My IT advisor (my youngest son) recommends using the Stolen Device Protection setting on the iPhone. The link below explains the rationale for this change, what’s affected, and how to adjust your settings.
N Hadzic et al. NEJM 2024; 390: 284-286.JAK Inhibition in STAT1 Gain-of-Function–Mediated Treatment-Resistant Autoimmune Hepatitis
In this case report, the authors describe a 21 month old who presented with jaundice and abnormal liver tests. Diagnostic evaluation identified high titers of LKM antibodies (1:10,520) along with liver biopsy findings consistent with type 2 autoimmune hepatitis (AIH). After 6 months of treatment with steroids and subsequently azathioprine, the patient continued with severe biochemical relapses and a liver biopsy showed only a partial response.
Subsequently, “genetic testing found the patient had a heterozygous c.821G→A p.(Arg274Gln) pathogenic variant in the gene encoding signal transducer and activator of transcription 1 (STAT1)… Functional assays in the patient repeatedly showed abnormally high STAT1 phosphorylation as compared with healthy controls; this confirmed an autosomal dominant STAT1 gain-of-function defect.”
Treatment with “baricitinib, an inhibitor of Janus kinase 1 (JAK1) and 2 (JAK2), was started. Within weeks, the patient’s aminotransferase levels normalized. ..A liver-biopsy sample that was obtained 4 months after the initiation of baricitinib therapy showed an absence of appreciable inflammation with residual mild fibrosis…She was weaned off mycophenolate and is continuing to receive daily baricitinib (8 mg) and prednisolone (2.5 mg) along with fluconazole and azithromycin for infection prophylaxis.”
My take: In children with refractory autoimmune hepatitis, genetic testing is worthwhile and may allow targeted therapy.
Patterns and Puzzles with VEO-IBD This is a very good review and the image on this day has one of my favorite patient t-shirts. STAT gain-of-function defects can cause VEO-IBD picture as well.
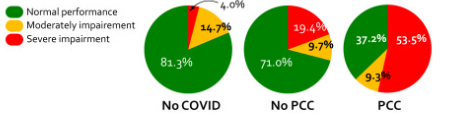
Methods: To examine cognitive slowing, patients with post-COVID-19 conditions (PCC) completed two short web-based cognitive tasks, Simple Reaction Time (SRT) and Number Vigilance Test (NVT). 270 patients diagnosed with PCC at two different clinics in UK and Germany were compared to two control groups: individuals who contracted COVID-19 before but did not experience PCC after recovery. For the SRT, participants were required to press the spacebar when a large red circle appeared in the center of the screen.
.**The simple reaction time task and the number vigilance task can be tried online at [https://octalportal.com/pcc]..
Key finding:
There was pronounced cognitive slowing in patients with PCC, which distinguished them from age-matched healthy individuals who previously had symptomatic COVID-19 but did not manifest PCC. Cognitive slowing was evident even on a 30-s task measuring simple reaction time (SRT), with patients with PCC responding to stimuli ∼3 standard deviations slower than healthy controls. 53.5% of patients with PCC’s response speed was slower than 2 standard deviations from the control mean, indicating a high prevalence of cognitive slowing in PCC.
Comorbidities such as fatigue, depression, anxiety, sleep disturbance, and post-traumatic stress disorder did not account for the extent of cognitive slowing in patients with PCC.
Cognitive slowing on the SRT was highly correlated with the poor performance of patients with PCC on the NVT measure of sustained attention.
Results of simple reaction time
My take (borrowed from authors): Using a 30-s web-based, self-administered psychomotor task, cognitive slowing in PCC can be reliably and easily measured as part of diagnostic work-up, and has potential to be a biomarker to track the progress of rehabilitation of PCC.
**The simple reaction time task and the number vigilance task can be tried online at [https://octalportal.com/pcc].
Gastroenterol 2024; 166: 87. Open Access! Spotlight (1 page summary)
Key recommendations
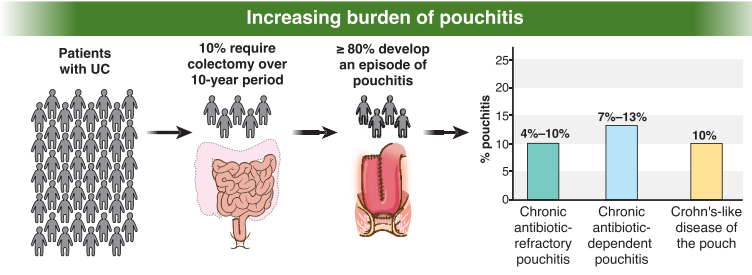
AGA recommends metronidazole and/or ciprofloxacin as preferred treatment of pouchitis with duration of treatment 2-4 weeks.
For Crohn’s-like disease of the pouch, AGA guideline recommends using either ileal-release budesonide or advanced immunosuppressive agents (eg. Biological therapies and small molecule therapies)
“In patients with cuffitis, topical therapies should be the first-line therapy, such as mesalamine suppositories, corticosteroid suppositories, or corticosteroid ointment applied directly to the cuff. Biological therapies and small molecule therapies are recommended in refractory cases
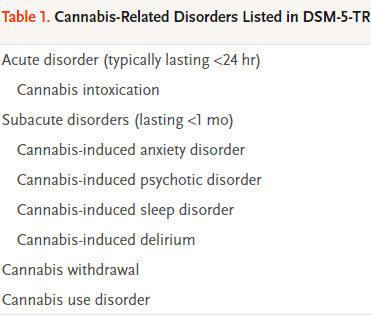
Two recent articles review cannabis-related disorders:
DA Gorelik. NEJM 2023; 389: 2267-2275. Cannabis-Related Disorders and Toxic Effects
Background: “In the United States, an estimated 52.4 million persons 12 years of age or older used cannabis in 2021, representing 18.7% of the community-dwelling population in that age group,5 and 16.2 million persons met the diagnostic criteria for cannabis use disorder, which has as its core feature the use of cannabis despite adverse consequences…Cannabis use poses a global disease burden, albeit substantially less than that posed by other psychoactive substances such as alcohol, tobacco (nicotine), opioids, and stimulants.10 The Global Burden of Disease project calculated that cannabis use in 2016 was responsible for an estimated 646,000 years of healthy life lost to disability.”
Key points:
“Cross-sectional surveys suggest that recent cannabis use increases the risk of motor vehicle crashes by 30 to 40%.26 By comparison, a blood alcohol concentration of 0.08% increases the risk of crashes by 250 to 300%.26“
“Cannabis use disorder, like other substance use disorders, is a chronic, relapsing condition.”
“A substantial reduction or a cessation of cannabis use after heavy or long-term use results in a withdrawal syndrome that is usually mild and self-limiting.39…Common psychological symptoms of cannabis withdrawal include depressed mood, anxiety, restlessness, irritability, decreased appetite, and sleep disturbance. Physical signs and symptoms are less common and include abdominal cramps, muscle aches, tremor, headache, sweating, chills, and weight loss. These signs and symptoms typically begin within 1 to 2 days, peak within 2 to 6 days, and last for several weeks…The prevalence of any withdrawal symptoms is almost 50% in persons who were using cannabis daily.”
Neonatal cannabis exposure: “Pregnant persons who use cannabis expose their neonates to cannabis. Such in utero exposure is associated with increased risk among newborns of having low birth weight, being small for gestational age, and being admitted to the neonatal intensive care unit.”
“Cannabinoid hyperemesis syndrome, a form of cyclic vomiting syndrome that is often accompanied by abdominal pain, occurs during or within 48 hours after frequent and heavy cannabis use.75 Cannabinoid hyperemesis syndrome is a major reason for cannabis-related visits to emergency departments, and it accounts for about 10% of patients with cyclic vomiting syndrome.76 Cannabinoid hyperemesis syndrome is distinguished from cyclic vomiting syndrome by its temporal association with cannabis use, relief with hot baths or showers, and resolution with extended abstinence from cannabis…The symptoms of cannabinoid hyperemesis syndrome are treated with benzodiazepines, haloperidol, and topical capsaicin. “
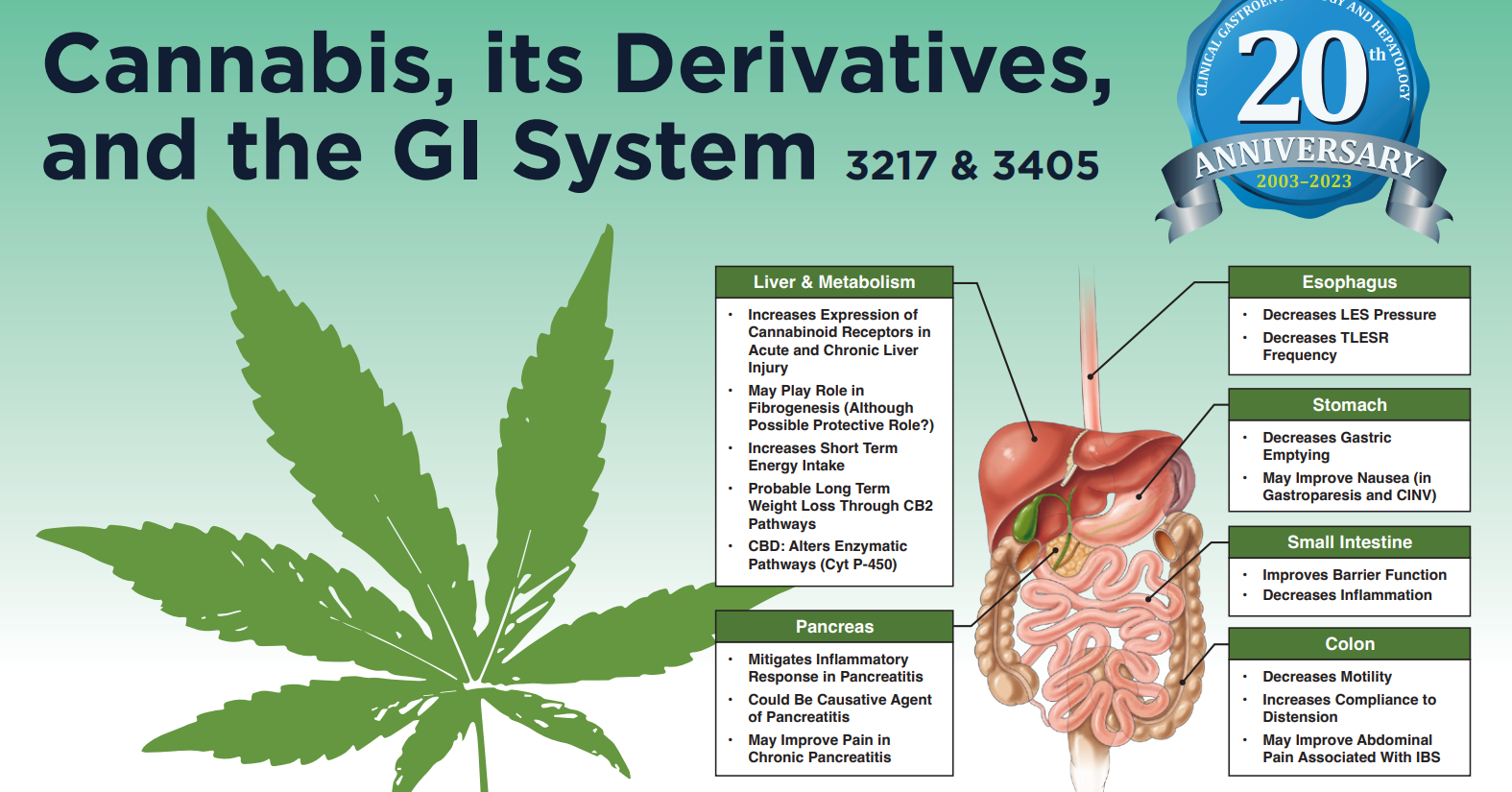
M Camilleri, T Zheng. Clin Gastroenterol Hepatol 2023; 21: 3217-3229. Cannabinoids and the Gastrointestinal Tract This article focuses more on the GI tract effects of cannabinoids.
At a lot of IBD conferences, there is often a lot of focus on health maintenance including discussions on optimizing immunization levels and nutrition. It is often striking how, in comparison, so little attention is focused on emotional health which seems to cause a much greater health burden.
CS Tse et al. Inflamm BowelDis 2024; 30: 150-153. Increased Risks for Suicide, Self-Harm, Substance Use, and Psychiatric Disorders in AdultsWith Inflammatory Bowel Disease: A Nationwide Study in the United States From 2007 to2017
Background: Patients with IBD are also at an increased risk for chronic opioid use, depression, anxiety, sleep disturbance, and disease-related disability (eg, unemployment), all known risk factors for suicide
Methods: This cross-sectional study uses the Nationwide Emergency Department Sample of the Healthcare Cost and Utilization Project (HCUP) as a public domain representing 80% of the U.S. population. This analysis included more than 260 million emergency department visits across the United States from 2007 to 2017.
Key findings:
Inflammatory bowel disease conferred >10-fold risk for suicide deaths, self-harm, substance use, and psychiatric disorders.
The absolute numbers of self-harm rates were low (<1% of all-cause inflammatory bowel disease emergency department visits; total 56 suicide deaths). This amounts to about 5 suicide deaths per year (compared to 0.5 per year for patients with celiac disease.
The risk of self-harm was higher in patients with Crohn’s disease than ulcerative colitis (RR, 3.3; 95% CI, 1.2-5.4), though the suicide risk was not statistically different (RR, 2.3; 95% CI, 0.8-4.5).
From Table 2: RR of self-harm, suicide, psychiatric disorders, and substance use of adults with inflammatory bowel disease compared with celiac disease in the United States from 2007 to 2017. The authors found that rates of self-harm and suicide were the same for patients with celiac disease as the general population (RR 1.0).
My take: Attention to mental health is important component of good care for patients with inflammatory bowel disease.
There is little evidence that we are reducing diagnostic errors despite more lab testing and more imaging. “One of the important reasons for these errors is failure to consider the diagnosis when evaluating the patient.” This, in turn, may be related to brief office visits.
AI support to radiologists for a large mammography study “showed improvement in accuracy with a considerable 44% reduction of screen-reading workload.” The cancer detection rate was 6.1 per 1000 compared to 5.1 per 1000 in the control group.
In difficult NEJM CPC cases, large language AI model (LLM) outperformed clinicians (see slide below).” The LLM was nearly twice as accurate as physicians for accuracy of diagnosis, 59.1 versus 33.6%, respectively.”
“Likewise, the cofounder of OpenAI, Ilya Sutskever, was emphatic about AI’s future medical superintelligence: ‘If you have an intelligent computer, an AGI [artificial general intelligence], that is built to be a doctor, it will have complete and exhaustive knowledge of all medical literature, it will have billions of hours of clinical experience.’ “
My take (borrowed from Dr. Topol): “We are certainly not there yet. But in the years ahead, …it will become increasingly likely that AI will play an invaluable role in providing second opinions with automated, System 2 machine-thinking, to help us move toward the unattainable but worthy goal of eradicating diagnostic errors.”
Seven pediatric patients with perianal Crohn’s disease were treated with mesenchymal stem cells. Key finding: At 6 months, 83% had complete clinical and radiographic healing. This healing rate is higher than “the 50% efficacy reported by the only completed randomized control phase III clinical trial.[ADMIRE study].”
MA Baarslag et al. NEJM 2023; 389: 1790-1796. Severe Immune-Related Enteritis after In Utero Exposure to Pembrolizumab
This case report details severe immune-related gastroenterocolitis after in utero exposure to pembrolizumab, an anti–PD-1 agent; the infant presented at 4 months of life. Extensive testing did not identify any underlying causes of VEO-IBD. This infant required TPN for a short period, but subsequently responded to treatment with glucocorticosteroids and infliximab (with plans to continue until at least 3 years of age). Both programmed death 1 (PD-1) and cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) immune checkpoint inhibitors are negative regulators of T-cell immune function. Inhibition of these targets, resulting in increased activation of the immune system and can result in medication-induced colitis in the patients who take them and potentially in infants exposed to these agents in utero.
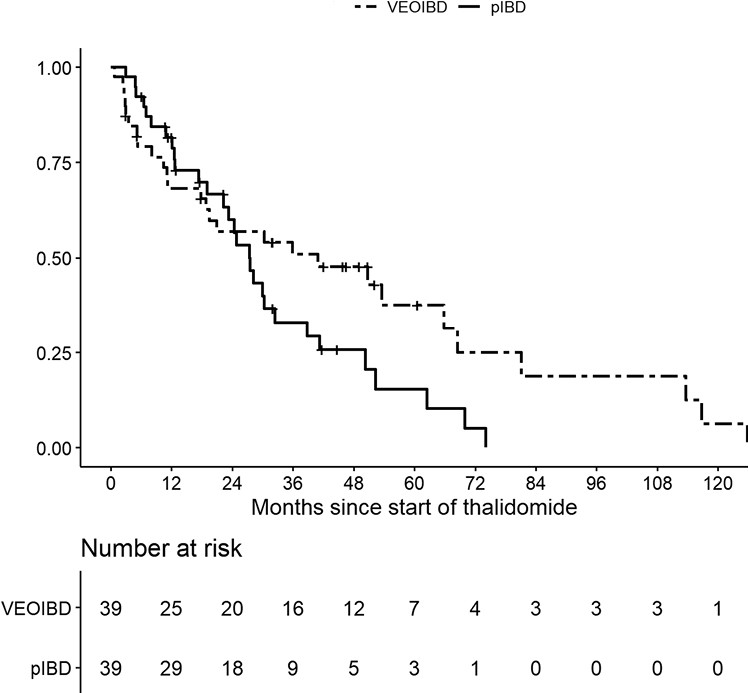
M Bramuzzo et al. Inflamm Bowel Dis 2024; 30: 20-28. https://doi.org/10.1093/ibd/izad018. Efficacy and Tolerance of Thalidomide in Patients With Very Early Onset Inflammatory Bowel Disease
This retrospective study with 39 patients with VEO and 39 patients with pediatric IBD.
Key findings:
The treatment persistence at 1, 2, and 3 years was 68.2%, 57.0%, and 50.9% for VEOIBD patients and 81.7%, 60.0% and 33.0% for pIBD patients, respectively
A significantly higher proportion of VEOIBD patients discontinued therapy due to lack of efficacy (48.2% vs 17.2%; P = .03), while AEs were the main reason for discontinuation in pIBD patients
A significatively lower number of VEOIBD patients experienced AEs compared with pIBD patients (14 [35.9%] vs 30 [76.9%]; P = .0005).
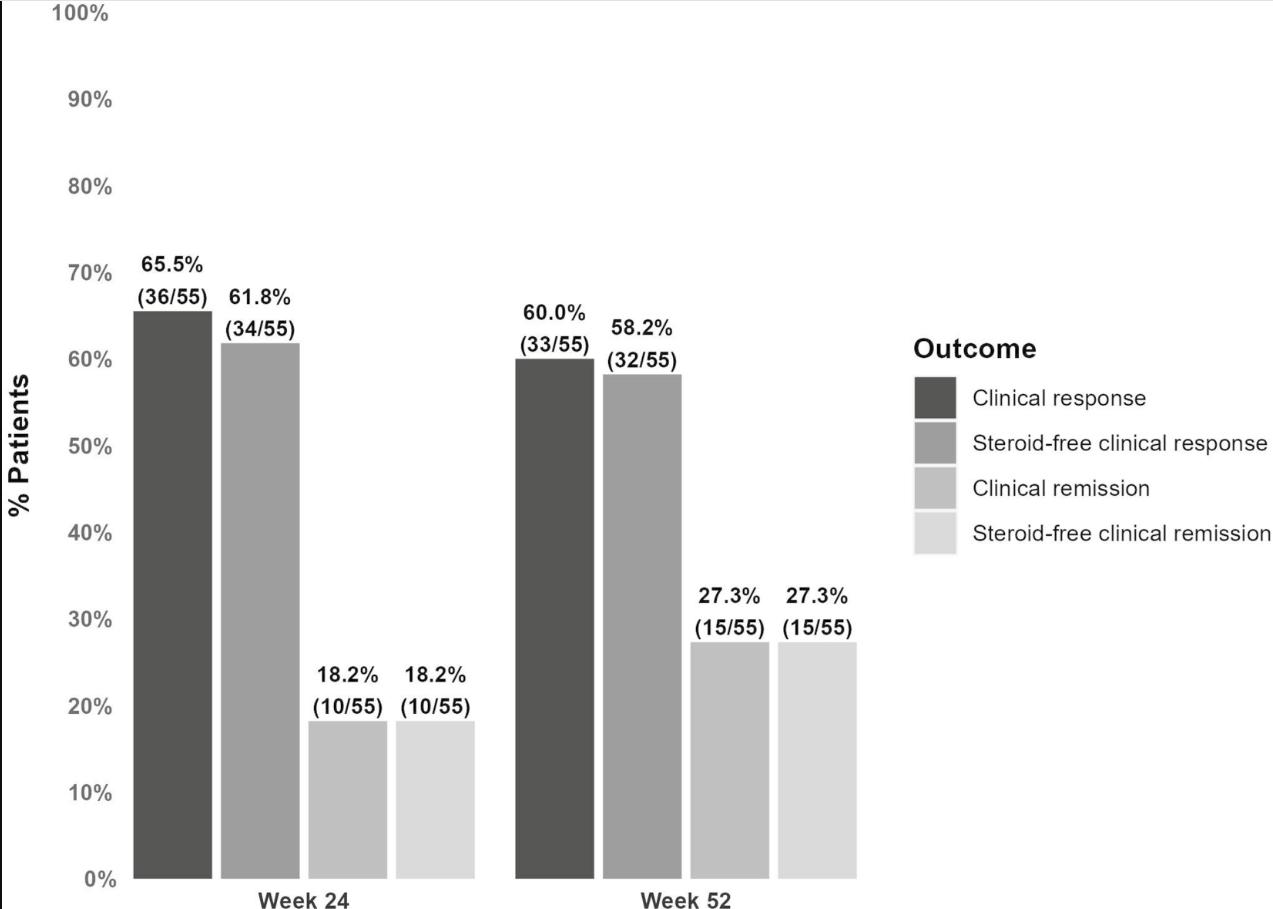
D Alsoud et al Inflamm Bowel Dis 2024; izad315, https://doi.org/10.1093/ibd/izad315. Real-world Effectiveness and Safety of Risankizumab in Patients with Moderate to Severe Multirefractory Crohn’s Disease: A Belgian Multicentric Cohort Study
Methods: Data from consecutive adult CD patients who started risankizumab before April 2023 were retrospectively collected at 6 Belgian centers. A total of 69 patients (56.5% female, median age 37.2 years, 85.5% exposed to ≥4 different advanced therapies and 98.6% to ustekinumab, 14 with an ostomy) were included.
Key findings:
At week 24, 61.8% (34 of 55) and 18.2% (10 of 55) of patients without an ostomy achieved steroid-free clinical response and remission, respectively.
At week 52, these numbers were 58.2% (32 of 55) and 27.3% (15 of 55), respectively. Endoscopic data were available in 32 patients, of whom 50.0% (16 of 32) reached endoscopic response within the first 52 weeks.
Results in patients with an ostomy were similar (steroid-free clinical response and remission, 42.9% and 14.3%, respectively).
20.3% (14 of 69) of patients underwent CD-related intestinal resectionsand 18.8% (13 of 69) of patients discontinued risankizumab during followup (median 68 weeks).
Risankizumab was well tolerated with no safety issues.
Discussion points: “98.6% of patients in the current study were exposed to ustekinumab compared with less than 20% in the registration trials. This indicates that a previous lack or loss of response to the inhibition of the p40 subunit common to IL-12 and IL-23 does not preclude a potential response from subsequent selective inhibition of IL-23. “
My take: This study shows that risankizumab can be effective in refractory patients, even in those who have received similar type medications (eg. ustekinumab).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
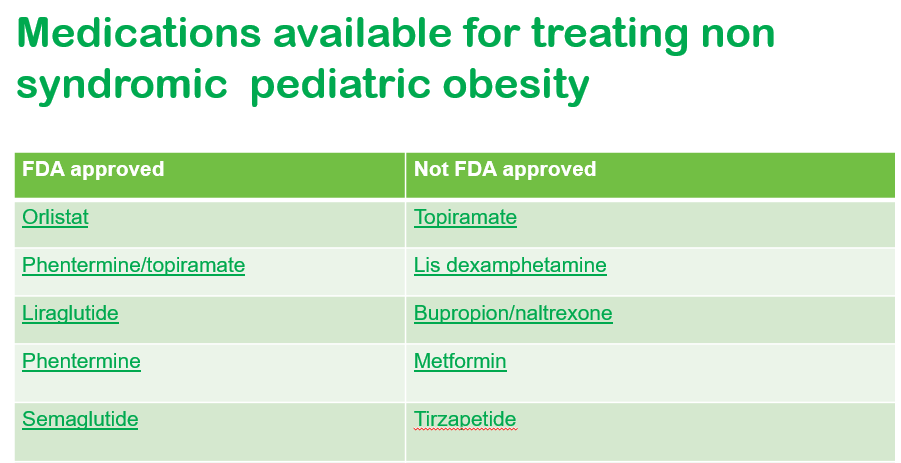
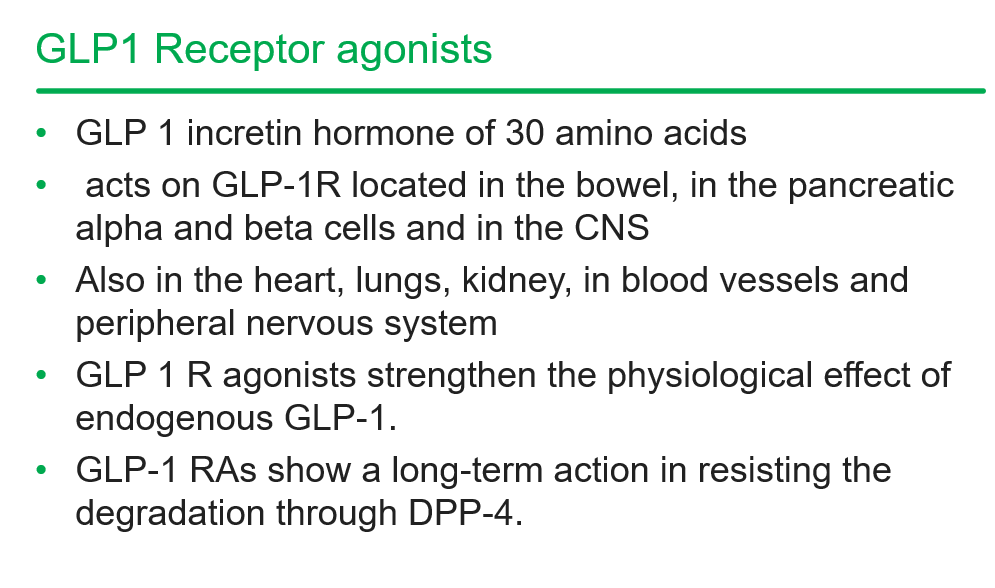
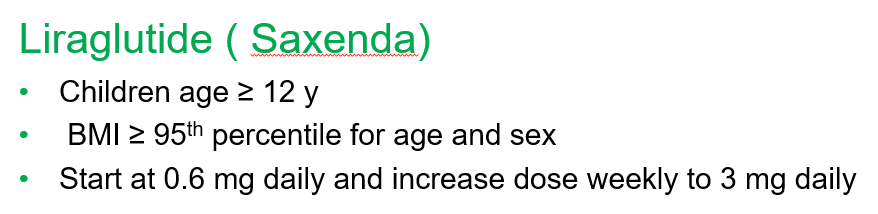
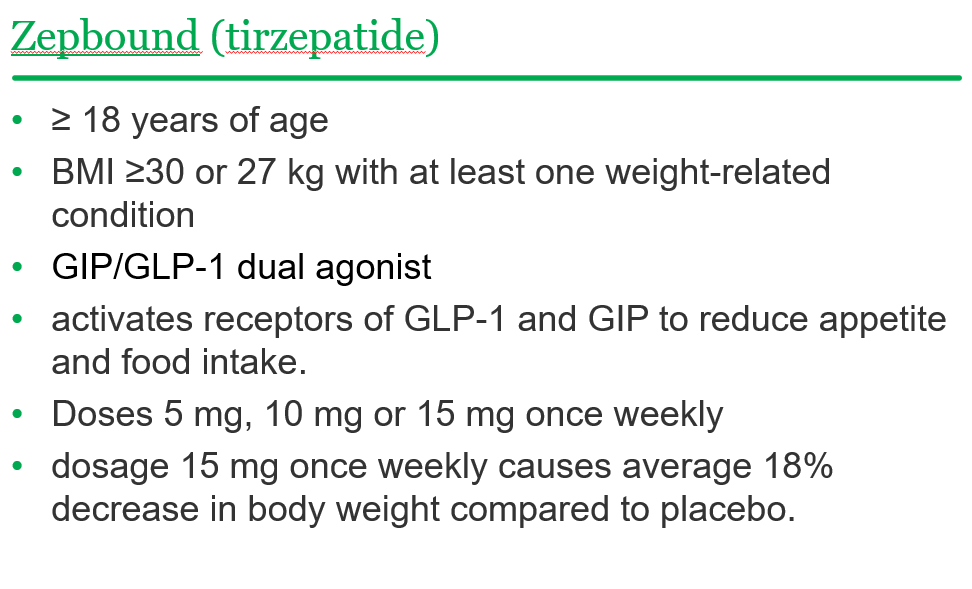
Recently, Dr. Shruthi Arora, an Emory Pediatric Endocrinologist and part of CHOA’s Strong4Life team, provided a terrific review of pediatric obesity pharmacology for our group.
Here are a few slides from Dr. Arora’s lecture:
General points from this lecture:
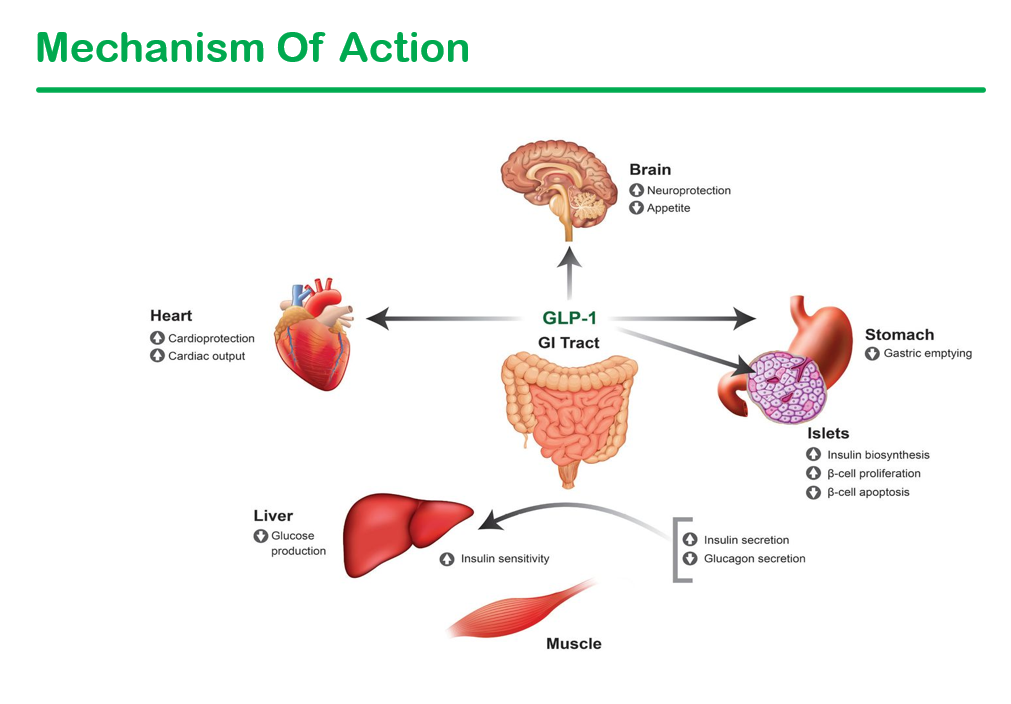
GLP-1 agents are a huge advance but currently limited by affordability (frequently there is a lack of insurance coverage if there is not T2DM) and availability. In addition, most individuals will regain weight loss when these agents are stopped.
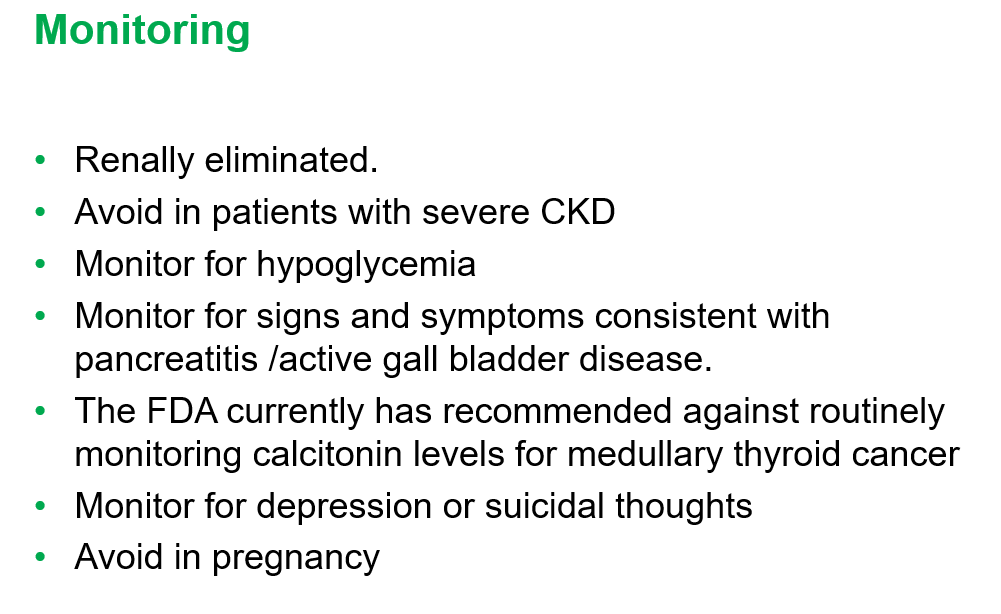
GLP-1 agents are not recommended in the following: patients with gastroparesis, and patients with a personal or family history significant for MEN 2 A /MEN 2 B/ Medullary thyroid cancer
Long-term data is still needed. These agents have been associated with muscle and bone loss; thus, working to assure a good diet is still very important
——————————————————————————
NASPGHAN has a good review/webinar on this topic as well: Pediatric MASLD in the Current Era of Pharmacological and Surgical Obesity Treatment Options. For members, after sign in, you can register and login to this webinar (look under clinical practice tab). This webinar made a lot of useful points (many covered by Dr. Arora too).
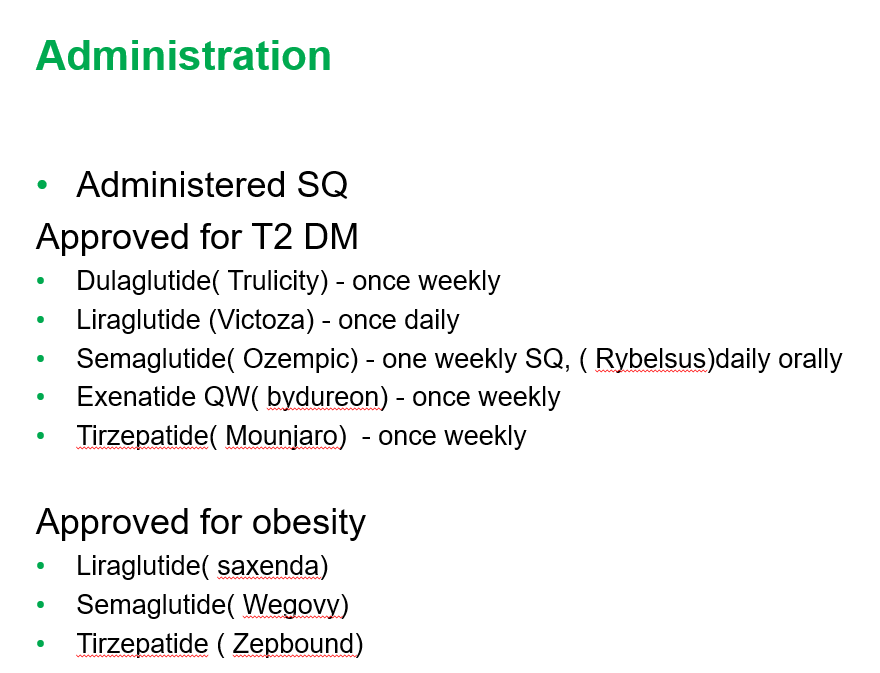
For GLP-1 agents, due to effects on gastric emptying, they are generally held prior to anesthesia. If they are given weekly, then hold 1 week prior to anesthesia. If it is a daily medication, hold for 1 day prior to anesthesia.
Surgery definitely helps improve MASH -though variable responses in patients. SLEEVE gastrectomy is currently the most frequent bariatric surgery
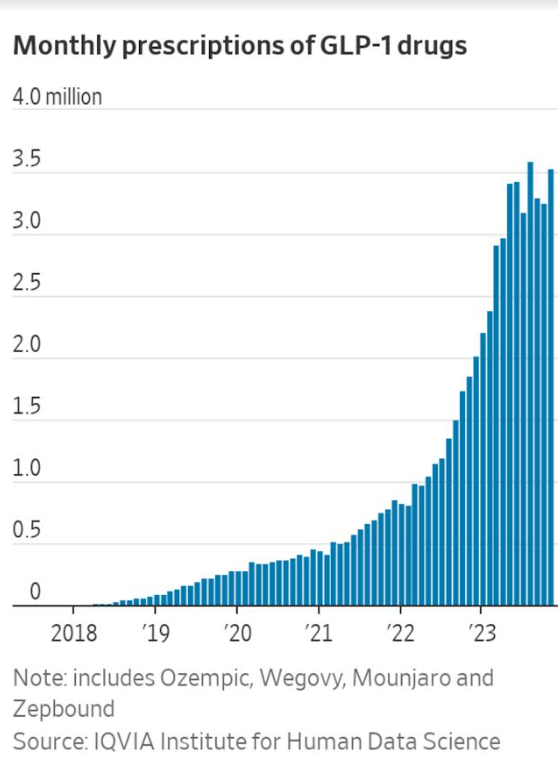
There is trouble getting GLP-1 medications.
Limited knowledge regarding long-term effects of cycling of GLP-1 agents.
Obesity is a long-term disease –>anticipate long-term treatment
The Wall Street Journal recently published a personal account of using the newer obesity medications. Bradley Olson, 1/12/24: A Weight-Loss Drug Changed My Life. Will It Solve My Problem? (behind a paywall). This article discusses the dramatic improvement experienced by the writer along with his concerns about the cost of the medication and potential for rebound when he can no longer afford it. Two of the figures:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.