A recent Children’s Healthcare Webinar by Hillary Bashaw reviewed several nutrition topics. I took some notes and some screenshots. Some errors of omission and transcription may have occurred.
Key points from talk:
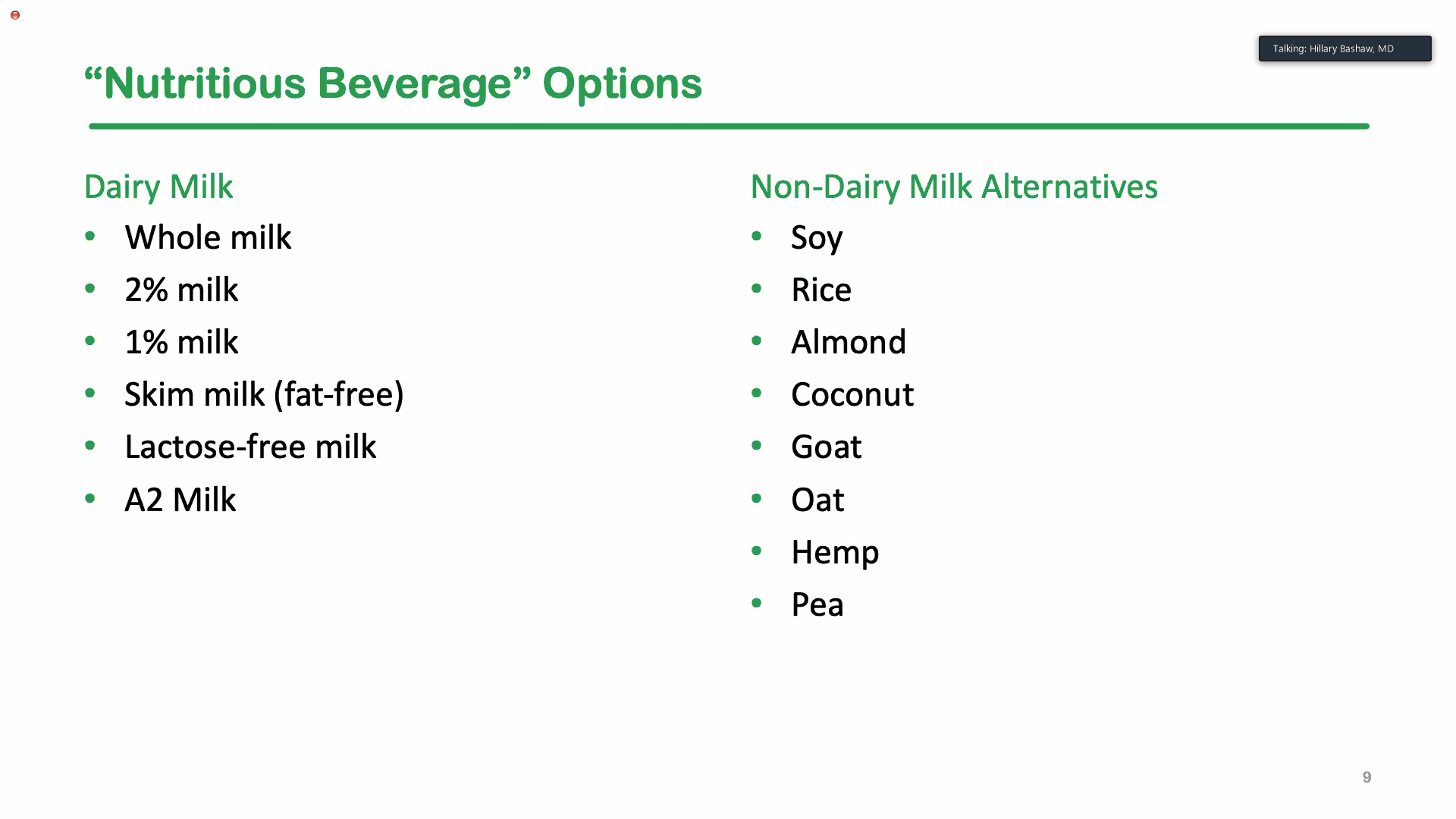
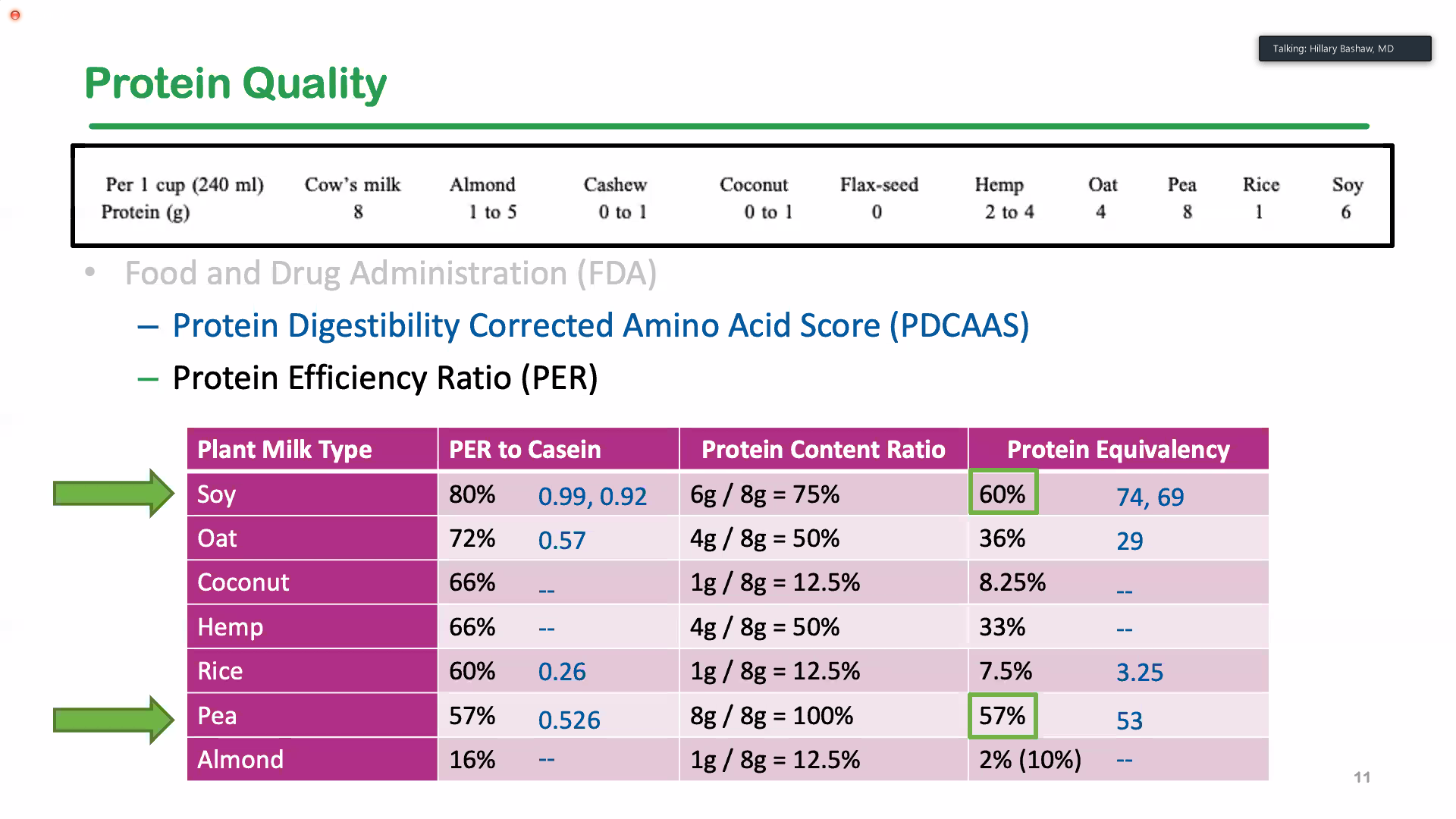
- Cow’s milk overall is a healthy beverage for children, though there are several plant-based alternatives that can be effective substitutes. Soy milk and pea-protein milk are often the best alternatives.
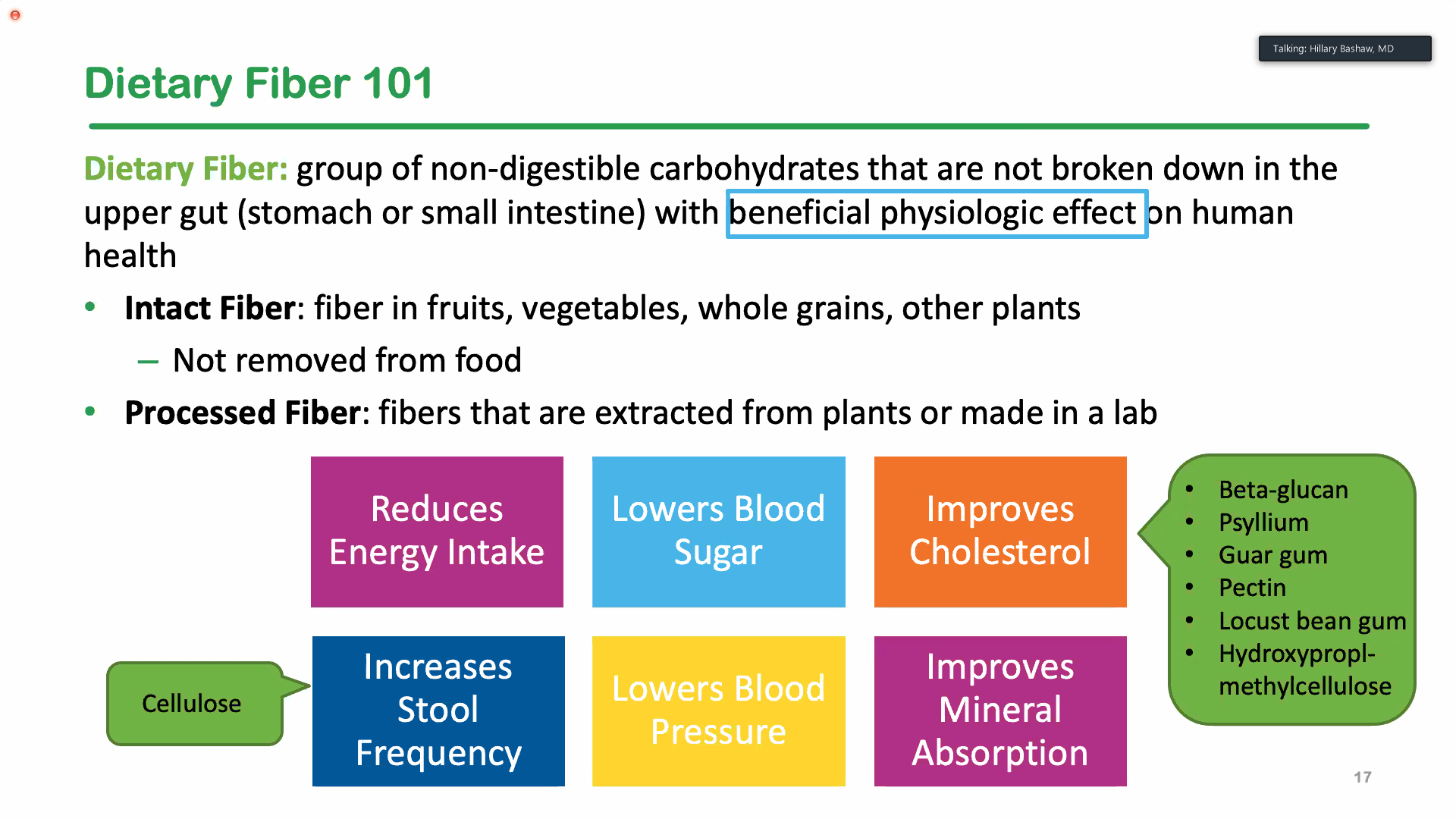
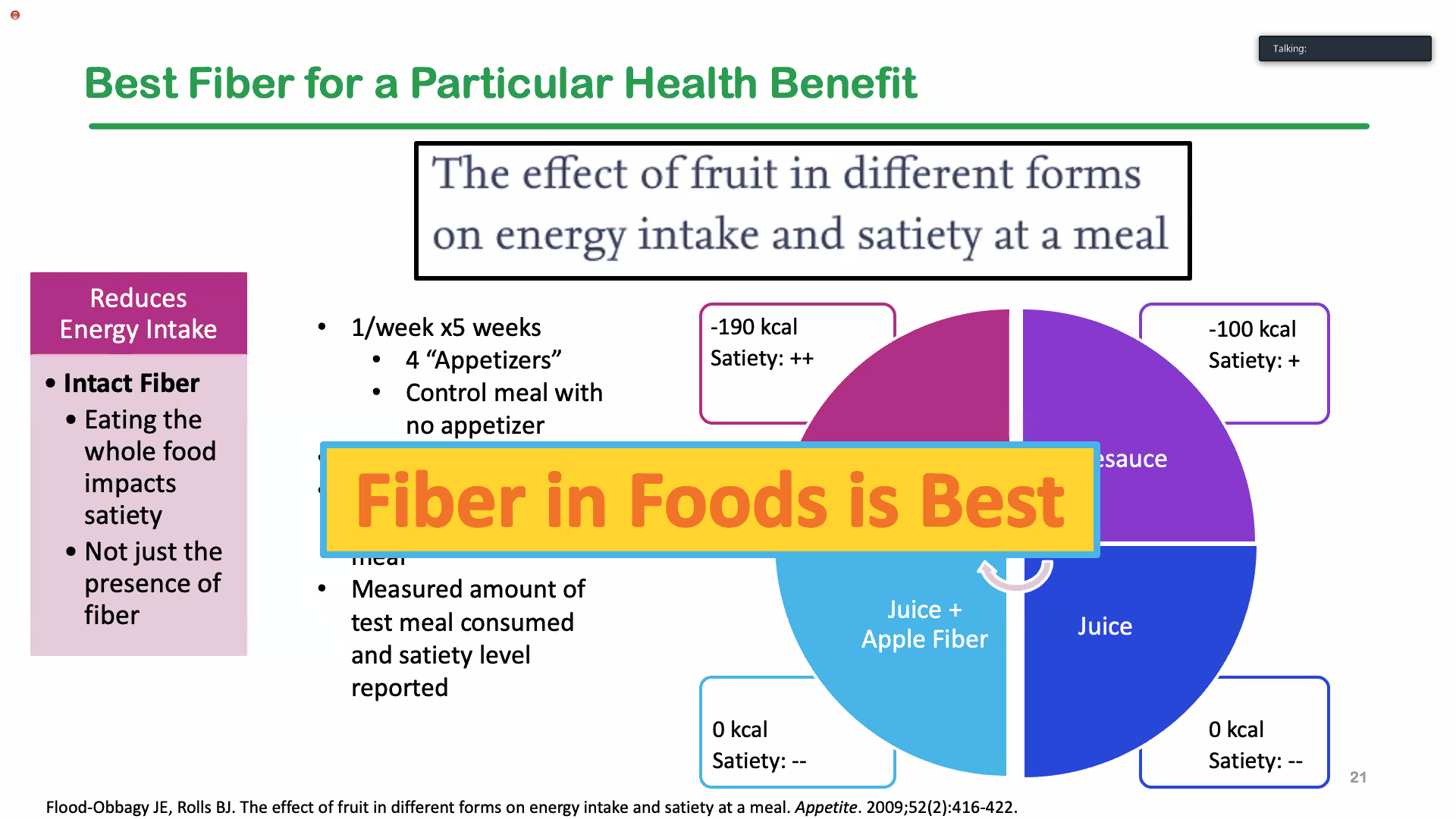
- Fiber from foods is the best way to get fiber. Gummy fiber products are not recommended.
- Eating breakfast likely helps with school performance; however, this does not mean it is the ‘most important’ meal of the day.
Related article: RJ Merritt et al. JPGN 2020; 71: 276–81. Full text link: NASPGHAN Position Paper: Plant-based Milks
- One of the slides from this talk modifies the Table 1 (adds skim milk) from this article.
- “Milk‘s contribution to the protein intake of young children is especially important. For almond or rice milk, an 8 oz serving provides only about 2% or 8%, respectively, of the protein equivalent found in a serving of CM.”
- “As presently constituted, almond, rice, coconut, hemp, flax seed, and cashew “milks” are inappropriate replacements for CM in toddlers and young children for whom milk remains an important part of the diet.”






Milk–related blog posts:
- It’s Complicated: The Relationship Between Milk and Health
- Is Drinking Milk Healthy?
- The Genius of Breastmilk | gutsandgrowth
- Overdiagnosis of Cow’s Milk Protein Allergy in Infants and Formula Industry Influence
- Pediatric Osteoporosis and Bone Health -Lecture Slides with commentary
Fiber:





Fiber–related blog posts:
- Why Fiber Matters?
- It’s Alimentary! Part 1
- Why Fiber (Fruits and Veggies) Is Good For You
- Eat your veggies…if you do not want to get sick
Breakfast:



Breakfast-related blog posts: