs symptomatic remission targets (ie, testing whether the target has been achieved, followed by algorithmic treatment adjustment, including escalating index therapy, adding an immunomodulator, followed by switching to an alternative advanced therapy and surgery). There was significant heterogeneity among the 2 reviewed studies, both in terms of the advanced therapy used, algorithms for therapy modification, and the cadence and frequency of endoscopic monitoring that challenge interpretation. Based on the significant uncertainty of evidence with regard to improving maintenance of remission or reducing the risks of adverse events, the guideline panel could not make a recommendation in relation to selecting endoscopic targets over clinical targets.
It is worth emphasizing that in both of the included trials, the majority of individuals in the endoscopic healing arms were not able to meet the goal of endoscopic healing despite an algorithmic approach. For example, in STARDUST, only 11% of individuals achieved endoscopic remission.149…There are specific patient populations, such as those who have recently undergone intestinal resection,155 in which endoscopic evaluation may be particularly valuable in clinical decision making...
The benefit of a monitoring strategy incorporating biochemical monitoring over clinical monitoring alone was demonstrated in the CALM trial,152 and has been addressed in previous AGA guidelines on the role of biomarkers in patients with CD.12“
My take: These “living” guidelines are likely to be quite influential in selecting Crohn’s disease therapy. In pediatrics, ImproveCareNow provides a similar role of guiding treatment.
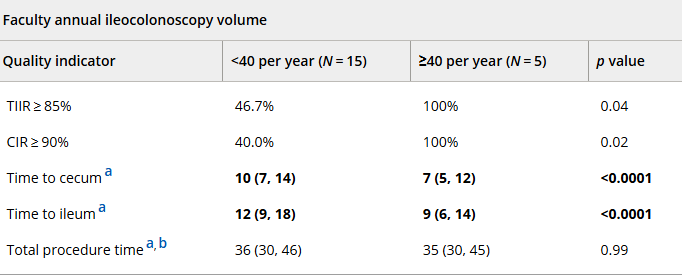
In this retrospective study with 985 ileocolonoscopies (2021-2024):
Methods: “Quality indicators were compared across groups using Kruskal–Wallis analyses. Multivariate modeling was performed to identify variables predicting terminal ileal intubation and TIIR ≥ 85%.”
Key findings:
Overall ileal intubation rate (TIIR) and cecal intubation rate (CIR) were 86.3% and 91.6%, respectively
Annual procedure volume ( APV ≥ 40) was identified as predictive for TIIR ≥ 85% (p < 0.01)
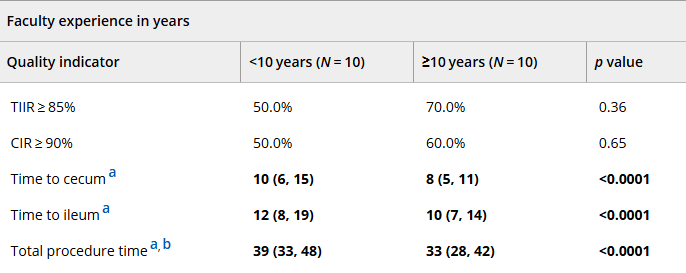
Faculty years’ experience (≥10 vs. <10 years) predicted shorter procedure duration (adjusted hazard ratio [confidence interval]: 1.40)
Adequate bowel prep was associated with higher TIIR (901% vs 76.7%), CIR (93.8% vs 86.0%) and shorter duration procedures (34 min vs 41 min)
a Presented as median (IQR) in minutes. b Includes only 967 combined esophagogastroduodenoscopy/ileocolonoscopy procedures without multiservice involvement. Bolded text and numbers reflect results demonstrating statistical significance
My take (borrowed in part from the authors): The authors state that “our findings suggest that a threshold of 40 annual procedures [ileocolonoscopies] is necessary to maintain high pediatric endoscopic quality.” While I agree that adequate procedural volume is helpful, there is a great deal of individual variation/ability. Particularly if the endoscopist has a lower procedural volume, metrics like ileal intubation rate can be useful to assure good quality.
Recently, Dr. Katja Karrento gave our group a great update on chronic nausea. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
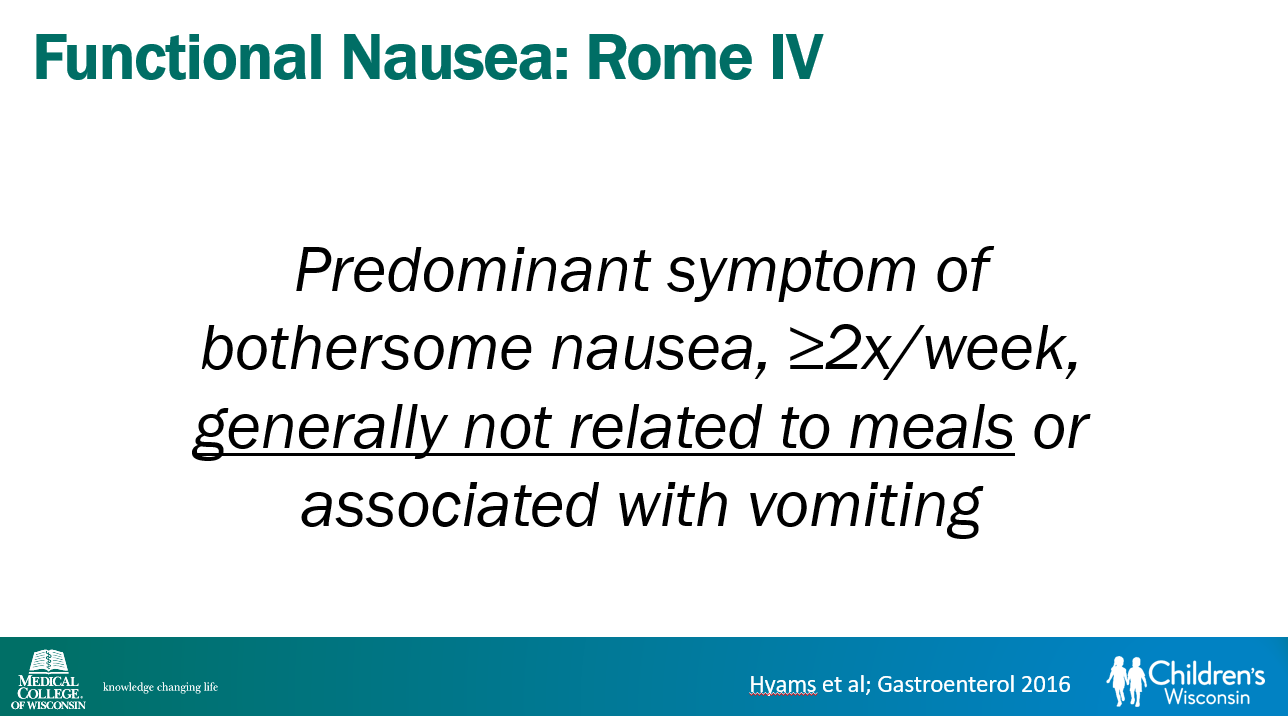
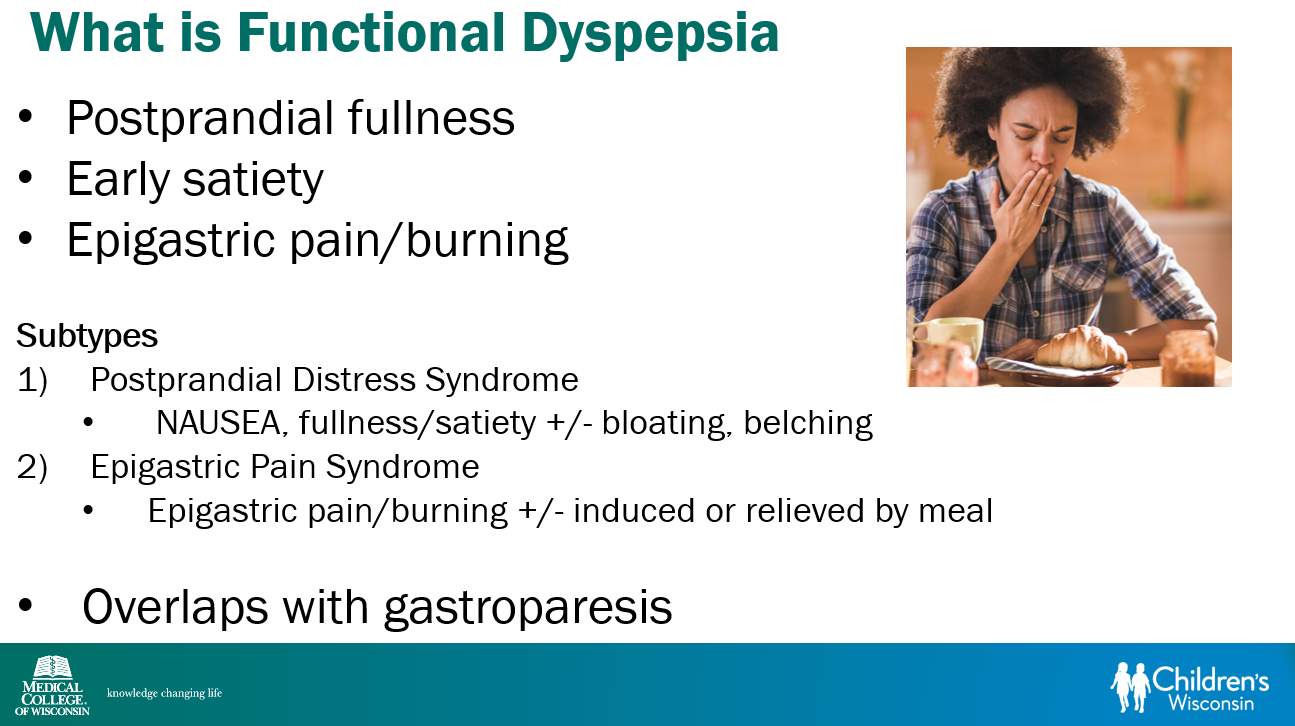
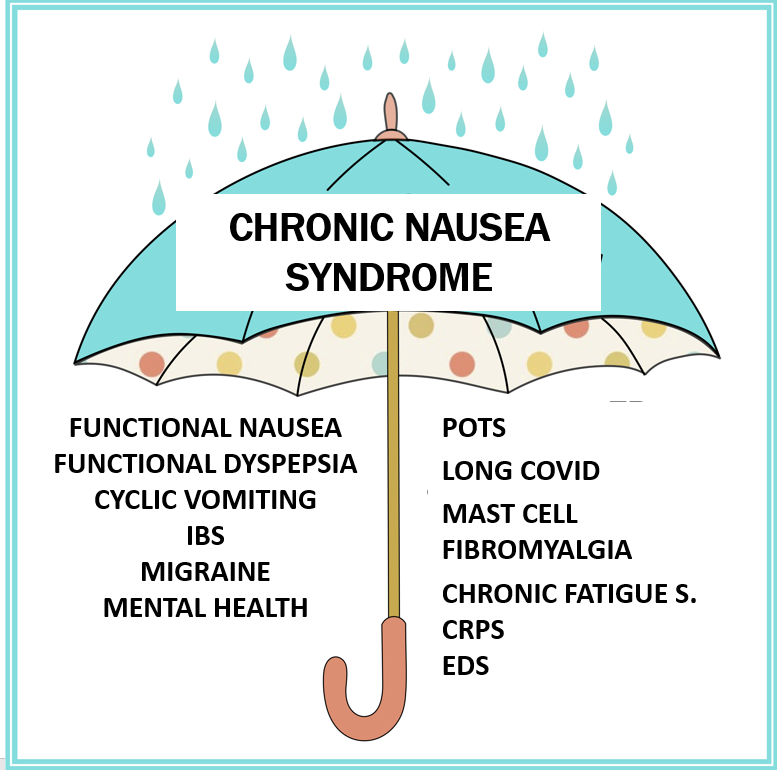
Recent research suggests that functional nausea overlaps with other DGBIs including functional dyspepsia, IBS and even gastroparesis
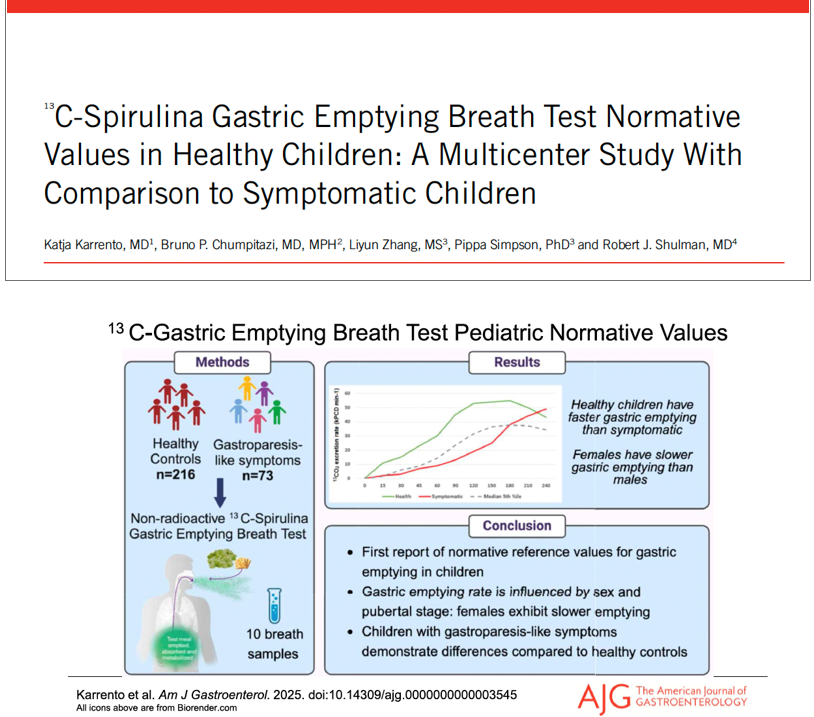
Delayed gastric emptying is found in a subset of patients who meet criteria for functional nausea (though there are limitations of GE studies)
Emerging research on use of C13-Spirulina breath test to assess gastric emptying
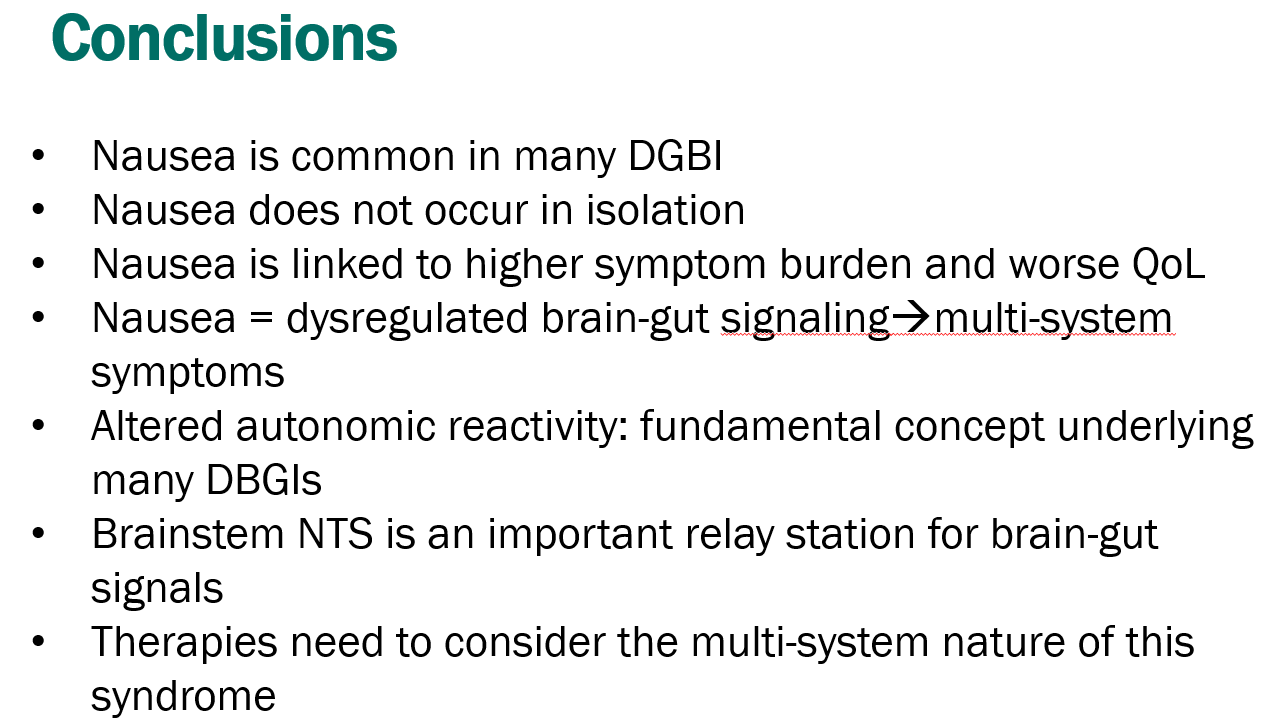
Nausea is linked to disability more than stomach pain
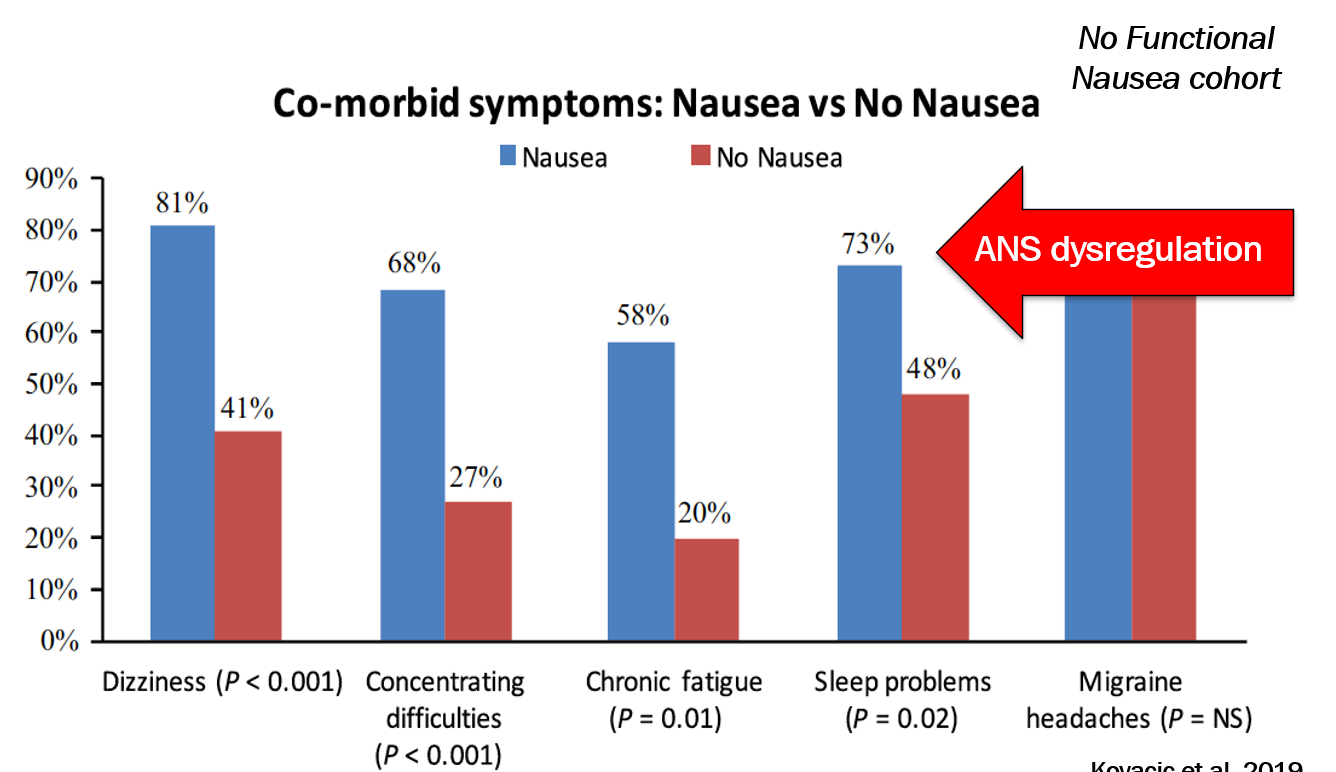
Among patients with DGBI, the presence of nausea was associated with increased comorbidities
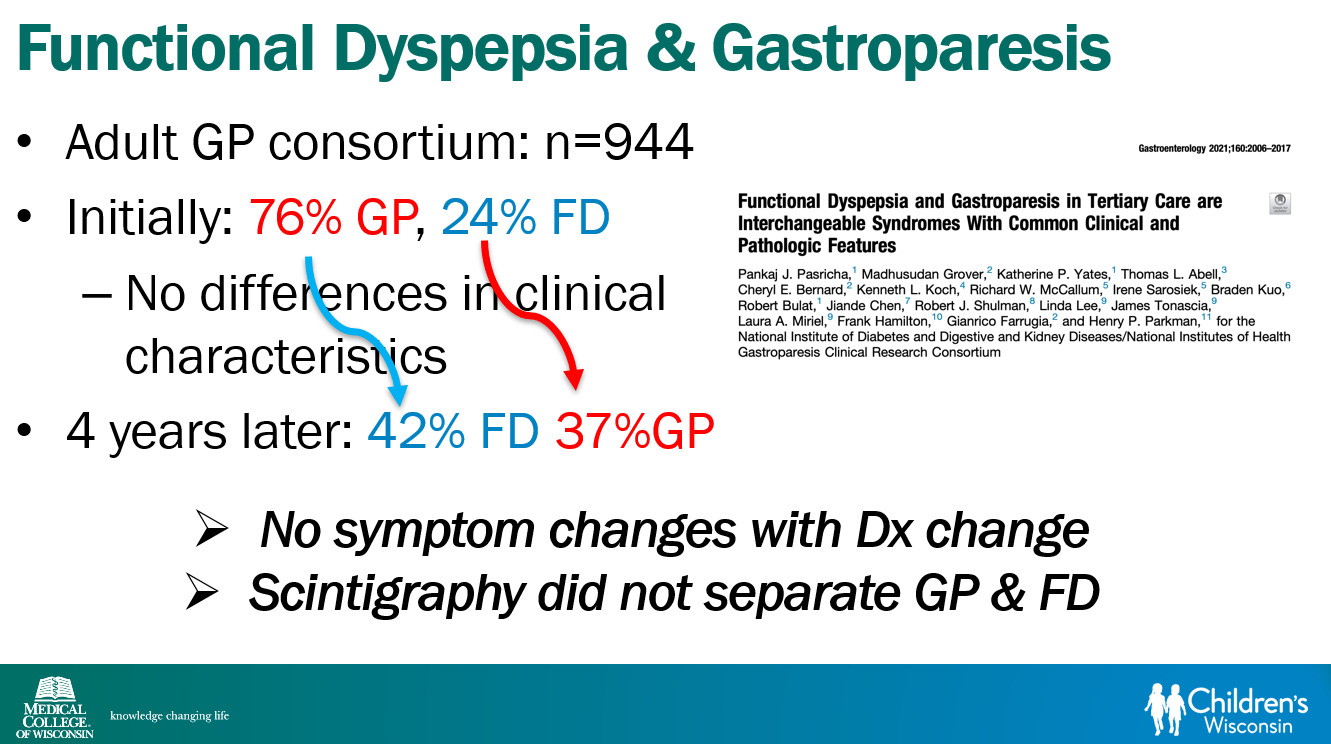
Functional dyspepsia and gastroparesis overlap and may be part of same disorder
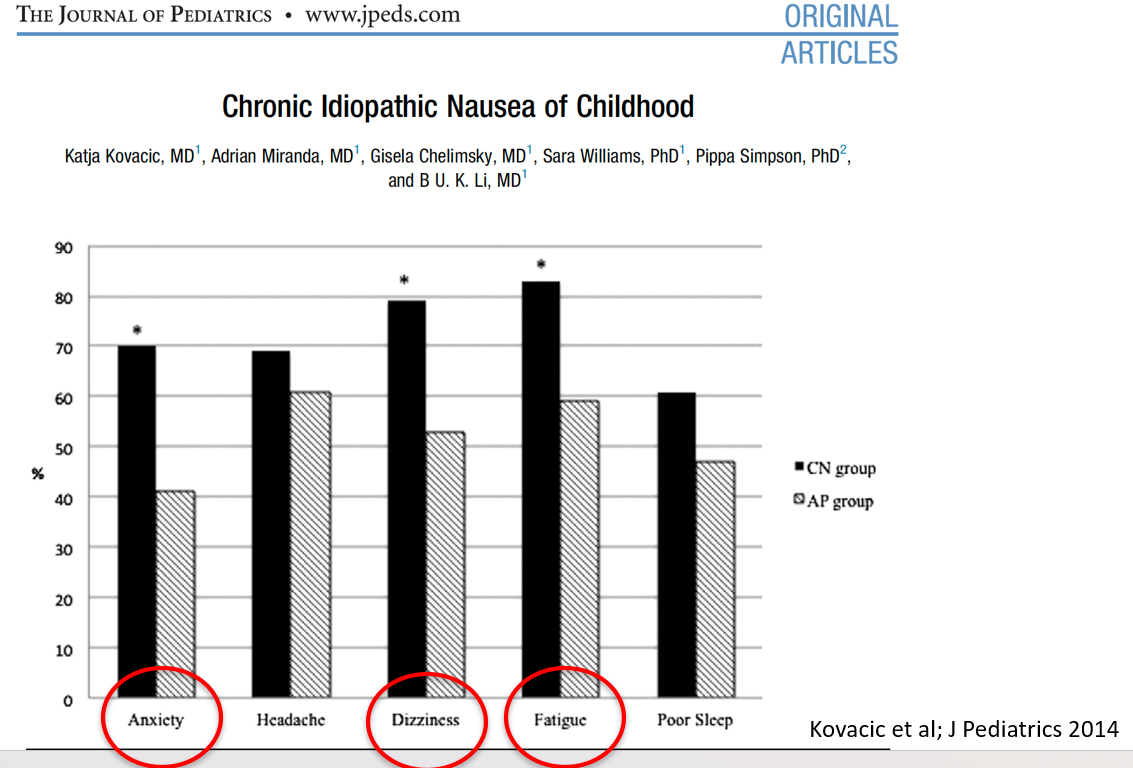
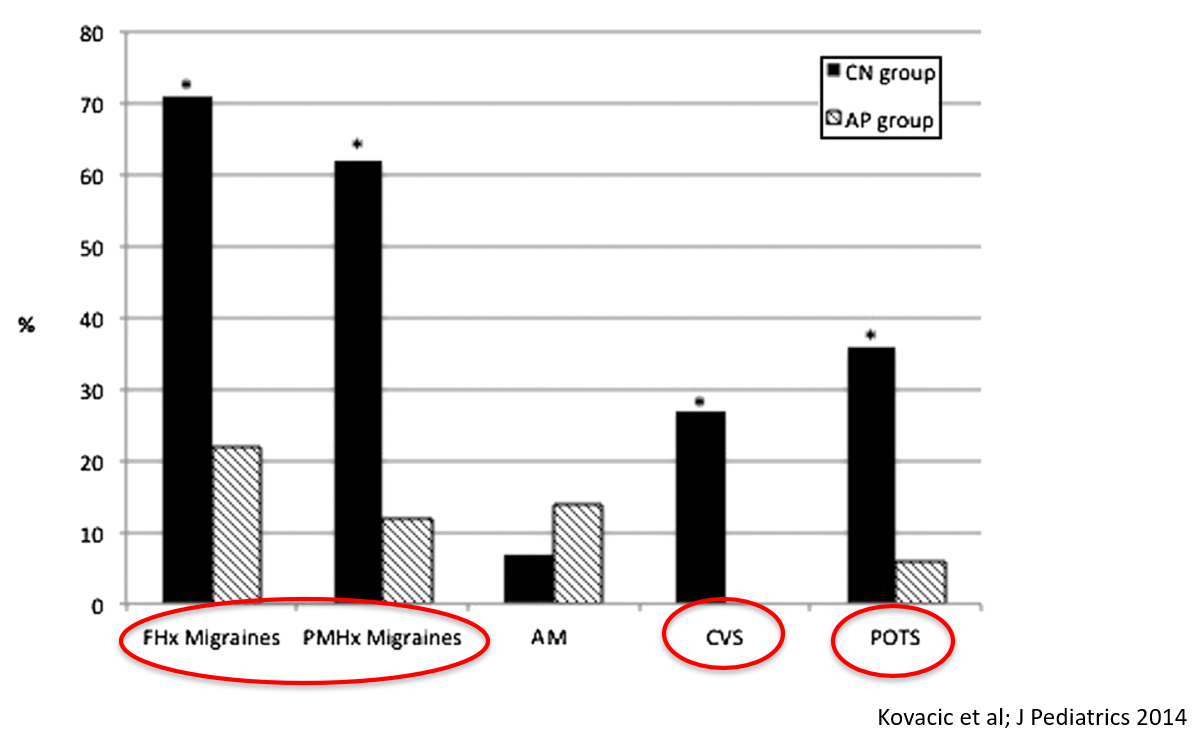
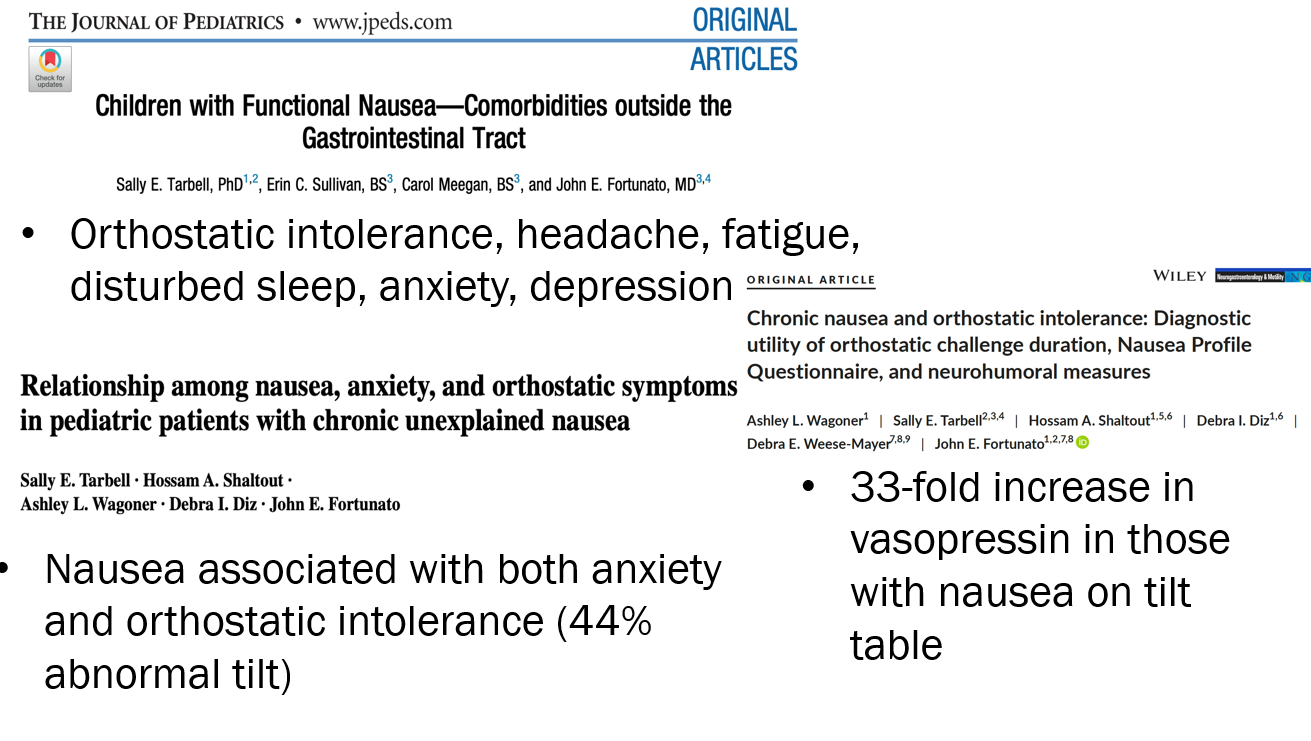
Nausea is associated with numerous extraintestinal comorbidities symptoms
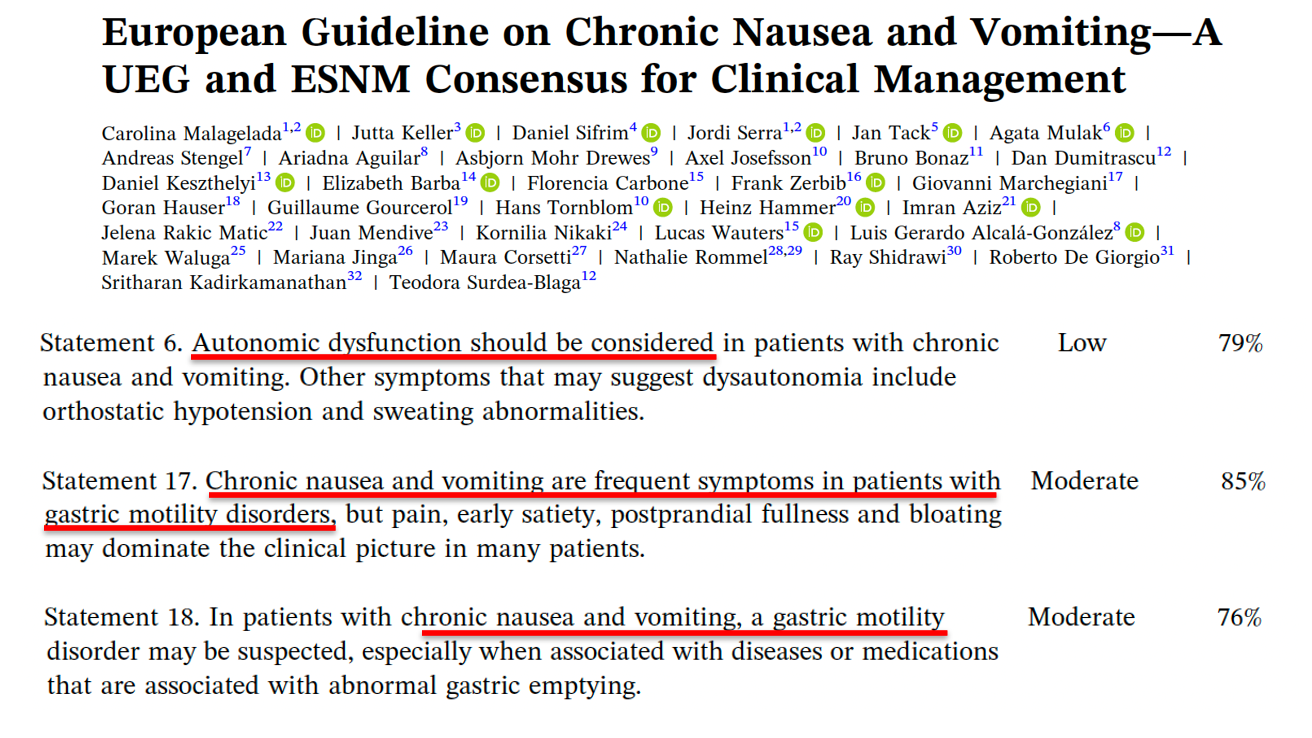
DGBIs are associated with abnormal autonomic nervous system signaling
Morning nausea, associated with being upright, is characteristic of dysautonomia. Other symptoms include ; palpitations, anxiety, sweating
POTS defined by increased HR >40 within 10 minutes with tilt test along with symptoms. In adults, increased HR>30 with symptoms.
A small (n=10) functional MRI study showed abnormal brain network organization in patients with nausea and orthostatic intolerance
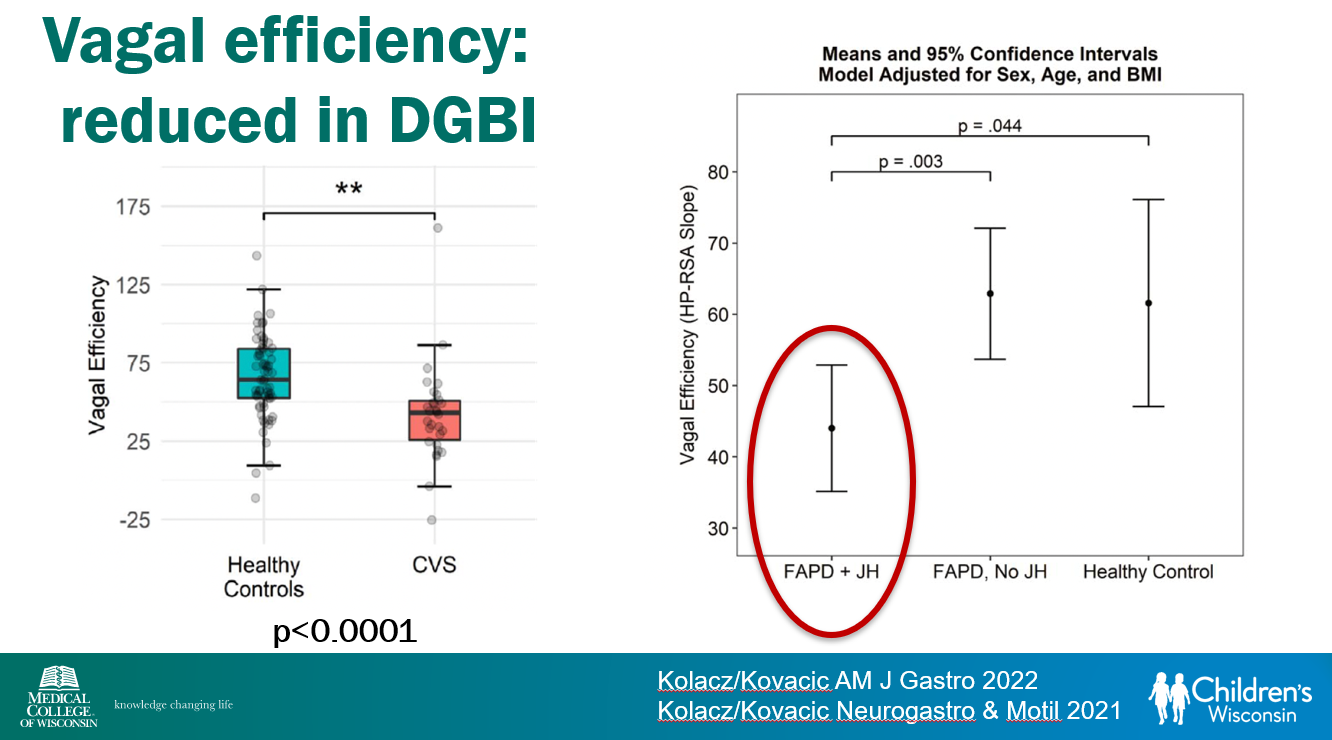
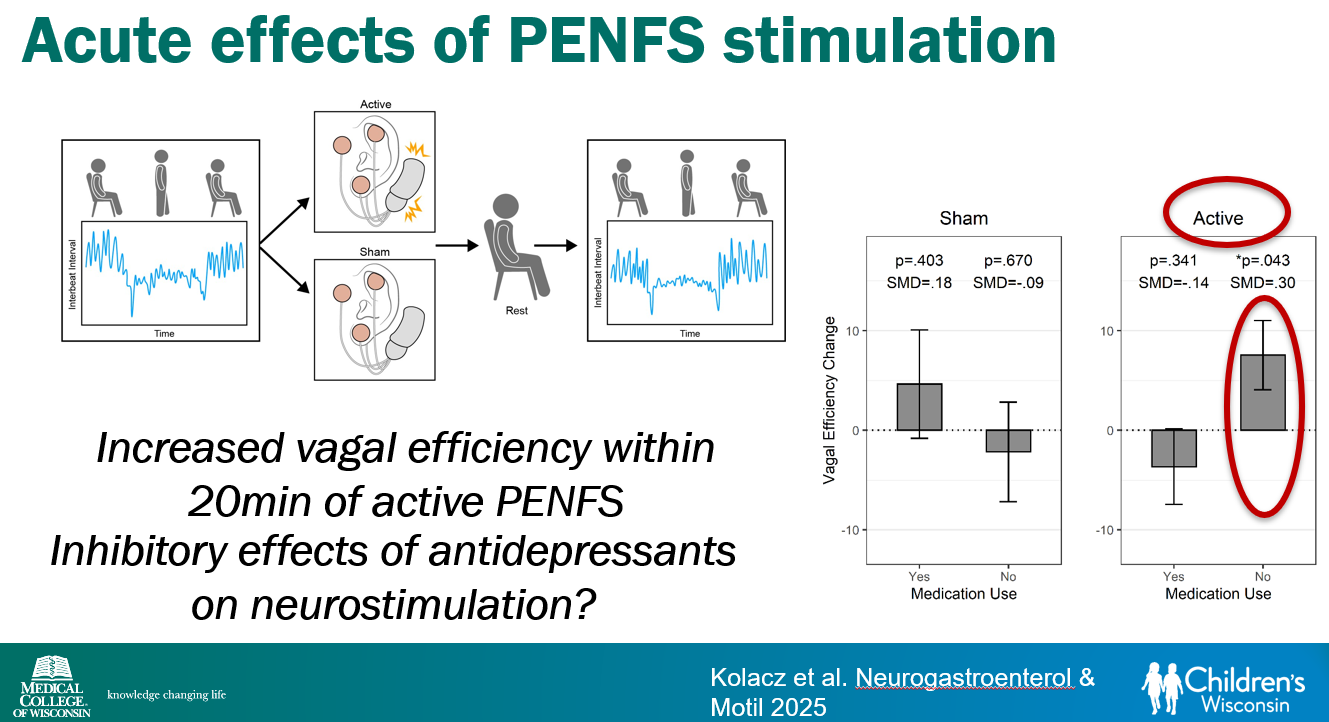
Vagal efficiency, which is decreased in subsets of DGBI, is a measure of the heart’s regulation of sympathetically-elicited tachycardia (or ‘..heart’s regulation of postural tachycardia’)
Cyclic vomiting is associated with autonomic nervous system alterations. In adolescence, the disorder often changes to chronic symptoms
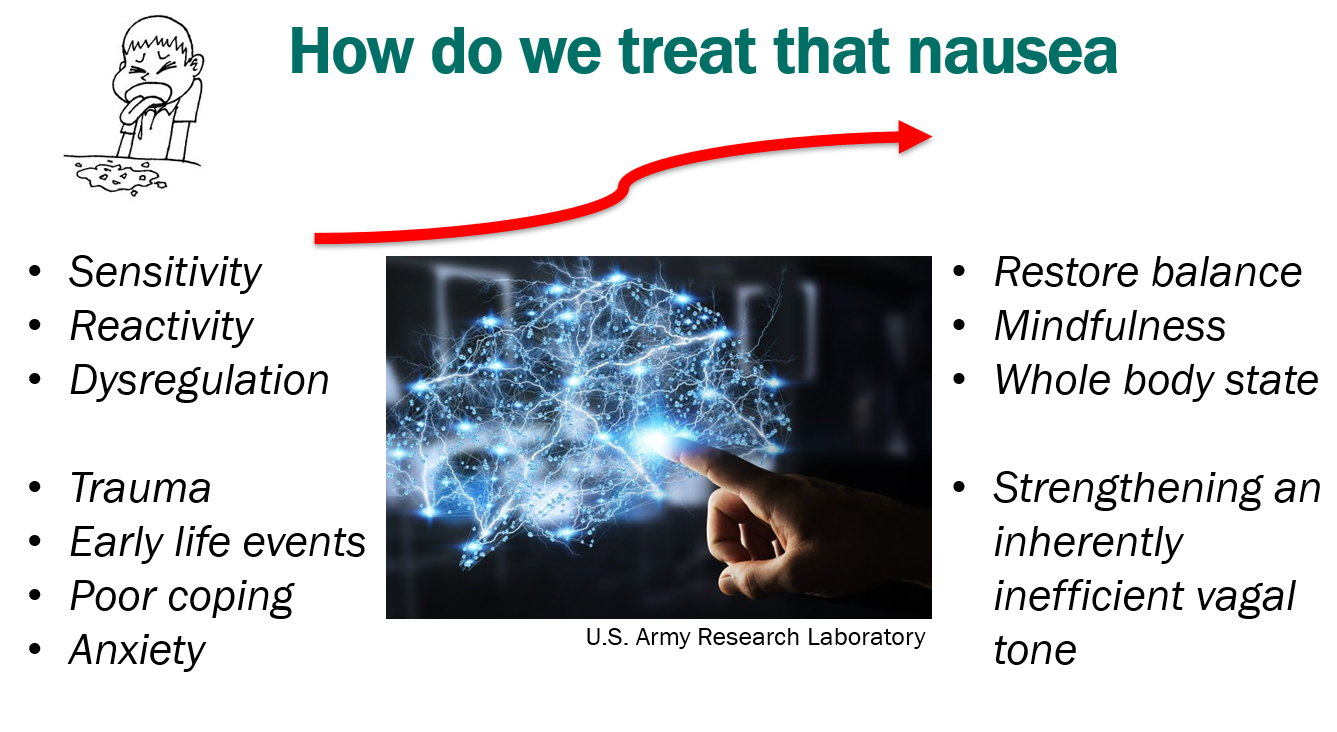
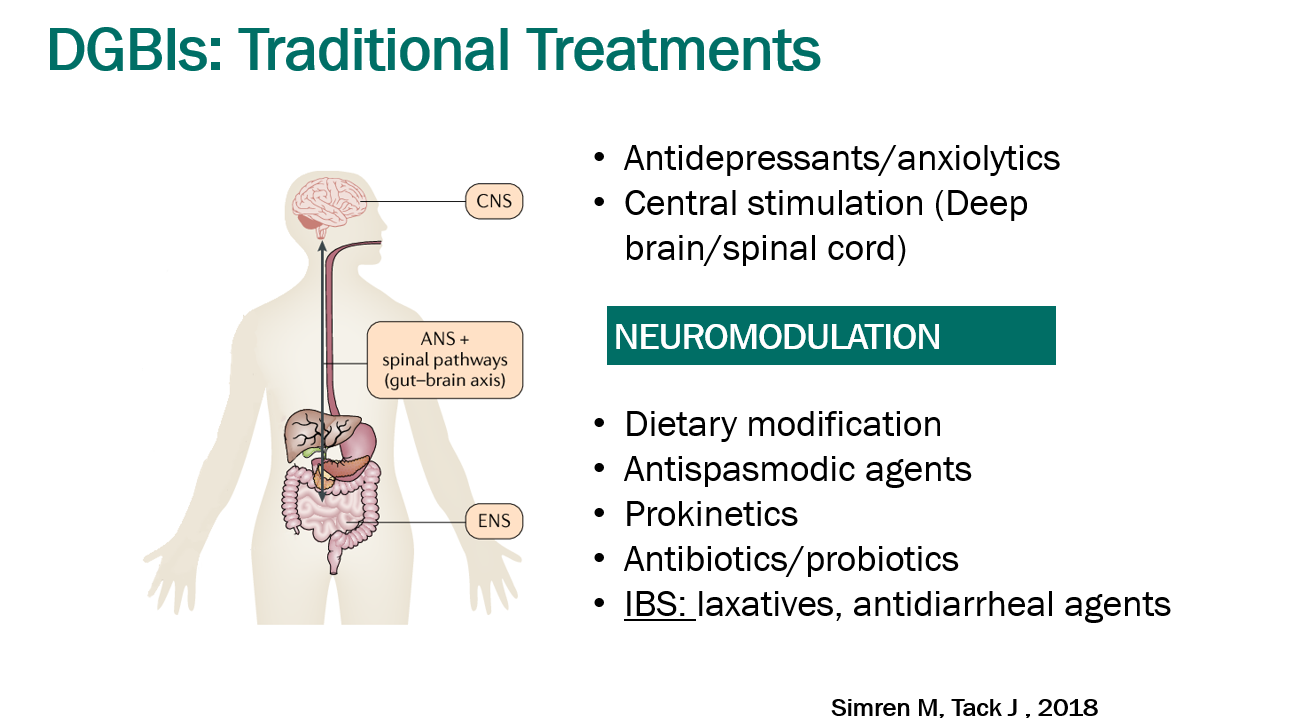
Treatment Advice: Explain early on the difficulty in treating these symptoms. Usually there is not a quick fix medicine. Lifestyle changes and coping are integral parts. Neuromodulation is likely more effective than other approaches
Dr. Karrento recommends The Dysautonomia Project to doctors and patients
Exercise is helpful for DGBIs
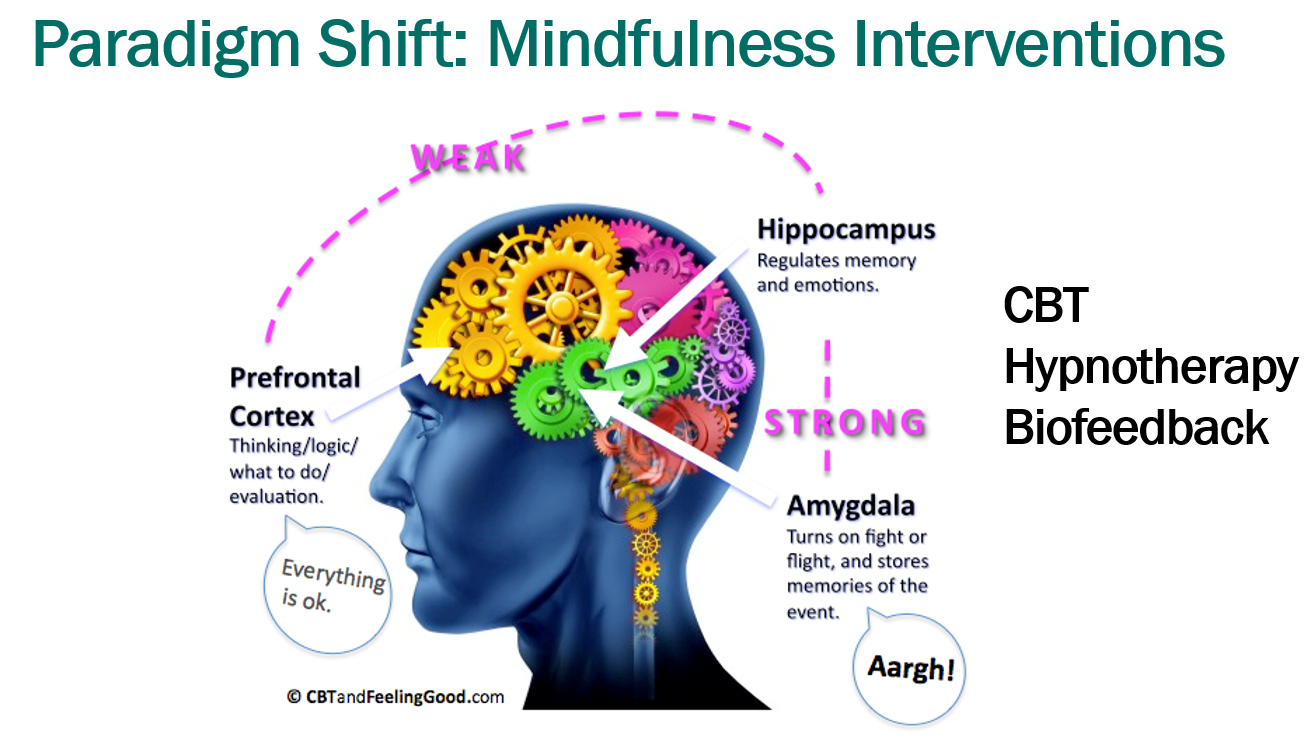
Mindfulness training may help: CBT, Hypnotherapy, Biofeedback
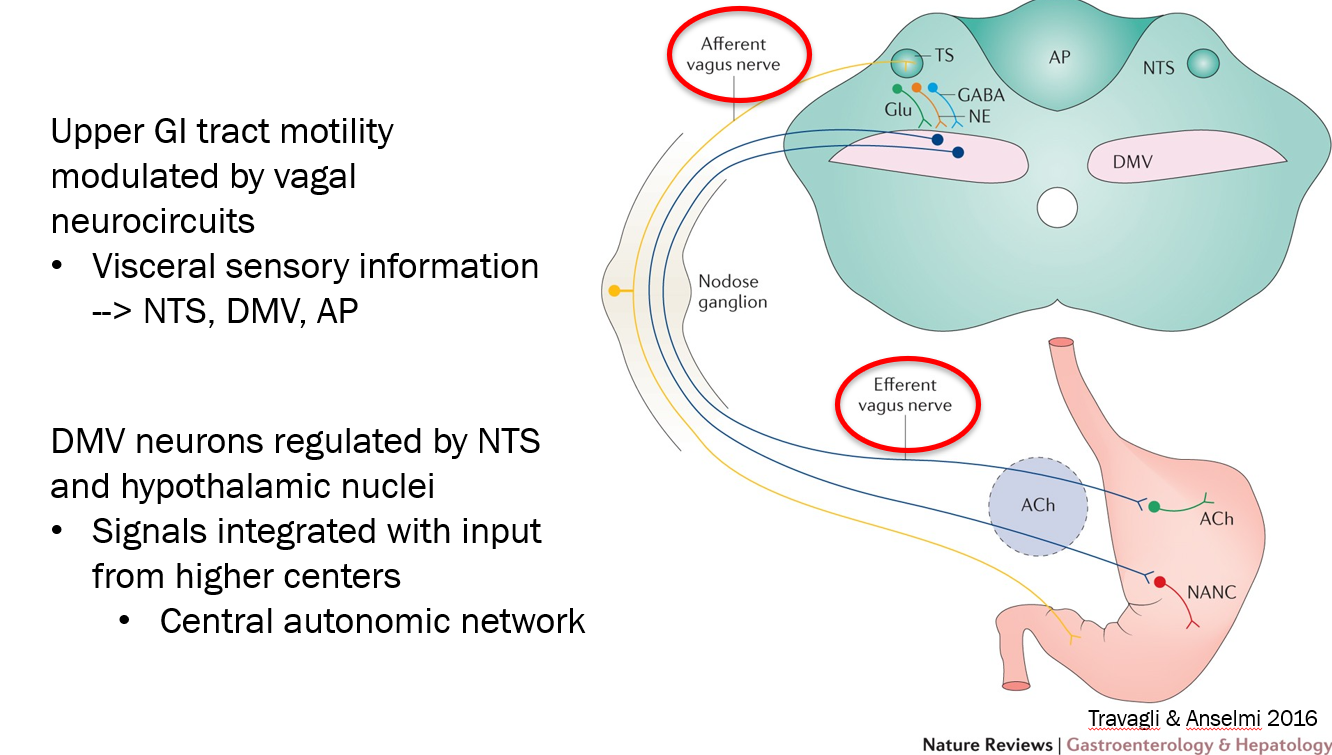
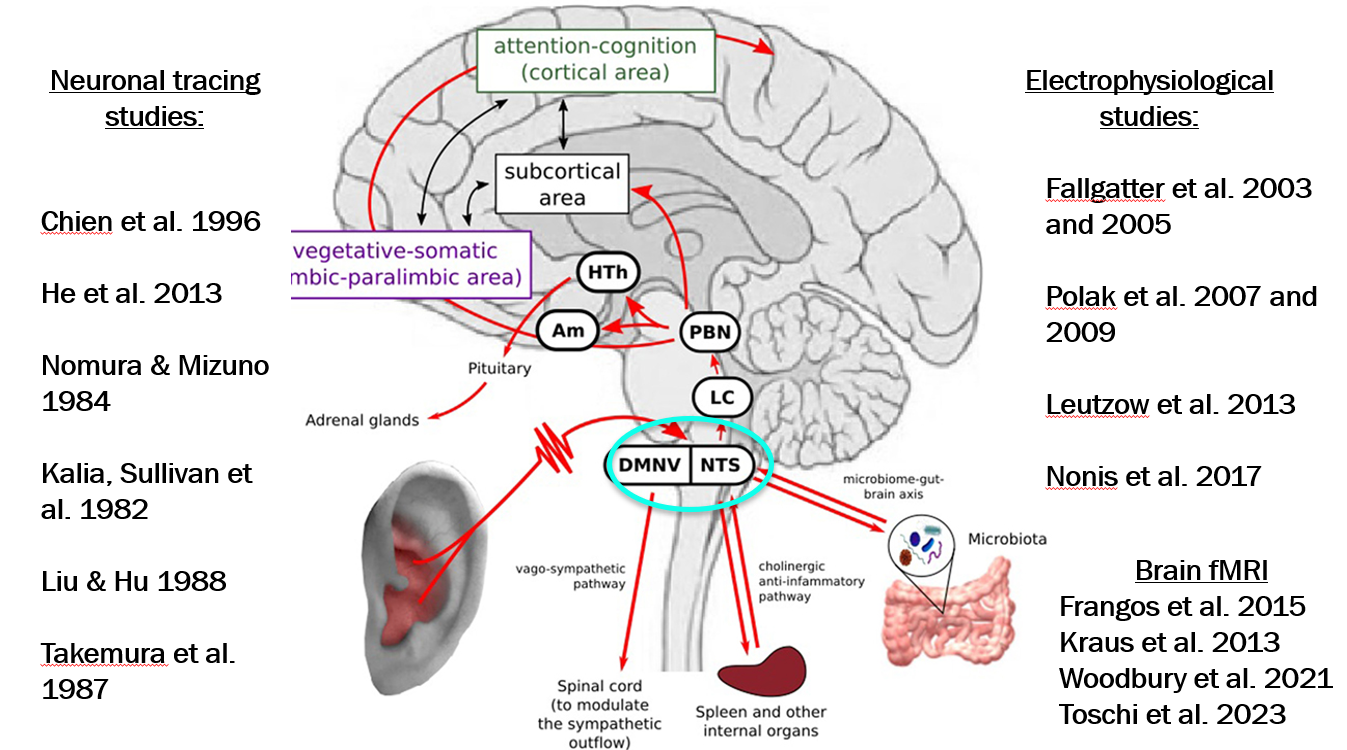
The auricular branch of the vagus projects to brainstem NTS. 95% of vagal afferent projections end up in NTS which in turn is directly and indirectly connected to a network of higher brain regions of the central autonomic network
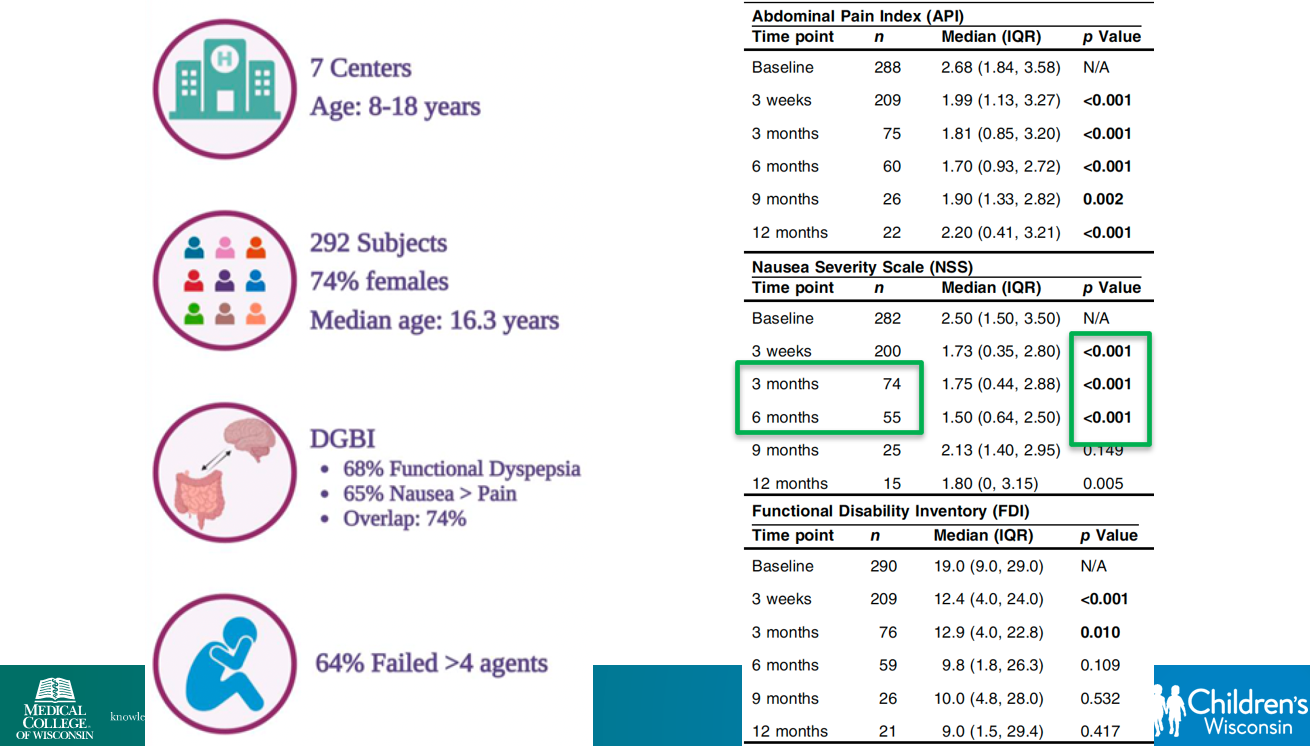
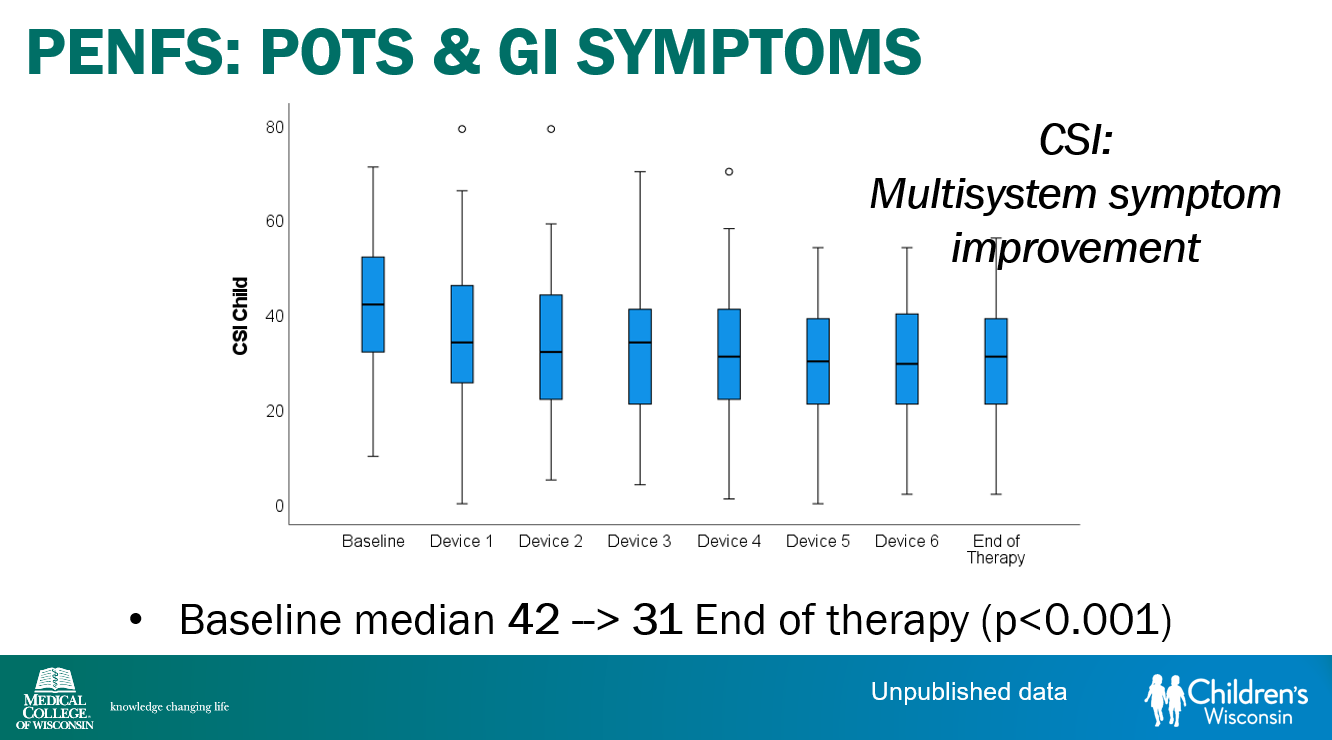
Percutaneous electrical nerve field stimulation (PENFS) can be useful in functional nausea and many DGBIs
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
CDC Study: “From late August 2024 to early September 2025, the vaccines reduced the risk of Covid-related emergency room and urgent care visits by 76% among children ages 9 months to 4 years, and by 56% among children ages 5-17, according to the study”
Citation: Irving SA, Rowley EA, Chickery S, et al. Effectiveness of 2024–2025 COVID-19 Vaccines in Children in the United States — VISION, August 29, 2024–September 2, 2025. MMWR Morb Mortal Wkly Rep 2025;74:607–614. DOI: http://dx.doi.org/10.15585/mmwr.mm7440a1
Between the end of February and mid-August, funding ceased for 383 studies that were testing treatments for conditions including cancer, heart disease and brain disease. The cuts disproportionately impacted efforts to tackle infectious diseases like the flu, pneumonia and COVID-19, researchers found…
More broadly, the lost research harms patients who could have benefited from a possible new treatment, researchers said in the report published Monday in the journal JAMA Internal Medicine…
“The whole purpose of these clinical trials is to generate evidence on what works and doesn’t work in medicine,” said study co-author Anupam B. Jena with Harvard Medical School. Researchers counted 11,008 NIH-funded studies during the study period. Of those, 1 in 30 lost funding.
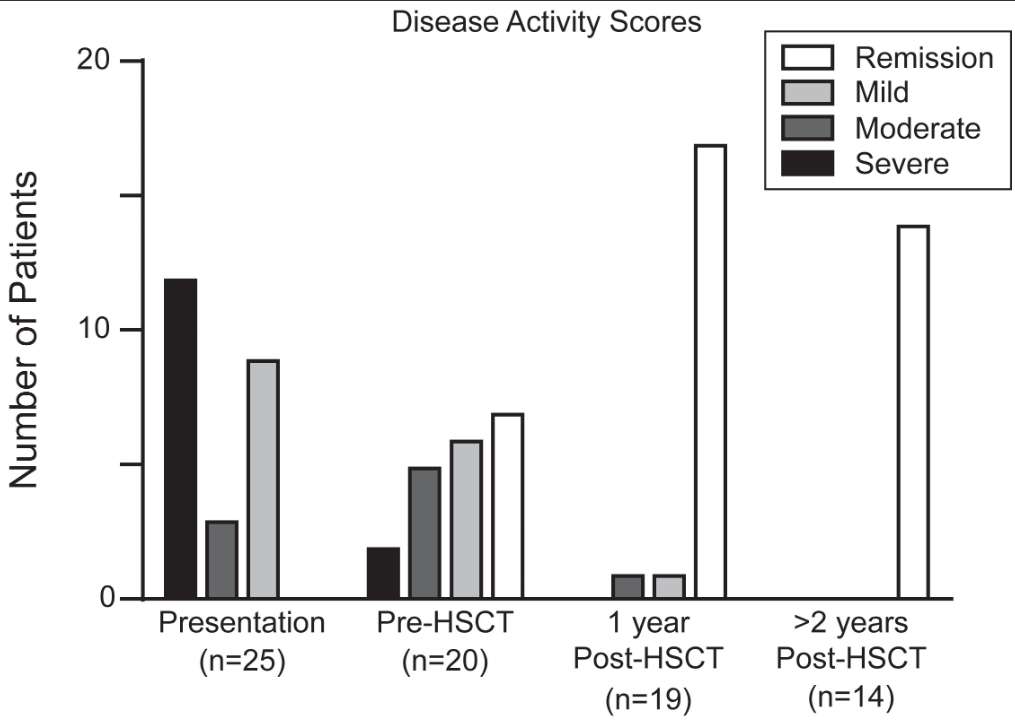
This was a retrospective single-center (CHOP) study of 25 children with monogenic IBD who underwent Hematopoietic Stem Cell Transplant (HSCT) (2012-2022).
Key findings:
Seventy-two percent of patients had Crohn’s Disease, and 28% were classified as IBD-unspecified. Ninety-two percent of patients had VEO-IBD, 56% presenting under age 1
At most recent follow-up, 92% of patients achieved sustained medication-free remission of IBD and 60% with prior ostomy underwent re-anastomosis. There was 100% survival at a median follow-up of 3 years
There was significant improvement in growth, hospital days, and severe infections
Disease activity scores at the time of IBD presentation, immediately prior to transplant, 1-year post-transplant, and at most recent follow up if ≥2 years since transplant.
Discussion points:
“Delay of HSCT with the goal of obtaining remission of IBD prior to transplant may prove to be determinantal, as outcomes of HSCT are in general improved for younger patients,20 and medical remission is often unattainable for more severe forms of monogenic IBD. Within our cohort, 32% of patients had moderate or severe disease at the time of transplant despite medical optimization. None of these patients developed intestinal GVHD, which was a rare event in our total cohort”
“HSCT is not without risk, and complications occurred in our cohort, at rates typical of other IEI cohorts”
“The selection of patients who would benefit from HSCT requires multidisciplinary discussion.”
With regard to patient selection, one item that was not included in the discussion was the one patient excluded from their analysis who had a TTC7A gene defect. In the results section, it was explained that the patient with “TTC7A was subsequently excluded as transplant was performed for the indication of SCID alone, rather than treatment of intestinal disease.” More discussion on this point is merited as many centers would NOT have a patient with TTC7A undergo HCST specifically because it cannot correct the underlying bowel disease.
Also, it was noted that one patient with CTLA4 deficiency had undergone HSCT prior to the discovery of the genetic defect. With the more widespread use of genetic testing available now, this discovery may have obviated the need for HSCT as treatment with abatacept is typically effective.
My take: Overall, the authors present impressive results for HSCT for monogenic IBD and strengthen the need for genetic testing in those with early onset disease and those refractory to treatment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
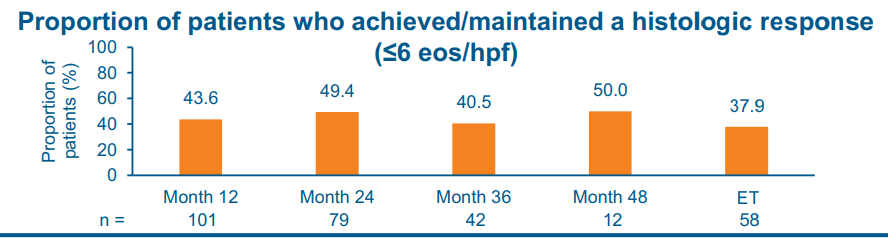
The study by Dellon et al was a 4-year, phase 3, open-label study in patients with EoE who completed up to 52 weeks of BOS therapy (Budesonide oral suspension 2 mg 2/day) in 2 preceding phase 3 studies.
Key findings:
At month 48 of treatment, 50.0% and 58.3% of patients achieved/maintained a histologic response (< or =6 and <15 eosinophils per high-power field, respectively)
Safety:
Treatment-emergent adverse events (TEAEs) occurred in 76.3% of patients; most were mild/moderate in severity and unrelated to study drug.
The most frequently reported BOS-related TEAEs included abnormal adrenocorticotropic hormone stimulation test results (8.4%, 11/131; number of events [m] [ 12) and adrenal insufficiency (2.3%, 3/131; m [ 3). Esophageal candidiasis occurred in 3.1% of patients (4/131)
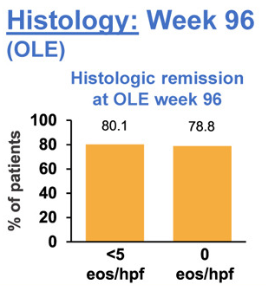
The study by Biedermann et al explored the use of an orodipsersible tablet for EoE up to 3 years in patients who achieved remission during a 12-week induction. This tablet is not available in the U.S.
Key findings:
At week 96, 80.1% of patients were in histologic remission, defined as peak eosinophils per high-power field of <5, at week 96 vs 91.8% at open label extension baseline
No new safety concerns were observed across 96 weeks of treatment. Suspected symptomatic candidiasis occurred at similar rates to prior BOT studies and was predominantly mild and resolved with treatment
My take: The pharmaceutical budesonide suspension, Eohilia, is labelled by the FDA for use as a 12 week treatment course. Since EoE is a chronic disease, 12 weeks is insufficient. These long-term studies provide data that may address this shortcoming.
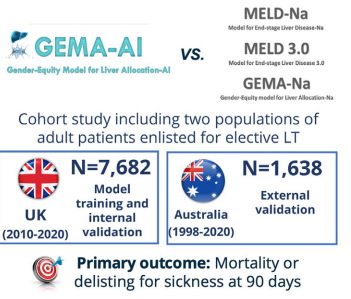
Background: “The current gold standard for ranking patients in the waiting list according to their mortality risk is the Model for End-Stage Liver Disease corrected by serum sodium (MELD-Na), which combines 4 serum analytic and objective parameters, namely bilirubin, international normalized ratio (INR), creatinine, and sodium…2“
“The Model for End-Stage Liver Disease (MELD) 3.0 was developed and internally validated in the United States,4 and the gender-equity model for liver allocation corrected by serum sodium (GEMA-Na) was trained and internally validated in the United Kingdom and externally validated in Australia.5… GEMA-Na was associated with a more pronounced discrimination benefit than MELD 3.0, probably owing to the replacement of serum creatinine with the Royal Free Hospital cirrhosis glomerular filtration rate (RFH-GFR)6 in the formula.5“
Methods:
Key findings:
GEMA-AI made more accurate predictions of waiting list outcomes than the currently available models, and could alleviate gender disparities for accessing LT
Discussion Points:
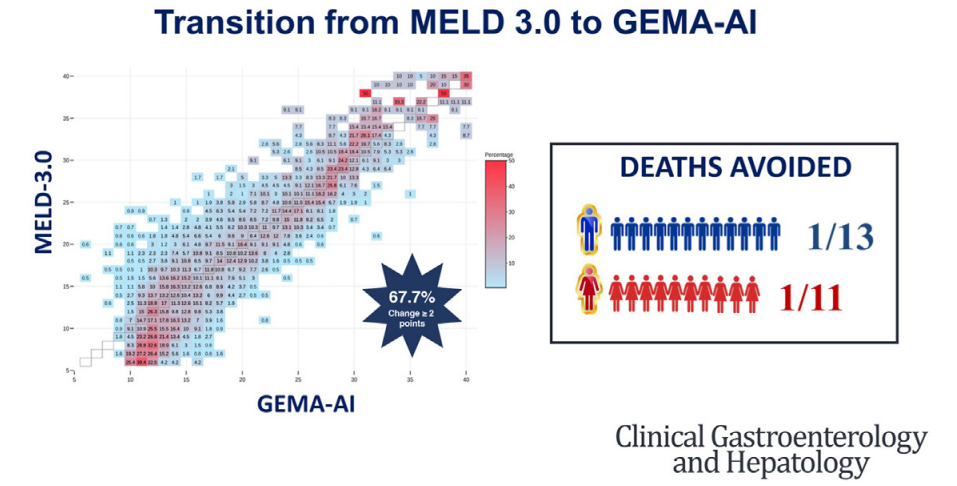
The components of the current scores available for waiting list prioritization provide objective and reproducible information…which in turn are associated with the probability of mortality or clinical deterioration resulting in transplant unsuitability.18 However, this relationship is nonlinear…at a certain point, for the highest values typically found in the sickest patients, the relationship with the outcome risk becomes exponential.5 …GEMA-AI was the only adequately calibrated model and showed the greatest advantage on discrimination”
An “advantage of nonlinear methodologies, and particularly of ANNs [artificial neural network], is their ability to identify patterns of combinations of values that are associated with an increased risk of death or delisting due to clinical worsening. While linear models give a fixed weight to each variable irrespective of its value or the value of other variables in the model, ANNs could capture specific combinations to modulate the weighting.19“
My take: In the movie, iRobot, Detective Spooner instructs the robot: “Sonny, save Calvin.” While things worked out in the movie, it turns out that the robot would usually make a better decision. This study shows that AI has the potential to reduce waiting list mortality by taking advantage of weighing non-linear variables.
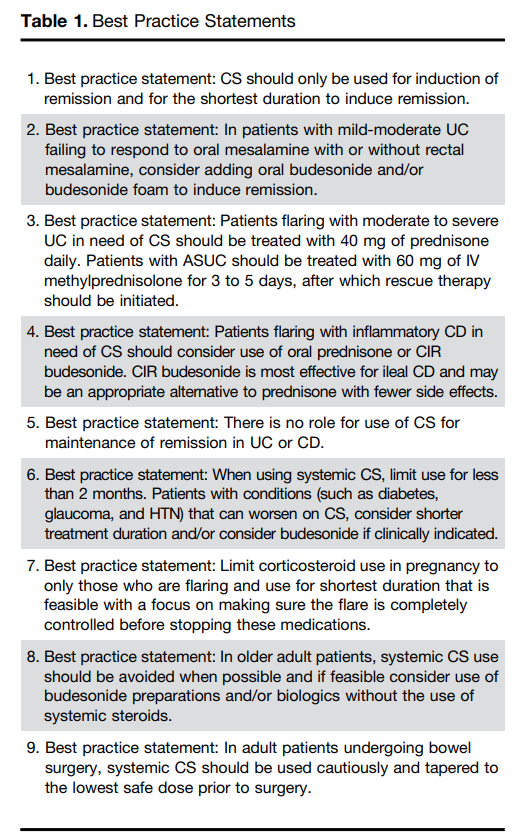
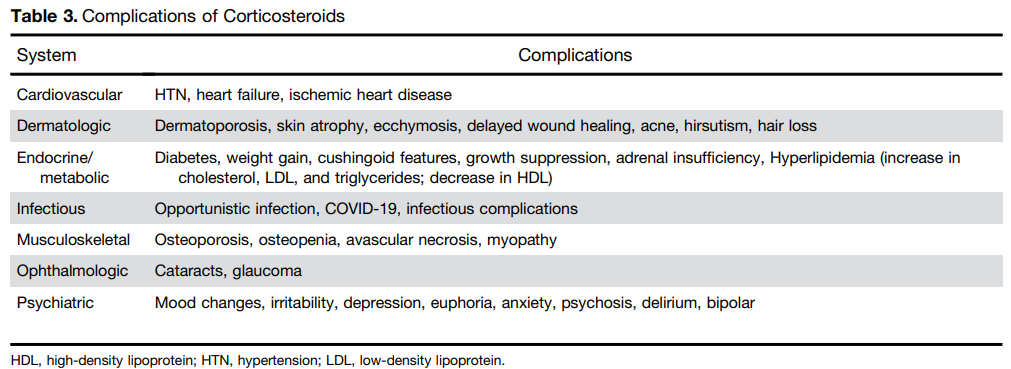
Steroids are commonly used and misused for inflammatory bowel disease. This article reviews best practices, steroid formulations/dosing, and potential complications.
For moderate to severe ulcerative colitis (in adults), the authors recommend treatment with 40 mg of prednisone daily. Patients with ASUC (acute severe ulcerative colitis) should be treated with 60 mg of IV methylprednisolone for 3 to 5 days, after which rescue therapy should be initiated
Use of budesonide is recommended as an option for many clinical situations to minimize steroid adverse effects. These situations include mild-moderate UC failing to respond to mesalamine, ileal CD and older patients
Postoperative complications: “In the postoperative period, patients treated with CS had a higher risk of both infectious complications (aOR, 3.69; 95% CI, 1.24–10.97) and major infectious complications (aOR, 5.54; 95% CI, 1.12–27.26) [Abrerra et al].135 Subramanian pooled data from 7 studies showing that preoperative CS use is associated with increased postoperative complications (OR, 1.41; 95% CI, 1.07–1.87) as well as infectious complications.
The authors note that corticosteroids “remain widely available and are an effective short-term option for induction of remission in patients with active UC or inflammatory CD. However, their well-described and significant safety profile warrants proactive strategies to limit their use through non-systemic formulations, short-term exposures, steroid-sparing maintenance options, and most recently, complete steroid avoidance strategies.”
My take: Continuing steroids when they are not effective prior to potential surgery (eg. ASUC) remains a frequent problem. Sometimes, it is difficult to know it they are helping some.




06160-8/asset/17e8b821-1efa-4c66-adce-db270f9e7629/main.assets/fx1_lrg.jpg){kind=link}