“There is no consensus regarding optimal management in instances of Orbeez™ ingestion. However, a review of reported cases from 2021 indicated that of 43 cases of bowel obstruction secondary to water bead ingestions, two patients required endoscopic removal and the remaining 41 required surgical enterotomy or intestinal resection. We report a case of successful medical management following ingestion of over 1000 water beads…The patient was placed on a clear liquid diet and received a mineral oil enema with minimal passage of beads. She was then started on sennosides and erythromycin ethylsuccinate to help stimulate expulsion. Stools were closely monitored and revealed passage of greater than 1000 beads over the next 24 h.”
GI and Hepatology News, Open Access: Watershed Moment’: Semaglutide Shown to Be Effective in MASH (November 2024): “At 72 weeks, a 2.4-mg once-weekly subcutaneous dose of semaglutide demonstrated superiority, compared with placebo, for the two primary endpoints: Resolution of steatohepatitis with no worsening of fibrosis and improvement in liver fibrosis with no worsening of steatohepatitis.”
“ESSENCE (NCT04822181) is an ongoing multicenter, phase 3 randomized, double-blind, placebo-controlled outcome trial studying semaglutide for the potential treatment of MASH.” Cohort: N=1200, biopsy-defined MASH and fibrosis, stages F2 and F3…”After initiation, the semaglutide dosage was increased every 4 weeks up to 16 weeks when the full dose (2.4 mg) was reached.”
Key findings:
62.9% of those in the semaglutide group and 34.1% of those in the placebo group reached resolution of steatohepatitis with no worsening of fibrosis.
37% of those in the semaglutide group and 22.5% of those in the placebo group had improvement in liver fibrosis with no worsening of steatohepatitis
Weight loss was also significant, with a 10.5% reduction in the semaglutide group compared with a 2% reduction in the placebo group
No new safety signals were identified
Cardiometabolic risk factors improved as well, with changes in blood pressure measurements, hemoglobin A1c scores, and cholesterol values.
20%-40% improvements in liver enzymes and noninvasive fibrosis markers, such as ELF and vibration-controlled transient elastography liver stiffness.
My take: This expected finding indicates that more GLP-1 agents are likely to be approved for MASH treatment. Survodutide received “U.S. FDA Breakthrough Therapy” in October 2024.
JHW Zhang et al. NEJM 391: 2098-2109. Xalnesiran with or without an Immunomodulator in Chronic Hepatitis B
Background: Xalnesiran, a small interfering RNA molecule that targets a conserved region of the hepatitis B virus (HBV) genome and silences multiple HBV transcripts.
Methods: This was a phase 2, multicenter, randomized, controlled, adaptive, open-label platform trial that included the evaluation of 48 weeks of treatment with xalnesiran at a dose of 100 mg (group 1), xalnesiran at a dose of 200 mg (group 2), xalnesiran at a dose of 200 mg plus 150 mg of ruzotolimod (group 3), xalnesiran at a dose of 200 mg plus 180 μg of pegylated interferon alfa-2a (group 4), or a nucleoside or nucleotide analogue (NA) alone (group 5) in participants with chronic HBV infection who had virologic suppression with NA therapy. The primary efficacy end point was hepatitis B surface antigen (HBsAg) loss (HBsAg level, <0.05 IU per milliliter) at 24 weeks after the end of treatment.
Key findings:
In the associated editorial by Janssen et al. (NEJM 2024;391:2163-2168), the authors note that “nucleoside or nucleotide analogues currently form the backbone of therapy for most patients with chronic HBV infection who have access to treatment…However, treatment must be continued on a long-term basis…Although treatment with nucleoside or nucleotide analogues is associated with a decrease in the severity of liver fibrosis and reduction of liver-related complications, the risk of hepatocellular carcinoma persists at the population level because functional cure is not achieved in most patients.”
“Further data are needed on the durability of the effect achieved with new agents that directly interfere with HBsAg production. The results reported by Hou et al. indicate a risk of relapse, undermining the choice of functional cure as an end point for these agents, at least when assessed relatively early after the withdrawal of therapy…Hou et al. observed that functional cure was achieved only in patients with a baseline HBsAg level of less than 1000 IU per milliliter. Although a substantial proportion of patients have similarly low HBsAg levels, patients with higher HBsAg levels have the greatest risk of adverse liver-related outcomes and thus have the most to gain from new therapies.”
My take: While this study represents important progress, it is not likely to change current treatment strategies in the near-term. Even better than treating HBV is preventing HBV. The best strategy for reducing HBV mortality and morbidity still relies of wide-scale use of the highly effective HBV vaccine.
The authors utilized prospectively collected data from 3 population-based birth cohorts (Danish National Birth Cohort, Norwegian Mother, Father, and Child Cohort, and All Babies in Southeast Sweden). This collectively included nearly 170,000 offspring.
Key findings:
During median follow-up of 16.3–22.3 years, between 1996 and 2021, 543 offspring were diagnosed with IBD
In each country, there was no association between exclusive breastfeeding duration and offspring IBD risk
Discussion:
“In contrast to majority of case-control studies, both cohort studies reported null association between breastfeeding, treated as a binary exposure (any versus no breastfeeding) or by duration, and offspring IBD risk. Similarly, 2 nested case-control studies, leveraging prospectively collected data on early life exposures as part of the population-based Jerusalem Perinatal Study and 2 United Kingdom birth cohorts (the 1946 National Survey of Health & Development and the 1958 National Child Development Study) reported null associations between breastfeeding and IBD risk.22,23 Data from these studies, which are more rigorous in methodology compared with case-control studies, are consistent with findings from our analyses.”
My take: While this study has some limitations inherent in observational data, this study with prospectively-collected data indicates that breastfeeding did not modulate the risk of developing IBD.
Methods: The authors used a cross-sectional study using data from the National Health and Nutrition Examination Survey (2005-2010) and they used two 24-hour dietary recalls and, based on the Nova classification, calculated intakes of ultra-processed foods (UPFs) and minimally-processed foods (MPFs). N=12,716 adults.
Key Findings:
Median UPF and MPF intakes were 26.5% and 66.2% of total grams per day, respectively
Greater UPF consumption (in % gram/d) was associated with higher odds of constipation (adjusted OR [aORQ4 vs Q1], 2.20]
Discussion point: The authors did not find an association with diarrhea. “UPF consumption has been associated with increased risks of GI disorders that can cause chronic diarrhea including IBD and irritable bowel syndrome (IBS). This was thought to be related to alteration of the gut barrier integrity and activation of the immune response in the setting of microbial dysbiosis. The overall effect induces a pro-inflammatory micro-environment in the intestine and alterations in bowel function. However, the amount of UPFs needed to be consumed by individuals such that the risk of diarrhea would be higher is unknown and likely varies between individuals.”
My take: Limiting UPFs and promoting fresh foods/minimally-processed foods is better for our health.
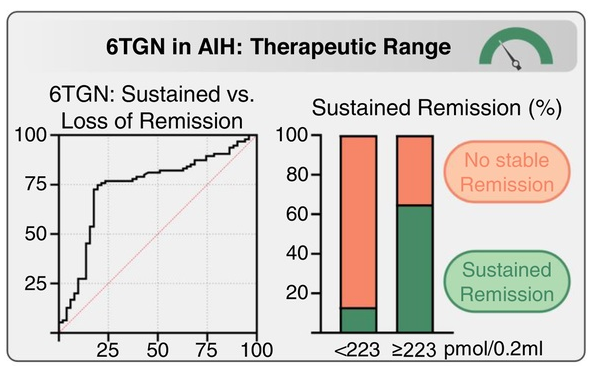
Over 4 years (N = 146), patients with higher average 6TGN levels were associated with those with stable complete biochemical remission (CBR) (260 pmol/0.2 mL) compared to those failing to maintain CBR (181 pmol/0.2 mL; p = 0.0014) or never achieving CBR (153 pmol/0.2 mL; p < 0.0001), with an optimal 6TGN cutoff of ≥223 pmol/0.2 mL
Adding allopurinol to thiopurines in difficult-to-treat patients (N = 36) raised 6TGN (168→321 pmol/0.2 mL; p < 0.0001) and lowered 6MMP (2125→184 pmol/0.2 mL; p < 0.0001), resulting in improved transaminases in all patients and long-term CBR in 75%.
Limitation: most of the 337 patients did NOT have sequential azathioprine metabolite monitoring. This could indicate that the 146 patients with sequential monitoring could have a selection bias favoring patients with a more aggressive disease course. Thus, the proposed 6-TGN level of 223 may not be applicable for all patients.
From editorial:
“In this issue of Hepatology, “Weltzsch et al1 conducted a multicenter study on the metabolic monitoring of thiopurines in AIH. The authors defined an optimal cutoff of ≥223 pmol/0.2 mL average 6TG level to maintain long-term biochemical remission (BR). Notably, 66% of patients with 6TG levels above this cutoff sustained BR rates.
Allopurinol shifts the thiopurine metabolism toward 6TG production, allowing thiopurine dose reduction to 25%–30%, which improves efficacy and tolerability. (The 100 mg dose of allopurinol had more favorable 6MMP/6TG ratio).
However, they note that in a prior study (J Hepatol 2021; 75: 324-32), “patients with subtherapeutic 6TG levels (75–225) achieved similar BR rates (75% vs. 81%, p = 0.589) to those with therapeutic levels (225–450), while experiencing significantly fewer adverse drug reactions (44% vs. 86%, p = 0.0002).”
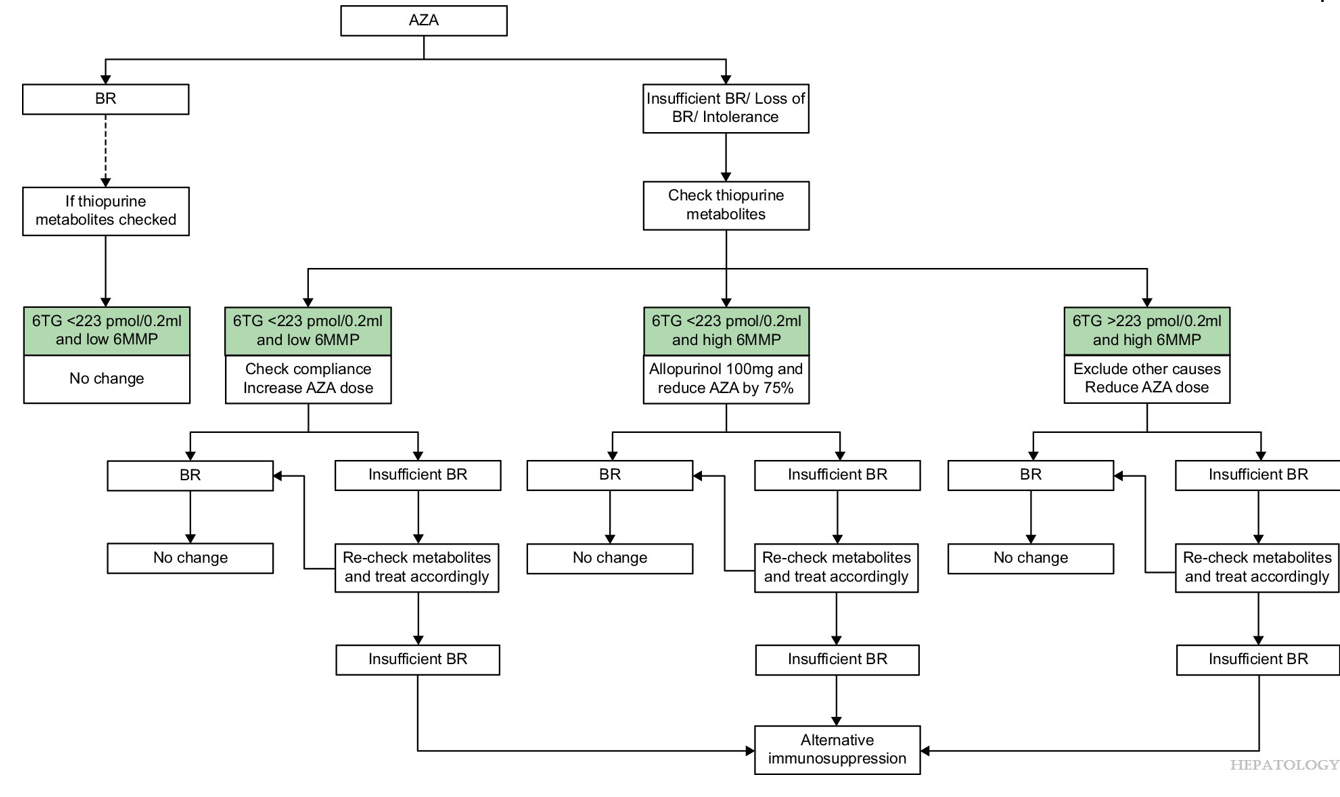
Proposed Algorithm
My take: This study shows in patients who have not achieved a biochemical remission, optimization of azathioprine dosing with metabolite monitoring improves biochemical remission. In those with low 6TG and low 6MMP, increasing the azathioprine should be considered. In those with low 6TG and high 6MMP, reducing azathioprine and adding allopurinol should be considered.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
With regard to achalasia, “Botox can be considered only in patients in whom rapid weight gain is important to improve surgical outcomes.”
With regard to gastroparesis/delayed gastric emptying in children, the authors note the following:
‘A recent retrospective study from the Mayo Clinic analysed the response to intrapyloric Botox in children (n = 20) with gastroparesis and concluded that intrapyloric Botox injection in children is safe and can provide temporary relief for patients with refractory upper gastrointestinal symptoms with and without gastroparesis.43 [This was] a meta-analysis, including six studies, 160 patients, which showed that 68% of patients responded to intrapyloric Botox irrespective of the presence of gastroparesis, while among patients diagnosed with gastroparesis the therapeutic response was 66%.43 These results suggest that intrapyloric Botox can be effective not only in children with gastroparesis but also in children with refractory functional upper gastrointestinal symptoms.’ In their conclusion, the authors note “Intrapyloric Botox injection is increasingly used for the treatment of gastroparesis but evidence supporting its use in children is still scarce.”
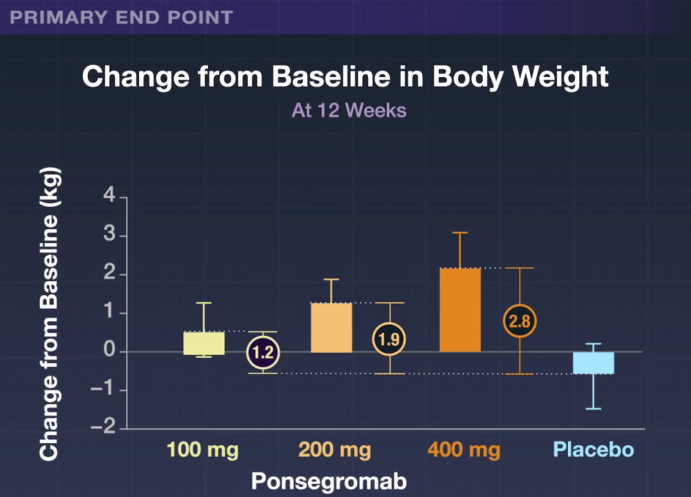
JD Groarke, et al. NEJM 2024; 391: 2291-2303. Ponsegromab for the Treatment of Cancer Cachexia
Background: “Growth differentiation factor 15 (GDF-15) is a stress-induced cytokine that binds to the glial cell–derived neurotrophic factor family receptor alpha-like protein (GFRAL) in the hindbrain.12 The GDF-15–GFRAL pathway has emerged as a main modulator of anorexia and body-weight regulation and is implicated in the pathogenesis of cachexia.13 …Ponsegromab (PF-06946860) is a potent, highly selective, humanized monoclonal antibody that binds to circulating GDF-15, thereby inhibiting the interaction with its GFRAL receptor.”
“A recent guideline supports low-dose olanzapine to improve appetite and weight in patients with advanced cancer,3 a recommendation that is largely based on a single-center study.4 Safe, effective, and targeted therapies for cancer cachexia are needed.10,11“
Methods: In this phase 2, randomized, double-blind, 12-week trial, we assigned patients with cancer cachexia and an elevated serum GDF-15 level (≥1500 pg per milliliter) in a 1:1:1:1 ratio to receive ponsegromab at a dose of 100 mg, 200 mg, or 400 mg or to receive placebo, administered subcutaneously every 4 weeks for three doses. N=187. Of these patients, 40% had non–small-cell lung cancer, 32% had pancreatic cancer, and 29% had colorectal cancer.
Key findings:
Over the 12-week trial, patients treated with ponsegromab had as much as a 2.8 kg weight gain compared to placebo.
Improvements were observed across measures of appetite and cachexia symptoms, along with physical activity, in the 400-mg ponsegromab group relative to placebo.
My take: This study explains a key driver of cachexia in cancer and shows that inhibition of GDF-15 can improve weight gain and physical activity.
For those of you with an interest in improving our healthcare system, I highly recommend either Eric Topol’s Ground Truths Podcast with Mark Cuban or the transcription of their discussion. Both can be found here: Mark Cuban: A Master Disrupter for American Healthcare
Mark Cuban describes the expansion of his generic pharmacy business Cost Plus Drugs. But the main focus is on other aspects of healthcare like pharmacy benefits managers, insurance companies and improving patient access.
“So a big part of my time these days is going to CEOs and sitting with them and explaining to them that you’re getting ripped off on both your pharmacy and your healthcare side….”
“Because when you see stories like we’ve all seen in news of a big healthcare, a BUCA healthcare (Blue Cross Blue Shield (BCBS), UnitedHealth, Cigna, and Aetna/CVS) plan with all the pre-authorizations and denials, typically they’re not even taking the insurance risk. They’re acting as the TPA (third party administrator) as the claims processor effectively for whoever hired them. And it goes back again, just like I talked about before. And as long as CMS hires or allows or accepts these BUCAs with these plans for Medicare for the ACA (Affordable care Act), whatever it may be, it’s not going to work. As long as self-insured employers and the 50 million lives they cover hire these BUCAs to act as the TPAs, not as insurance companies and give them leeway on what to approve and what to authorize and what not to authorize. The system’s going to be a mess, and that’s where we are today.”
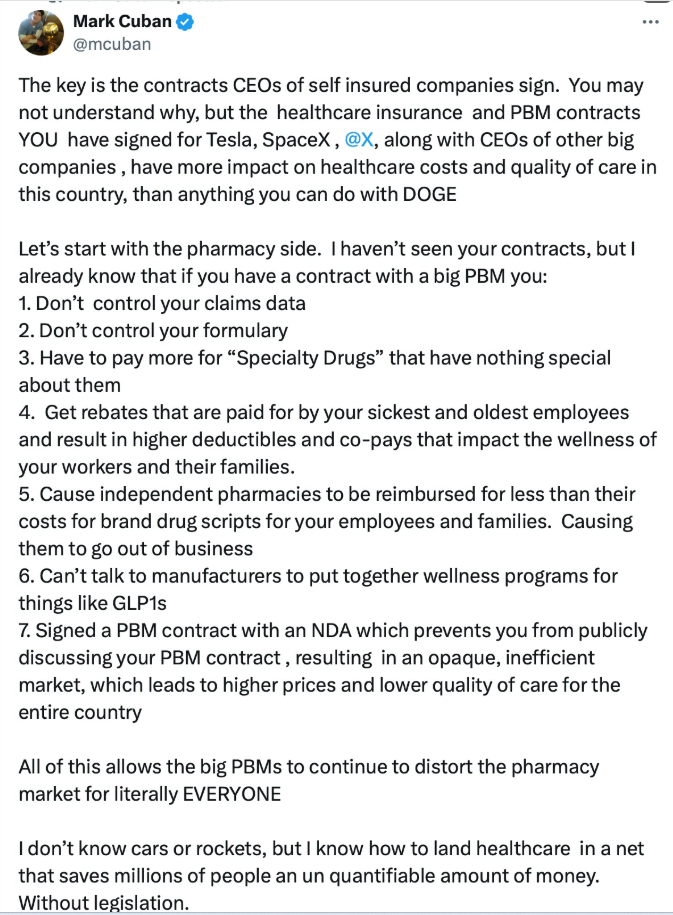
In response to a post by Elon Musk that Americans are not getting a good deal with their healthcare expenditures, Mark Cuban posted the following:
“Because we’re cutting out all those ancillary costs and credit risk, I want Medicare pricing. Now the initial response is, well, Medicare prices, that’s awful. We can’t do it. Well, when you really think about the cost and operating costs of a hospital, it’s not the doctors, it’s not the facilities, it’s all the administration that cost all the money. It’s all the credit risks that cost all the money. And so, if you remove that credit risk and all the administration, all those people, all that real estate, all those benefits and overhead associated with them, now all of a sudden selling at a Medicare price for that hip replacement is really profitable.”
He also describes how his employees pay premiums but no additional costs and how to get to universal health coverage. “Why do we need insurance companies if they’re not even truly acting as insurance companies?“
A recent Vanity Fair Article echoed some of the problems that our group has experienced with insurance companies.
An excerpt:
While no one can seriously justify the decision to gun down a father of two to make a political point, Americans seem to agree on one thing: Something does need to be done about the country’s broken health insurance system.
The brutal slaying, and the frenzied manhunt that followed, have exposed widespread frustration with a system of for-profit health insurance that many Americans feel is actually killing them, one delayed-or-denied health insurance claim at a time. And doctors are as fed up as their patients…
Struggling with the seemingly arbitrary policies and undermarket reimbursements offered by UnitedHealth Group and other insurers, doctors feel trapped in a zero-sum game that has robbed them of their clinical independence.
Four companies, known collectively as BUCA—Blue Cross and Blue Shield, UnitedHealth, Cigna, and Aetna—have become so powerful that “when doctors try to negotiate, they have to take whatever that carrier gives them,” says Ron Howrigon, a health care consultant who represents doctors in their dealings with insurers…
Amid this anger, UnitedHealth stands out for its sheer size, its aggressive moves to vertically integrate healthcare, and its expansive denial of claims, say health care experts and doctors. Headquartered in Minnetonka, Minnesota, it is a behemoth that took in more than $370 billion last year, making it America’s fourth-largest corporation by revenue. It insures more than 26 million Americans. More than one tenth of US doctors are either employed by or affiliated with the UnitedHealth subsidiary Optum Health…
Doctors in independent practice groups describe strong-arm tactics by the company—suddenly pushing them out of network, slashing their reimbursements, and stranding their patients with almost no notice. “Their interest is in killing private practice physicians,” says a North Carolina anesthesiologist…
The travails of Rheumatology Associates, P.C., the largest private rheumatology practice in Indiana, is a case in point. UnitedHealth offered the doctors in the group such paltry reimbursements that negotiations on a new contract ground to a halt…The group met with the Indiana attorney general’s office…
The company’s conduct was often nightmarish, even for patients in network. “Even when we get approvals on their letterhead, they would turn around, deny claims, and say they were approved incorrectly.”…
“They have so much power, they are out of control. They believe they are untouchable.”
My take: In the article, a health policy physician states the following: “Commercial Insurance Isn’t in the Health Care Business. It’s in the Financial Business.”
Our group is currently out of network with UnitedHealth. We negotiated with them for more than two years and offered them rates that were as good or better than all of the other commercial insurers. Their claims about trying to negotiate rates that are “affordable for consumers and providers” are misleading. In our case, they are making their insured patients pay much more by forcing them to see other providers at an academic center with much higher costs, less availability, and longer travel distances. They don’t care about forcing patients, who have had long-standing relationships, to find new doctors or the inconvenience and cost to patient families. Their aim is to leverage their consolidation of coverage to force smaller groups to accept lower reimbursements. Over time, this will lead to even fewer options for patients.