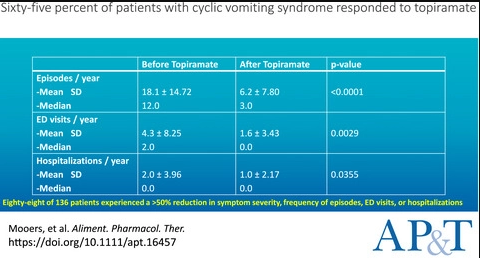
H Mooers et al. AP&T 2021; https://doi.org/10.1111/apt.16457 Retrospective review of patients treated for cyclic vomiting syndrome with topiramate
“Response was defined as a global improvement in symptoms or >50% reduction in the number of CVS episodes, ED visits or hospitalisations.” 92% of patients had previously failed TCA therapy.
Key findings:
- “Sixty-five percent (88/136) of patients responded to topiramate in an intent-to-treat analysis.”
- “There was a significant decrease in the annual number of CVS episodes (18.1 vs 6.2, P < 0.0001), CVS-related ED visits (4.3 vs 1.6, P = 0.0029), and CVS-related hospitalisations (2.0 vs 1.0, P = 0.035).”
- Fifty-five percent of patients experienced side effects, and 32% discontinued the medication as a result. The most common side effects were cognitive impairment (13%), fatigue (11%) and paresthesia (10%).
Related blog posts: