L Peyrin-Biroulet et al. NEJM 2024; 391:213-223. Risankizumab versus Ustekinumab for Moderate-to-Severe Crohn’s Disease
Background: “Interleukin-23 is a heterodimeric proinflammatory cytokine comprising a p40 subunit shared with interleukin-12 and a unique p19 subunit that plays a key role in skin, joint, and gastrointestinal inflammation.16 Ustekinumab and risankizumab are humanized IgG1 monoclonal antibodies; ustekinumab selectively binds p40, and risankizumab selectively binds p19…In head-to-head trials directly comparing their efficacy in psoriasis, risankizumab was superior to ustekinumab, which suggests greater efficacy with p19 blockade than with p40 blockade.”
This “SEQUENCE” trial was a phase 3b, multicenter, open-label, randomized controlled trial with 527 patients with moderate-to-severe Crohn’s disease who either had an inadequate response or had intolerance to anti-TNF agents, received either risankizumab or ustekinumab.
Key Findings:

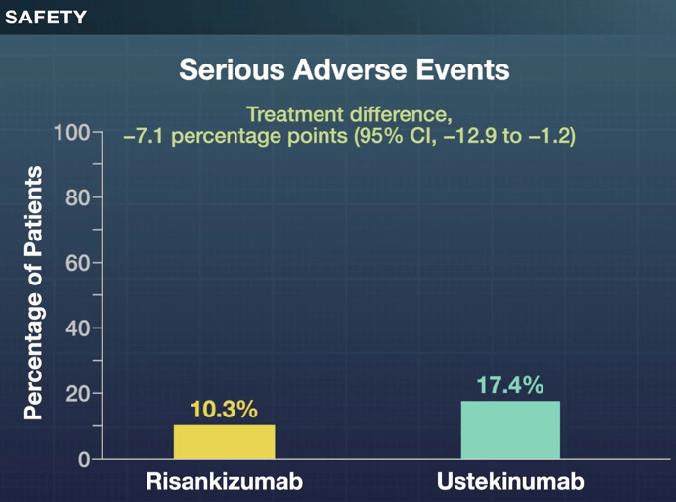
- A higher percentage of patients in the risankizumab group than in the ustekinumab group completed all the assigned treatment (90.2% [230 of 255 patients] vs. 72.8% [193 of 265 patients]). The primary reason for discontinuation of risankizumab was an adverse event (3.1% [8 of 255 patients]), and the primary reason for discontinuation of ustekinumab was lack of efficacy (13.2% [35 of 265 patients]
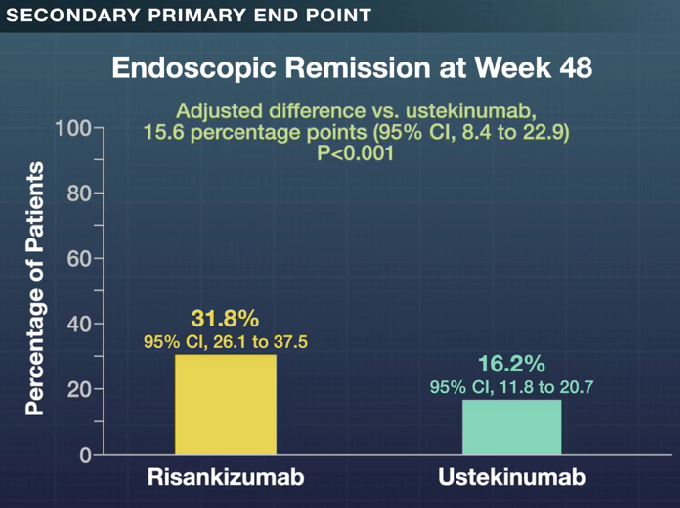
- Clinical remission at 48 weeks was 60.8% with risankizumab and 40.8%% with ustekinumab (P<0.001); there were similar rates of glucocorticoid-free clinical remission, 60.8% vs 40.4% respectively. Endoscopic response at 48 weeks was 45.1% and 21.9% respectively.
My take: These head-to-head results showed the superiority of risankizumab over ustekinumab across numerous clinical and endoscopic end points, including glucocorticoid-free clinical remission and endoscopic remission. However, it is still concerning to me that endoscopic remission rates were only 32% at 1 year and that less than half had an endoscopic response.
Related blog posts: