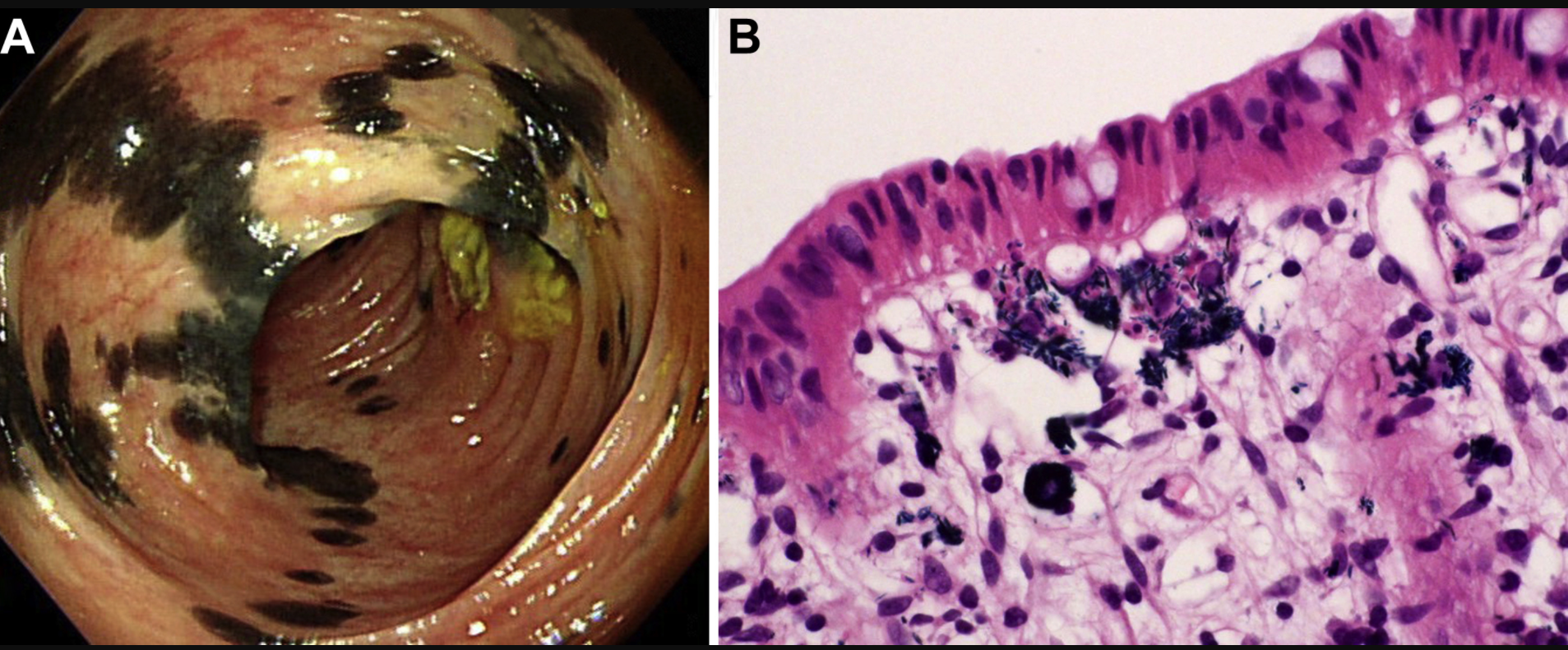
The image below is from a 57 yo woman with Crohn’s disease who was taking a supplement, indigo naturalis (Qing-Dai). “Higher magnification disclosed bluish, needle-like crystals in the cytoplasm of these histiocytes. In light of the presence of pigment-laden histiocytes, we called the lesions indigo naturalis-related pseudomelanosis. Unlike melanosis coli, which typically shows continuous homogeneous brown or black discoloration of colon mucosa (snake-skin appearance or starry sky appearance), indigo naturalis-related pseudomelanosis exhibits a haphazard distribution of black discoloration reminiscent of the skin markings of Holstein Friesian cattle…It remains to be seen whether deposition of indigo naturalis has any long-term adverse effect, although histologically the mucosa with indigo deposition was not accompanied by significant inflammatory activity.”
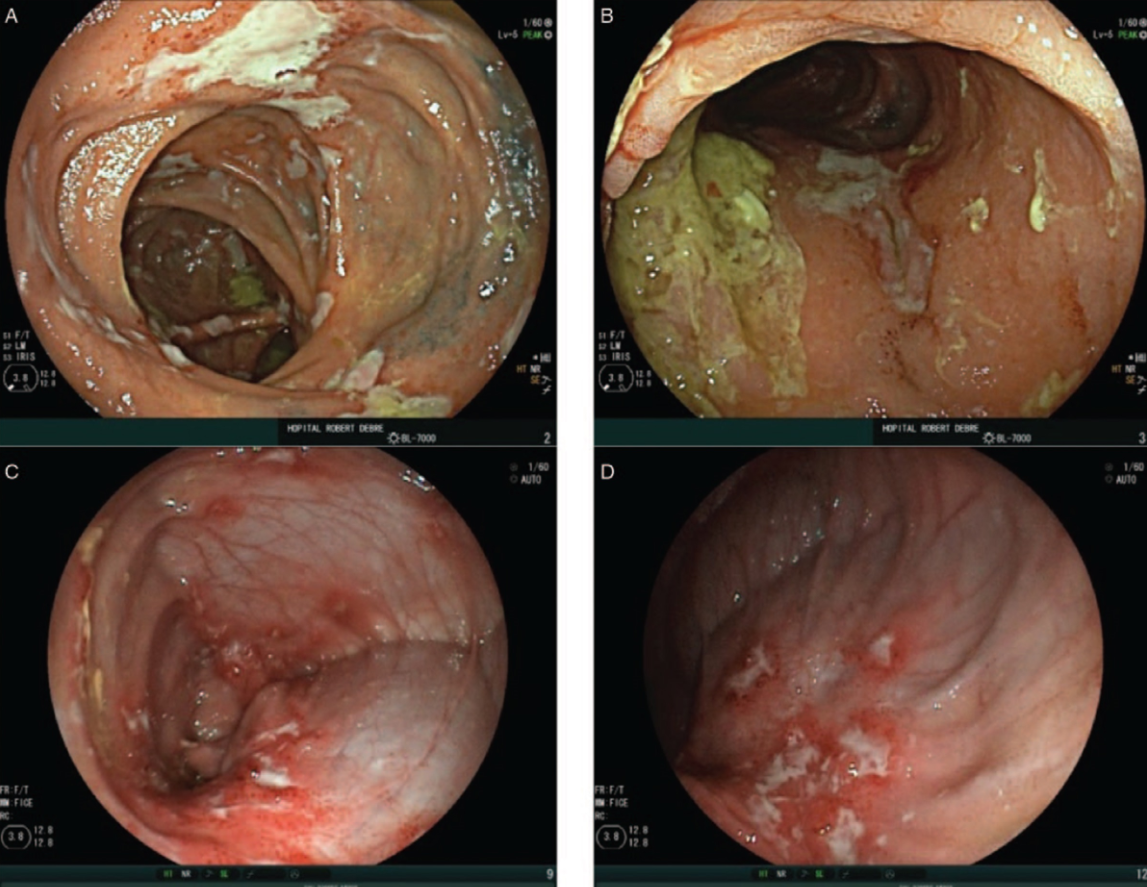
This survey study with 51 children described the etiology and treatment of perianastomic ulcerations (PAU).
Key findings:
Most common initial etiologies: necrotizing enterocolitis (n = 20) or Hirschsprung disease (n = 11)
Median onset of symptoms: 39 [22–106] months after surgery
Clinical features: Anemia was the most prevalent symptom followed by diarrhea, abdominal pain, bloating, and failure to thrive. Hypoalbuminemia, elevated CRP, and fecal calprotectin were common
Deep ulcerations were found in 59% of patients usually proximally to the anastomosis (68%)
Treatments: treatments reported to be the most effective included exclusive enteral nutrition (31/35, 88%), redo anastomosis (18/22, 82%), and alternate antibiotic treatment (37/64, 58%). The authors note that despite similarity to Crohn’s disease, there was a lack of response to immunosuppressors and anti-TNF therapies
From JPGN twitter feed. Figure 2 in article showing examples of ileocolonic ulcerations
Turns out cows can be potty trained as easily as toddlers… 11 out of 16 cows learned to use the “MooLoo” when they had to go…And it took only 15 days to train the young calves.
[Results were] published Monday in the journal Current Biology...Massive amounts of urine waste is a serious environmental issue,…A single cow can produce about 8 gallons (30 liters) of urine a day… toilet training animals makes it easier to manage waste products and reduce greenhouse gas emissions
Theresearchers mimicked a toddler’s training, putting the cows in the special pen, waiting until they urinated and then giving them a reward: a sweet liquid of mostly molasses… If the cows urinated outside the MooLoo after the initial training, they got a squirt of cold water…
The biggest environmental problem for livestock, though, is the heat-trapping gas methane they emit in belches and flatulence, a significant source of global warming. The cows can’t be trained not to belch or fart, Matthews said: “They would blow up.”
Methods: The study population from consisted of 3 groups—50 newly diagnosed CD children (group 1), 50 previously diagnosed CD children who were on gluten free diet (GFD) >3 months (group 2), and 100 age and gender matched healthy controls (group 3).
Key findings:
Positive anti-HBs response was found in 46% in newly diagnosed CD children, 60% in CD children on GFD, and 83% in healthy controls (P < 0.001)
Ongoing gluten intake has significant impact on protective immune response to Hepatitis B vaccine
44 out of 45 (97.77%) nonresponders from CD group seroconverted after a single booster dose
My take: Check Hep B immune response in patients with celiac disease.
Source: CHOA COVID-19 Webpage The graph below depicts the number of patients hospitalized at CHOA (Egleston and Scottish Rite) during 2021, currently 8.7% of admissions are due to COVID-19.
Here’s a link showing the U.S Vaccination Rate Compared to Other Countries (from Eric Topol): U.S. Fallen to #45 in World with Percentage of Population with 1 or More Doses of Vaccine
J Dailey et al. Inflammatory Bowel Diseases, izab207, https://doi.org/10.1093/ibd/izab207 Open Access: Antibody Responses to SARS-CoV-2 After Infection or Vaccination in Children and Young Adults With Inflammatory Bowel Disease This article showed that there was a “lower and less durable SARS-CoV-2 S-RBD IgG response to natural infection in IBD patients receiving biologics [which] puts them at risk of reinfection. The robust response to immunization is likely protective.” Also, “hospitalized pediatric patients with PCR documented SARS-CoV-2 infection, S-RBD IgG antibody levels were significantly lower in the IBD cohort and by 6 months post infection most patients lacked neutralizing antibody.” This study provides a strong rationale for vaccination, especially in our IBD patients. (Thanks to Stan Cohen for this reference)
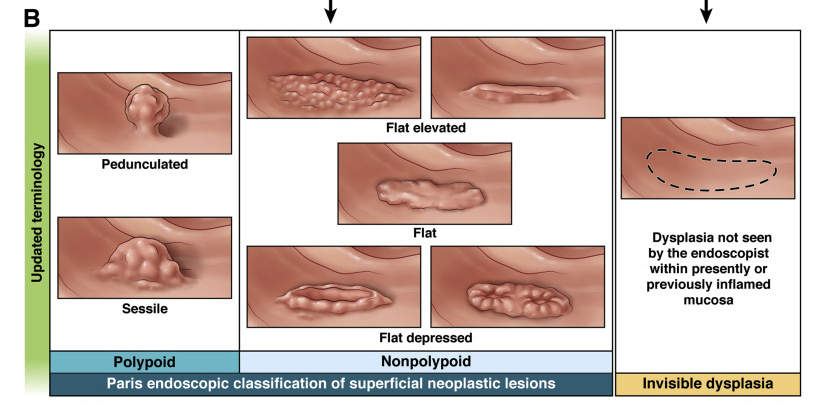
Best Practice Advice 1: Precancerous colorectal lesions in inflammatory bowel disease should be described as either polypoid (≥2.5 mm tall), nonpolypoid (<2.5 mm), or invisible (detected on nontargeted biopsy), using a modified Paris Classification. The older terms dysplasia-associated lesion or mass, adenoma-like mass, and flat dysplasia (when referring to dysplasia detected in nontargeted biopsies) should be abandoned.
Best Practice Advice 3: Initial colonoscopy screening for dysplasia should be performed at 8–10 years after disease diagnosis in all people with colonic inflammatory bowel disease, and immediately on diagnosis of primary sclerosing cholangitis. Staging biopsies should be taken from multiple colonic segments to assess histologic disease activity and extent and to help guide future surveillance intervals.
Best Practice Advice 8: Extensive nontargeted biopsies (roughly 4 adequately spaced biopsies every 10 cm) should be taken from flat colorectal mucosa in areas previously affected by colitis when white light endoscopy is used without dye spray chromoendoscopy or virtual chromoendoscopy. Additional biopsies should be taken from areas of prior dysplasia or poor mucosal visibility. Nontargeted biopsies are not routinely required if dye spray chromoendoscopy or virtual chromoendoscopy is performed using a high-defintion endoscope, but should be considered if there is a history of dysplasia or primary sclerosing cholangitis.
While these guidelines are geared towards adult gastroenterologists for colorectal cancer screening, some advice is universally applicable
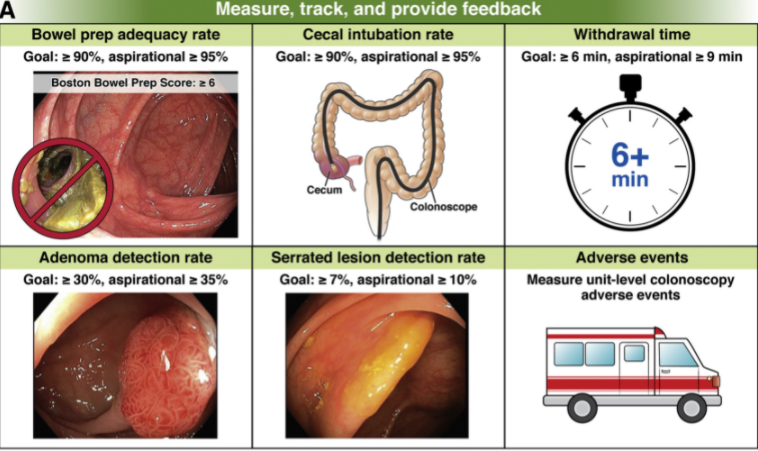
tracking quality metrics: good prep, cecal intubation rate, and adverse events
good bowel preparation instructions
detailed endoscopy reports
appropriate followup: All patients with advanced adenomas should have repeat colonoscopy in 3 years. Average-risk patients with normal screening colonoscopies or those with only small distal hyperplastic polyps should not undergo repeat examinations before 10 years
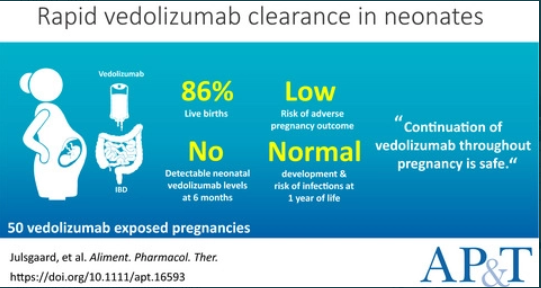
In 50 vedolizumab-exposed pregnancies, we observed 43 (86%) live births, seven (14%) miscarriages, no congenital malformations and low risk of adverse pregnancy outcomes
The mean time to vedolizumab clearance in infants was 3.8 months (95% CI, 3.1-4.4)
No infant had detectable levels of vedolizumab at 6 months of age
Developmental milestones at 12 months were normal or above average
Neither vedolizumab exposure in the third trimester (RR 0.54, 95% CI, 0.28-1.03) nor combination therapy with thiopurines (RR 1.29, 95% CI, 0.60-2.77) seemed to increase the risk of infections in the offspring
My take: Given the good safety profile of vedolizumab, this small study provides additional reassurance regarding use of vedolizumab during pregnancy.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
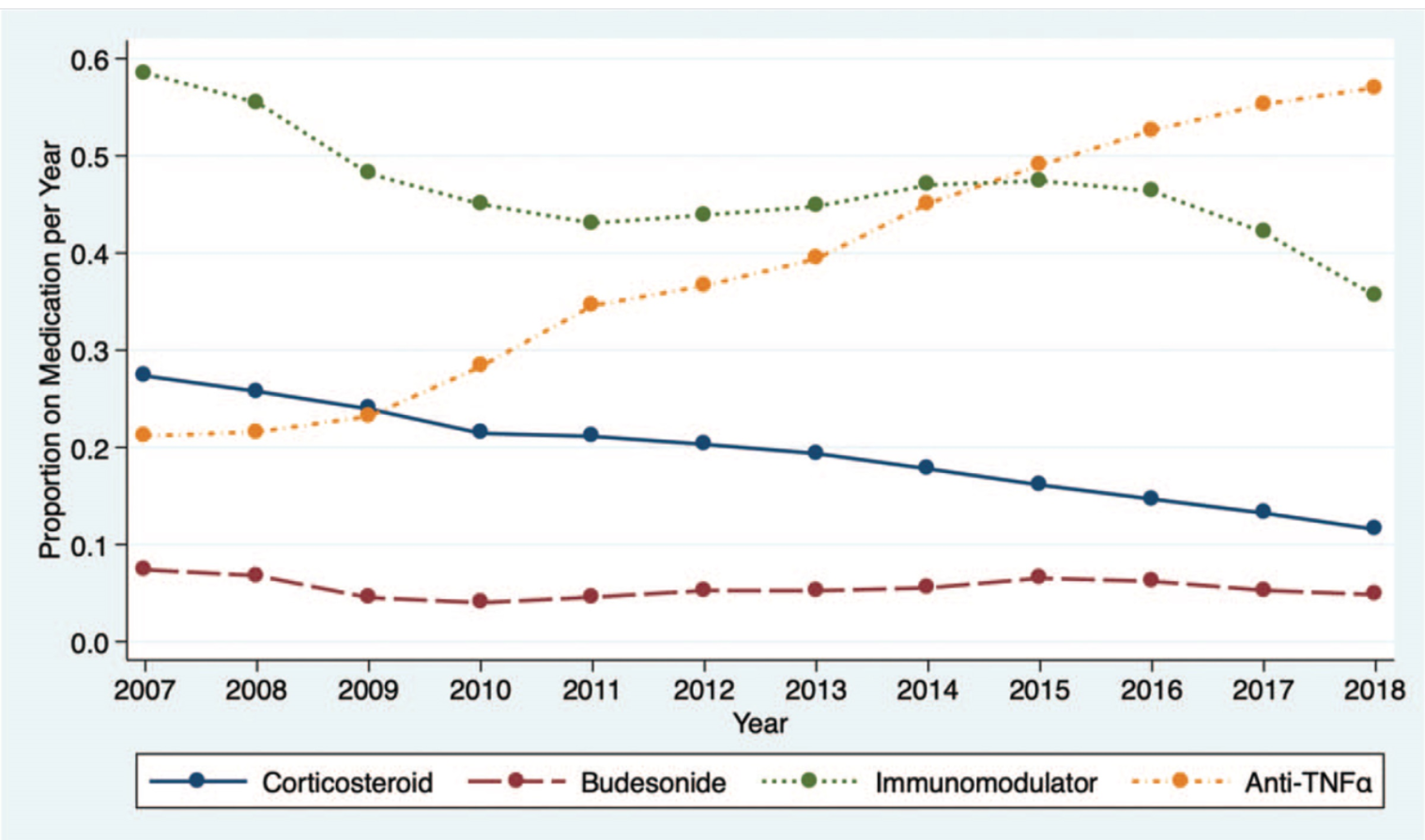
In this study of 27,321 patients enrolled in the ImproveCareNow (ICN) learning health system, key findings:
Corticosteroid use decreased from 28% (2007) to 12% (2018)
Black patients received corticosteroids more commonly than white patients. This disparity improved as corticosteroid use decreased in both groups
Anti-tumor necrosis factor-alpha medication use <120 days after diagnosis was associated with a reduction in corticosteroid use
As corticosteroid use decreased, steroid-sparing therapy use increased and height and weight z scores improved, particularly among children with Crohn disease
27 centers (31%) had a significant reduction in steroid use, 5 (6%) had a significant increase, and 45 (52%) had variability in steroid use. 9 centers (11%) had <2 years of data.
My take: These findings are expected but nice to see. Patients in the ICN are using less steroids and growing better. Given the variation in care among centers, there is more work needed.
There are a lot of articles that have been published regarding bowel preparations prior to colonoscopy, especially in adults. One of the key advances has been split-prep dosing, which is not utilized much in the pediatric age group.
Nevertheless, a recent pediatric study (S Kumar et al. JPGN 2021; 73: 325-328. Inadequate Bowel Preparation in Pediatric Colonoscopy—Prospective Study of Potential Causes) shows that inadequate bowel preparation in their prospective cohort (n=334) was less prevalent than that noted from typical adult data. Their bowel preparation assessmetn was based on Boston Bowel Preparation Scale (BBPS).
Key finding: Inadequate bowel preparation (IBP) was noted in 12.8% (41/321); there were no age, gender, obesity, race, or insurance type associated with IBP. (IBP was defined by BBPS <5)
Their preparation instructions:
If <25 kg, “119 g of PEG 3350 mixed in 32 oz of sport drink” and then “additional 32 oz of a sports drink without PEG 3350”
If 26-49 kg, “238 g of PEG 3350 mixed with 64 ounces of fluids” and then “additional 64 oz of a sports drink without PEG 3350”
If >50 kg, “238 g of PEG 3350 mixed with 64 ounces of fluids” and then “64 ounces of a sports drink and four bisacodyl tablets”
My take: If you are seeing a high rate of IBP, the prep instructions in this study could be replicated (given their good results), split preps could be given for teens, and better instructions (visual aids) could be needed.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.