

A recent “Grand Rounds” review of venous thrombosis (VT) in pediatric inflammatory bowel disease (E Mitchel, T Diamond, L Albenberg. J Pediatr 2020; 216: 213-7) provides some practical advice in an area in need of more clarity.
Risk factors for VT:
Key points:
My take: In adolescents hospitalized with IBD, this article suggests that almost all should receive mechanical prophylaxis for VT and a subset at increased risk may benefit from pharmaccologic prophylaxis.
Related blog posts:

From a visit to Montreal
Previous studies have documented numerous deficiencies in the care of children with celiac disease, particularly with regard to followup. A recent study (B Sparks et al. J Pediatr 2020; 216: 32-6) demonstrates that using a prospective patient registry can improve many aspects of care and allows scrutiny of other aspects for further improvement.
In this single center study with 25 pediatric gastroenterologists, the authors reviewed the experience in establishing their “Celiac Care Index.”
Key findings:
When looking at their ‘smartset’ labs obtained in most of their 145 patients, the authors note that several may not be needed:
Lab Findings:
My take:
Related blog posts:

Signage at a restaurant’s bathroom near Mount Tremblant
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
A recent policy statement (SC Armstrong et al. Pediatrics 2019; 144 (6): e20193223) outlines current evidence regarding adolescent bariatric surgery and makes recommendations for practitioners & policymakers. There is also an accompanying technical report which provides more detail and supporting evidence. Thanks to Ben Gold for this reference.
Full PDF Link: Pediatric Metabolic and Bariatric Surgery: Evidence, Barriers, and Best Practices
This policy statement uses “adolescent” to refer to a person from age 13 years to age 18 years.
Background: “Although nearly 4.5 million US adolescents have severe obesity, current estimates suggest that only a small faction undergo metabolic and bariatric surgery…Many providers prefer a “watchful waiting” approach, or long-term lifestyle management.50 However, current evidence suggests that pediatric patients with severe obesity are unlikely to achieve a clinically significant and sustained weight reduction in lifestyle-based weight management programs53 and that watchful waiting may lead to higher BMI and more comorbid conditions…In addition, comparative data examining
postoperative outcomes along the severely obese BMI spectrum (low, middle, and high) suggest that adolescents within a lower BMI range (BMI <55) at the time of bariatric
surgery have a higher probability of achieving nonobese status when compared with individuals with a higher starting BMI (BMI ≥55).”
From Table 2 -Indications for Bariatric Surgery:
Recommendations for practitioners:
SYSTEM-LEVEL RECOMMENDATIONS:
My take: These recommendations are in general agreement with previous guidelines. I think having the stamp of approval from the AAP is likely to help in getting coverage and may shift attitudes.
Related blog posts:
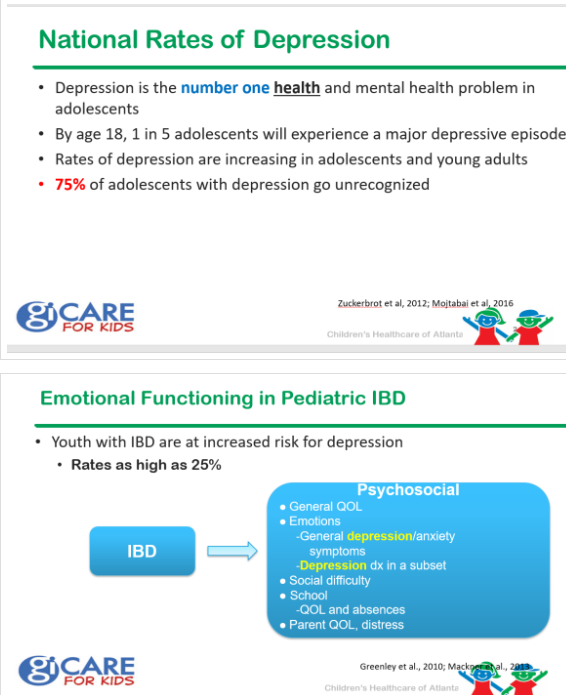
LM Mackner et al. JPGN 2020; 70: 42-47. Bonney Reed, our psychologist at GI Care for Kids is one of the authors as well.
Key points:
My take (borrowed from authors): “Implementing depression screening in a busy clinic may seem like a daunting task and is likely to require changes in workflow and procedures. Nonetheless, optimal IBD care treats all aspects of health, and identifying depression symptoms, that often go undetected and can affect IBD outcomes, benefits patients, families, and providers.” In our office, we have implemented screening and there is now a smartform available in EPIC. We are fortunate to work closely with psychologists who can help when there is an abnormal screen.
Related blog posts:
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
RS Choung et al. Gastroenterol 2020; 158: 151-9.
Full abstract link: (which has link to full text): “Community-Based Study of Celiac Disease Autoimmunity Progression in Adults”
Methods: In this prospective cohort study, waste blood samples from residents of a community were tested for CeD autoimmunity at 2 time points. We analyzed waste blood samples from 15,551 adults for tTGA and, if titer results were above 2 U/mL, for endomysial antibody. The median interval between the two time points was 8.8 years.
Results:

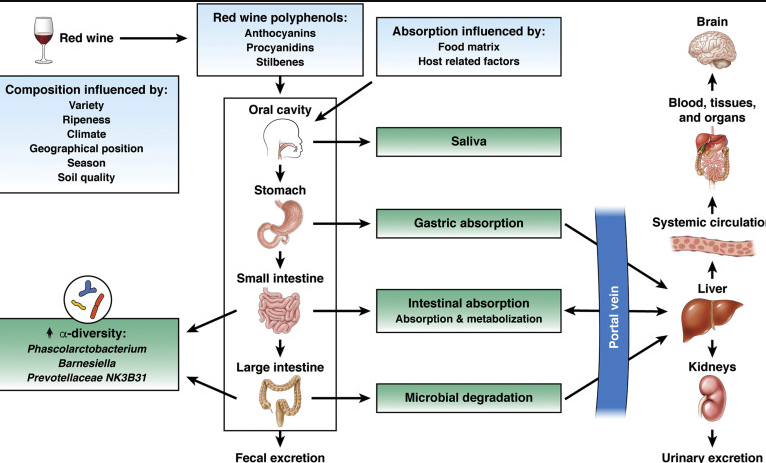
A recent study (C Le Roy et al. Gastroenterol 2020; 158: 270-2) has indicated that red wine (& to a lesser extent white wine) can improve the intestinal microbiome diversity.
A recent AGA blog provides some insight into this study: Is Red Wine Consumption Good For Your Intestinal Microbiome?
An excerpt:
Consumption of red wine polyphenols has been previously associated with health benefits ranging from reducing cardiovascular disease risk factors, metabolic syndrome, and depression to improving cognition…
Le Roy et al compared the effects of beer and cider, red wine, white wine, spirits, and sum of all alcohols on the α-diversity of the intestinal microbiota (determined from 16s ribosomal RNA sequence data) in discovery cohort of 916 women (from a study of twins in the United Kingdom) and 2 replication cohorts (in Europe and North America) using a linear mixed-effect model adjusted for age, body mass index, Healthy Eating Index scores, education, and family structure…
LeRoy et al found that red wine consumption was associated, in a frequency-dependent manner, with α-diversity—even rare consumption had an effect. White wine was associated with α-diversity to a lesser extent, and there was no association with other alcohol categories…
LeRoy et al also observed a direct association between red wine consumption and blood level of insulin and high-density lipoprotein.
[Limitations] this was a cross-sectional and observational study; randomized studies would be needed to determine whether red wine drinking has direct effects on composition of the intestinal microbiome and health outcomes…
My view: If you like to drink red wine, that’s fine but I would be reluctant to expect a health benefit –no matter how great your poop is. As the associated editorial notes, “high consumption of alcohol has many adverse health effects, including development of cirrhosis. So, it remains to be determined whether long-term trials of red wine can be safely managed in an ethically responsible manner. It will be important to identify doses that provide beneficial health effects without reducing gut barrier integrity.”
Related blog posts
YouTube: How to Create a Better Research Poster in Less Time
This ~20 minute reviews how to create a research poster that conveys the main message for more conference attendees.

According to a recent study (NEJM 2019; 381: 2529-40), correction of vitamin D deficiency in critically-ill has NO significant effects on mortality and other non-fatal outcomes.
Link to abstract: Early High-Dose Vitamin D3 for Critically Ill, Vitamin D–Deficient Patients
The article notes that observational data have indicated that Vitamin D deficiency is common in critically ill patients and has been associated with longer lengths of stay, prolonged ventilation and death. However, “vitamin D level is considered a marker of coexisting conditions and frailty, and residual confounding may drive theses associations.”
Methods: a randomized, double-blind, placebo-controlled, phase 3 trial of early vitamin D3 supplementation in critically ill, vitamin D–deficient patients who were at high risk for death. Randomization occurred within 12 hours after the decision to admit the patient to an intensive care unit. Eligible patients received a single enteral dose of 540,000 IU of vitamin D3 or matched placebo.
Results:
My take: Correction of low serum vitamin D levels did not improve outcomes. This likely indicates that low vitamin D levels are often an epiphenomenon of critical illness and not a contributing causal etiology.
Related blog posts:

Montreal
S Nagai et al. Clin Gastroenterol Hepatol 2019; 17: 2759-68. For patients who underwent liver transplantation during 2016–2017, a significantly lower proportion of patients with NASH survived for 1 year after transplantation than patients with HCV (P = .004) or ALD (P < .001). 1-year patient survival rates: NASH 90.4%, HCV 92.8%, ALD 93.5%. Full Text: Increased Risk of Death in First Year After Liver Transplantation Among Patients With Nonalcoholic Steatohepatitis vs Liver Disease of Other Etiologies
JE Squires et al. JPGN 2020; 70: 79-86. Using a prospective, longitudinal database, this study from ChiLDReN network with 93 children with biliary atresia and native liver found that NO increased prevalence of neurodevelopmental delays. Markers of advanced liver disease (high bilirubin/GGT for those ≤5 yrs, and portal hypertension for those >5 years) did negatively affect neurodevelopmental measures.
C Jaramillo et al. JPGN 2020; 70: 87-92. This pilot study with 21 patients found that degree of fibrosis, quantified by collagen hybridizing peptide, at time of Kasai, was associated with the risk of requiring a liver transplantation by age 4 years. Total bilirubin >2 mg/dL and Albumin ❤ g/dL at 3 months post-Kasai were also associated significantly with need for liver transplantation.
H-S Chen et al. Hepatology 2019; 70: 1903-12. In this study from Taiwan with 182 children (median age of 10.6 at enrollment) with hepatitis B and a normal ALT, a baseline anti-HBc titer of >500 IU/mL was associated with spontaneous HBeAg seroconversion with hazard ratio of 2.81. Over the median follow-up of 19.8 years, 85 subjects (46.7%) had HBeAg seroconversion. Thus, anit-HBc reflects anti-HBV immune response in the HBeAg-positive patients with normal ALT.

