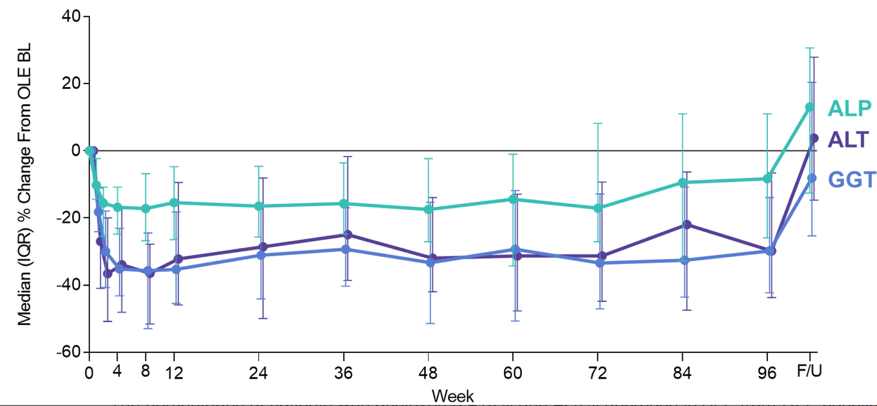
Study: There were 52 subjects enrolled in the phase II study, 47 (90%) continued in the open-label extension phase. Key findings:
At week 96, reductions in serum alkaline phosphatase (median, −8.3%), gamma-glutamyl transferase (−29.8%), alanine aminotransaminase (−29.8%), and aspartate aminotransaminase (−16.7%) occurred, and rebounded after 4 weeks of untreated follow-up. Serum cytokeratin 18 M30 and M65 (which are markers of apotopsis and necrosis)were also reduced in the OLE
My take (from authors): “Whether cilofexor impacts clinically relevant endpoints associated with PSC await the results from the placebo-controlled, phase III PRIMIS study.”
Longitudinal relative change in serum ALP, GGT, and ALT from OLE baseline to week 96 and then 4-week, untreated follow up (F/U).
This article provides a good review of the investment of private equity in gastroenterology practices. Key points:
“In addition to finding that many gastroenterologists were willing to join a PE-backed practice, PE firms found such an investment attractive because of the returns they could earn through consolidating the market.6,33…Dermatology,39 eye care,40,41 fertility,42 orthopedics,43 urology,44,45 and oncology46 are also showing increased PE activity.”
“The effects of PE ownership in gastroenterology are only recently being studied. Notable conclusions include increased costs of services, more visits by new patients, and increased esophagogastroduodenoscopy utilization absent any increase in total number of polyps or tumors removed.50…To increase revenue, one needs to increase either prices or volume of services provided, and it appears as if PE-backed practices are effectively doing both.”
“Increased volume could reflect overutilization of profitable services, unnecessary/low-value care, and/or more effective marketing, among other tactics. Higher prices could relate to more efficient charge capture, higher intensity coding, higher negotiated prices, patients being offered higher-priced services, or other causes.”
A new study finds that private equity firms own more than half of all specialists in certain U.S. markets…The medical groups were associated with higher prices in their respective markets, particularly when they controlled a dominant share, according to a paper by researchers at the Petris Center at the University of California, Berkeley, and the Washington Center for Equitable Growth, a progressive think tank in Washington, D.C. When a firm controlled more than 30 percent of the market, the cost of care in three specialties — gastroenterology, dermatology, and obstetrics and gynecology — increased by double digits...
Nearly 70 percent of all doctors were employed by either a hospital or a corporation in 2021, according to a recent analysis from the Physicians Advocacy Institute...If they could, given their rising costs and how squeezed they feel by insurers, “every independent group would want to increase its fees”…
“This builds the case for strong antitrust tools for these incrementally small but collectively larger consolidation trends,” said Erin Fuse Brown, the director of the Center for Law, Health and Society at Georgia State University.
My take: Private equity’s acquisition of medical practices is likely to drive up healthcare costs without significant improvement in patient outcomes. However, few if any other stakeholders in medical care are incentivized to provide high value care.
A previous study (SEAVUE) has suggested similar efficacy of ustekinumab and adalimumab in biologic-naive patients (post: SEAVUE: Head-to-Head Ustekimumab vs. Adalimumab) with ~60-65% clinical response at 52 weeks and ~30% endoscopic remission.
This current retrospective study sought to obtain ‘real-world’ data comparing anti-TNF agents (95 adalimumab, 61 infliximab) to ustekinumab (n=50). In the anti-TNF group, 44% (n=68) received concomitant immunomodulator therapy. Key findings:
At 3 months, clinical response rates were 86% in anti-TNF groups and 64% in the ustekinumab.
At 12 months, in adjusted multivariate analysis, clinical remission (based on Harvey-Bradshaw Index) was independently associated with the biological therapy received (odds ratio, 2.6 for anti-TNF agent vs ustekinumab;P = .02).
“In our sensitivity analysis, a significant difference in terms of efficacy was only found between infliximab and ustekinumab.”
In those with ileocolonoscopy, endoscopic healing was similar (between 6-18 months): 58% of anti-TNF group and 61% of ustekinumab group.
2% of patients in the anti-TNF group had severe adverse events compared to none in the ustekinumab group; among patients receiving adalimumab, 1 patient had cerebral aspergillosis, 1 had a postinfectious macrophage activation syndrome, and 1 had severe folliculitis needing abscess drainage.
Drug persistence at 12 months was 87% in anti-TNF group and 88% in ustekinumab group.
The discussion notes that ‘real-world’ data is important as only ~30% of patients in a regular practice would fulfill the criteria to be included in clinical trials. However, in this retrospective (non-randomized) study, there were differences in the patient population that could affect response to treatment, including a higher rate of smokers in the anti-TNF group (29% compared to 12% in the ustekinumab group).
My take: While anti-TNF therapy, particularly infliximab, may be a little better based on clinical remission, the most objective marker of efficacy, endoscopic healing, was similar. Thus, it is not clear if anti-TNF therapy is more effective than ustekinumab. To achieve optimal results, many in the anti-TNF group received immunomodulator cotherapy and dose escalation.
Joel Andres, Chef & Philanthropist, World Central Kitchen
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
The pooled placebo response rate was 29.3% (95% CI, 23.7%–35.2%) in 23 trials (n=1011)
Pooled placebo response rates were higher in idiopathic compared with diabetic gastroparesis (34.2% vs 28.1%).
Pooled responses were also higher in RCTs of shorter duration (<4 weeks, 32.6% vs ≥9 weeks, 23.2%) and in trials that did not use validated symptom questionnaires (31.2% vs 27.4%)
Adverse events occurred in 33.8% (95% CI, 26.4%–41.8%) of patients with placebo, in 27 trials, and were less common in idiopathic compared with diabetic gastroparesis (17.9% vs 43.4%)
My take: The relatively high placebo response joins the list of factors which make the management of gastroparesis difficult. This list includes trouble with diagnosis/variable results with gastric emptying studies and limited response to current treatments.
This retrospective cohort study identified 1037 patients with Crohn’s disease who underwent ileocecal resection (ICR). Only 5.4% were younger than 18 yrs at the time of surgery. In this cohort, 278 (26%) received a biologic agent as prophylaxis to prevent recurrence with 80% receiving an anti-TNF agent. In those receiving an anti-TNF agent, 35% were started on therapy within 4 weeks of surgery and 65% were started between 4 and 12 weeks. Recurrence was defined by endoscopy (≥ i2b Rutgeerts score) or radiography (active inflammation in neoterminal ileum). Key findings:
After adjusting for factors associated with postoperative recurrence (POR), compared with no biologic prophylaxis, the initiation of an anti-TNF agent (n=223) within 4 weeks following an ICR was associated with a reduction in POR (adjusted hazard ratio, 0.61).
Prophylaxis after 4 weeks following an ICR or with vedolizumab or ustekinumab was not associated with a reduction in POR compared with those who did not receive prophylaxis –though sample size with vedolizumab (n=27) and ustekinumab (n=28) was very limited
Most patients receiving biologic prophylaxis had prior anti-TNF exposure including 73% of the anti-TNF group, 96% of the vedolizumab group, and 93% of the ustekinumab group.
In their discussion, the authors note that their findings reinforce previous studies which showed beneficial effects of anti-TNF therapy for POR, including the PREVENT trial. This randomized controlled trial with infliximab initiation within 45 days postoperatively in high risk individuals reduced endoscopic recurrence at 18 months (22.4% compared with 51% in placebo group).
My take: Anti-TNF therapy, even in those with prior exposure, likely improves outcomes in patients with Crohn’s disease following ileocecal resection. This study indicates that starting therapy within the first 4 weeks is more beneficial.
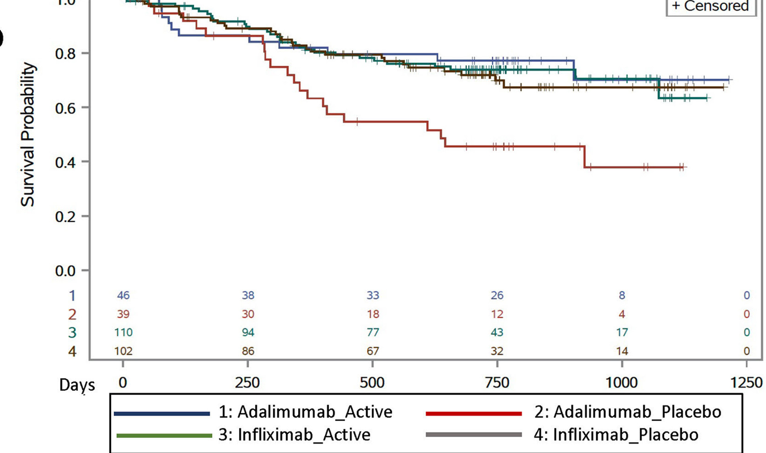
This study enrolled 297 children with Crohn’s disease starting anti-TNF therapy. Patients initiating infliximab or adalimumab were randomized in 1:1 allocation to methotrexate or placebo and followed for 12–36 months.
Methotrexate dosing: For those in the active arm, oral methotrexate was administered with a weekly dose of 15 mg for children ≥40 kg, 12.5 mg for children 30 to <40 kg, and 10 mg for children 20 to <30 kg. All participants received pretreatment with ondansetron 4 mg (or placebo) to prevent nausea and folic acid (1 mg/d).
Key findings:
For treatment failure: among infliximab initiators, there were no differences between combination and monotherapy (hazard ratio, 0.93; 95% CI, 0.55–1.56)
For treatment failure: among adalimumab initiators, combination therapy was associated with longer time to treatment failure (hazard ratio, 0.40; 95% CI, 0.19–0.81).
A trend toward lower anti-drug antibody development in the combination therapy arm was not significant (infliximab: odds ratio, 0.72; 95% CI, 0.49–1.07; adalimumab: odds ratio, 0.71; 95% CI, 0.24–2.07).
In our study, only 38% of participants underwent colonoscopy during follow-up (41% had calprotectin measurement).
My thoughts on this study:
The COMMIT study Gastroenterol 2014; 146: 681-88 found similar findings with regard to infliximab (see blog post: Digging into the COMMIT Study). In this study, MTX with IFX was not superior to monotherapy but did result in fewer antibodies and better levels.
With IFX the benefits of combination therapy seem to be minimal in those with good therapeutic levels, S Lega et al. Inflamm Bowel Dis 2019; 25: 134-41, JF Colombel et al. Clin Gastroenterol Hepatol 2019; 17: 1525-32: (blog posts: Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD?; Combination Therapy Study Points to Central Role of Adequate Drug Levels). In the discussion, the authors note that intensive therapeutic drug monitoring may contribute to better outcomes with infliximab compared to adalimumab. “The observed benefit of combination therapy among adalimumab users was demonstrated in the setting of standard of care TDM. Of note, anti-TNF dose or interval adjustment and TDM were more frequent in infliximab-treated patients than adalimumab-treated patients, likely due to ease of obtaining trough levels during infusions and more flexible dosing.”
My take: Given the increased difficulty monitoring the kids on adalimumab, they are probably better off on dual therapy. My suspicion, though, is that if they had optimized levels, the benefit of dual therapy is probably small and would mirror the findings with IFX.
This position paper regarding dilatation of strictures in Crohn’s disease provides mostly vague advice.
Here are a few examples:
Imaging: “The need for fluoroscopy is dependent on the stricture phenotype and the treating team…The advantage of live imaging is obvious: it provides greater certainty of balloon position and dilatation success; however, it is difficult and impractical in some centers…In simple strictures, where balloon passage and deployment can be performed with reasonable confidence under direct vision,…it is reasonable to dispense with imaging.”
Dilatation Size: “In the recent pediatric case series…a median of 15 mm was used” as a target dilatation….”It is wise to set reasonable goals for dilatation…Inherited wisdom recommended limiting esophageal dilatation to no more than 3 mm per session. However,…subsequently challenged in several studies demonstrating safe dilatation up to 5 mm per session…As an informal rule, the authors limit dilatation to 2 balloon sizes per session which roughly translates to 5-6 mm. An alternative approach…is to dilate to a maximum of three times the initial stricture diameter; however, neither of these approaches are based on any robust data.”
The main clear cut recommendations are to obtain careful consent, expecting a complication rate of ~4% (eg. bleeding, sepsis, perforation), and to have surgical backup.
My take: This “position paper” offers very few positions on management advice and gives little clear guidance in terms of dilating strictures in Crohn’s disease.
Methods: This was a a phase 3, double-blind, placebo-controlled trial of patients with chronic constipation, who were randomized to receive either a vibrating or placebo capsule, once daily, 5 days a week for 8 weeks. The primary efficacy end points were an increase of 1 or more complete spontaneous bowel movements per week (CSBM1 responder) or 2 or more CSBMs per week (CSBM2) from baseline during at least 6 of the 8 weeks
Key findings:
A greater percentage of patients receiving the vibrating capsule achieved both primary efficacy end points compared with placebo (39.3% vs 22.1%, P = .001 for CSBM1; 22.7% vs 11.4% P = .008 for CSBM2).
Spontaneous bowel movements per week, adjusted mean change: 1.40 vs 1.24 per placebo (0.16 per week difference)
The capsule used is 24 mm x 11 mm and includes a motor for vibrations, a battery, a computer chip and a latex-free plastic shell. The control group had received a dissolvable sham capsule.
I looked up cost of this new treatment and it is approximately $89/month which equates to $139 price per poop (PPP). To my knowledge, the PPP is a new metric –I have not seen it previously. For the vibrating capsule, I derived this figure by dividing the monthly cost into a weekly cost and dividing it by 0.16 (mean difference in weekly stooling with vibrating capsule). The PPP may be competitive with some of the constipation medications which cost in the range of ~$500 per month on GoodRx (like prucalopride and linaclotide) but is much more costly than senna products which can be purchased for ~$5/month.
My take: The vibrating capsule is an expensive way to help with constipation