Methods: The study used data from the Fragile Families and Child Wellbeing Study, a longitudinal birth cohort study of children born in 20 US cities. Study outcomes were “based on age-15 interviews with the focal children and their caregivers with sample sizes ranging from 2088 to 2327 across outcomes. The relationship between CPS contact and child wellbeing was estimated using the propensity score method of inverse probability of treatment weighting.”
Key findings:
“Despite a federal mandate to improve child wellbeing, we found no evidence that contact with the child welfare system improves child outcomes. Rather, CPS contact was associated with worse mental health and developmental outcomes” including associated increases in smoking (88% increase), in being expelled from school (18% increase), in depression (7.5% increase, and in anxiety (6.9% increase).
My take: While protecting children and reporting abuse/neglect are mandated, it is not clear that involvement of CPS results in better outcomes.
E Tobin-Tyler. NEJM 2023; 388: 1345-1347. Courts’ Disregard for Women’s Health and Safety — Intimate Partner Violence, Firearms, and “History and Tradition”
A few excerpts:
In June 2022, the Supreme Court issued its opinion in New York State Rifle & Pistol Association v. Bruen, which left the door open for constitutional challenges to virtually any state or federal firearm restriction. One of these restrictions is a federal law passed in 1994 as part of the Violence Against Women Act (VAWA) that makes it unlawful for people subject to certain domestic violence–related restraining orders to possess a firearm or ammunition for the duration of the order.
Writing for the majority in Bruen, Justice Clarence Thomas struck down New York’s restrictions on who may carry a firearm in public. In doing so, he declared that a government arguing in support of a restriction on firearm possession has the burden of showing that its regulation “is consistent with the Nation’s historical tradition of firearm regulation.”..
On the heels of the Supreme Court’s decision in Bruen, a federal district judge on November 10, 2022, held in United States v. Perez-Gallan that the VAWA’s restriction on firearm possession by people subject to restraining orders is unconstitutional…
Searching for relevant laws from the 18th and 19th centuries to justify current laws protecting people who have experienced IPV (intimate partner violence) obscures the fact that married women weren’t even considered legal subjects until the late 19th century. Instead, they were understood to be the property of their husbands.1 Black women who were enslaved, married or not, had no legal rights. “Wife beating” did not become illegal in some states until the late 19th century…
In Rahimi, the court applied Bruen’s “history and tradition” analysis to a case involving a person who not only was subject to a restraining order because he had allegedly assaulted his ex-girlfriend, but also had been involved in incidents in which he had fired a gun at people and at a constable’s car…The court determined that under Bruen’s analysis, there is no reason to consider the potential consequences for people experiencing IPV of permitting their abusers to possess guns.
My take: Deciding gun ownership laws solely on the basis of ‘history and tradition’ is incredibly stupid. Research shows that restriction of access to firearms by domestic abusers results in lower rates of gun deaths. This supreme court will allow anyone to possess a firearm, except those in their vicinity.
Related article: The Hill (5/11/23): Federal judge rules adults ages 18-20 cannot be blocked from purchasing handguns. “A federal judge in Virginia has ruled that federal laws prohibiting 18-to-20-year-olds from getting handguns at federally licensed firearms dealers are unconstitutional…The judge concluded that the Second Amendment’s “right of the people to keep and bear Arms” applies to people in that age group. “Because the statutes and regulations in question are not consistent with our Nation’s history and tradition, they, therefore, cannot stand,” Payne wrote.
Also, I want to give a shout out to Ajay Kaul (who completed his training in Cincy one year after I did) and his recent Bowel Sounds Podcast. Ajay is a terrific person. This was a good review on Achalasia and a reminder of the improvements in motility testing. A good clinical pearl was to ask anesthesiology to intubate patients with suspected achalasia to protect their airway.
My 35 years living with two different donor hearts (I was 25 at the time of the first transplant) — finishing law school, getting married, becoming a mother and writing two books — has felt like a quest to outlast a limited life expectancy. With compulsive compliance, I adhered to the strictest interpretation of transplant protocols. I honored my gifts of life with self-discipline: not one pat of butter; not one sip of alcohol; running mile after mile hoping to stave off vasculopathy, an insidious artery disease that often besets transplanted hearts within about 10 years...
But now I lower my chin and whisper the words malignant … metastatic … lungs … terminal. It is the end of the road for my heart and me…
Organ transplantation is mired in stagnant science and antiquated, imprecise medicine that fails patients and organ donors. And I understand the irony of an incredibly successful and fortunate two-time heart transplant recipient making this case, but my longevity also provides me with a unique vantage point...
Over the last almost four decades a toxic triad of immunosuppressive medicines — calcineurin inhibitors, antimetabolites, steroids — has remained essentially the same with limited exceptions. These transplant drugs… cause secondary diseases and dangerous conditions, including diabetes, uncontrollable high blood pressure, kidney damage and failure, serious infections and cancers...
Transplantation is no different from lifelong illnesses that need newer, safer, more effective medicines. Improvements in drug regimens are needed for lupus, Parkinson’s and a host of others. The key difference is that only in transplantation are patients expected to see their disease state as a “miracle.” …But this narrative discourages transplant recipients from talking freely about the real problems we face and the compromising and life-threatening side effects of the medicines we must take.
This “gratitude paradox,” as I’ve come to think of it, can manifest itself throughout the transplant professional communities as well. Without vigorous pushback, hospitals and physicians have been allowed to set an embarrassingly low bar for achievement.
My take: Though organ transplantation has extended lives, this touching first-hand account outlines important obstacles/challenges that transplant medicine continues to face. For pediatric providers, the article is even more sobering as good outcomes need to last even longer.
From Roger Mills:The procedure is not a cure, but a trade. Patient and physician agree to manage a short-term life-threatening illness by substituting a long-term life-threatening illness — immunosuppression…I take issue only with her understandably harsh words about “stagnant science and antiquated, imprecise medicine that fails patients and organ donors.” Early on, many thought the immune response would yield to targeted therapies using relatively nontoxic small molecules. But experience has taught us that managing the immune response is like peeling back layers of an onion. There are more layers than we ever dreamed of, and each one brings more tears.
From Judith Hale: Here is another story: I’m a healthy, happy 74-year-old who received a heart transplant at the age of 56. I live a normal life: I walk at least two miles a day, cross-country ski in the winter, and tend my garden the rest of the year. I’m not on any special diet: I eat butter and drink an occasional glass of wine with dinner. I have virtually no side effects from the medications.I couldn’t be more grateful for the advances in medical science that have, so far, given me 18 healthy years of life.
From Ronald Kalen: In fact, the advances of transplant medicine have been remarkable given the complexity of the immune system. It is not a trivial problem for research. Dedicated scientists have spent careers in prolonging the life of the transplanted organ, as well as the life of the person receiving that organ, and are as aware as Ms. Silverstein of the “deeply entrenched problems” that remain. Their research is not “mired in stagnant science and antiquated, imprecise medicine that fails patients and organ donors.”
In this prospective study (n=198), the authors examined lipid profile changes at week 10 in patients starting IBD medications: corticosteroids, thiopurines, methotrexate, anti-TNF-α agents, vedolizumab, ustekinumab, and tofacitinib.
Key findings:
Relative increases in total cholesterol, HDL-c, and LDL-c were significant after prednisone (+26%, +31%, +12%) and tofacitinib therapy (+20%, +25%, +26%), respectively
No changes were observed in other drug classes
Findings did not correlate with calprotectin or CRP values, likely indicating a direct medication effect
My take: Recent studies have provided some reassurance regarding tofacitinib and the risk of major adverse cardiovascular events (MACEs) (see posts below). Nevertheless, it seems prudent to monitor lipids in patients receiving JAK inhibitors.
The Oro Valley/Tucson Loop shared use bike path extends over 130 car free miles throughout unincorporated Pima County, Marana, Oro Valley, and Tucson. We managed a 40 mile bike trip.
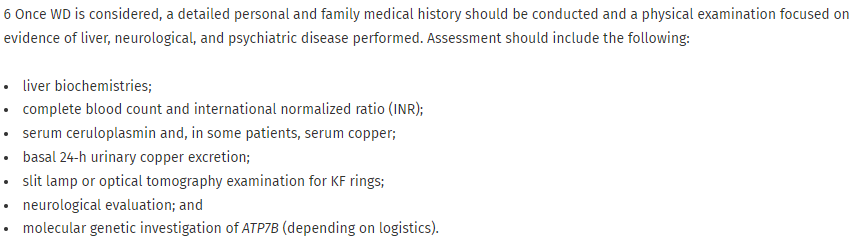
This article is an excellent review of Wilson disease (WD). It reviews clinical manifestations, disorders with overlapping findings and recommendations for diagnosis/management. “This executive summary provides a condensed overview, including the clinical algorithms, tables, and full complement of guidance statements.” Though this ‘summary’ is a lengthy publication, “the full Guidance document with comprehensive text, complete references, and supplementary materials (“A Multidisciplinary Approach to the Diagnosis and Management of Wilson Disease: 2022 Practice Guidance on Wilson Disease from the American Association for the Study of Liver Diseases”) is available on the American Association for the Study of Liver Diseases (AASLD) website (https://doi.org/10.1002/hep.32801).”
Some of the recommendations:
The Leipzig score for diagnosis of Wilson disease may aid in diagnosis
My take: This is a useful guidance and the tables/algorithms should help with both diagnosis and treatment adjustment. In my limited experience with WD, I have had a lot of difficulty with adherence to treatment in the small sample of patients under my care.
In this multicenter retrospective cohort (n=42), the authors examined the efficacy and safety of fecal microbiota transplantation (FMT) in immunocompromised (IC) children with Clostridioides difficile infection (CDI). Etiology of IC included: solid organ transplantation (18, 43%), malignancy (12, 28%), primary immunodeficiency (10, 24%), or other chronic conditions (2, 5%)
Key findings:
23 (55%) of FMT was delivered via colonoscopy, 17 (40%) were delivered via enteric tube, and 2 (5%) via capsule
Success rate was 79% after first FMT and 86% after 1 or more FMT.
There were serious adverse events (SAEs) in 13 out of 42 (31%) patients; 4 (9.5%) of which were likely treatment-related (all patients recovered). These events included cecal perforation, aspiration pneumonitis, diarrhea and fever. Given retrospective design of study, AEs were likely underreported
My take: Though there are the potential for significant adverse effects, FMT is effective in a high percentage of immunocompromised children with CDI.
Methods: This population study assessed all confirmed cases of BA, from January 2020 to December 2021 across the 3 UK pediatric liver centers originating from England and Wales. Data was then compared to the incidence of confirmed BA cases from January to December 2017, 2018, and 2019.
Key findings -BA cases:
2017: 16
2018: 13
2019: 18
2020: 8
2021: 12
This difference was significant in a two-sided t test for 2020 (P = 0.035) but not for 2021 (P = 0.385)
The authors note that new BA diagnoses were reduce among Danish centers as well. In their discussion, the authors discuss the possibility of missed diagnosis versus an actual drop in BA cases. The later is intriguing due to concerns that perinatal infections could trigger BA.
My take: This study provides a piece of a puzzle regarding the etiology of BA, indicating a good likelihood of environmental/infectious etiologies as a trigger.
Methods: Participants with biliary atresia from the Childhood Liver Disease Research Network, in a prospective observational cohort, were included if they had normalized bilirubin levels 6 months after KP and stored serum samples from the 6‐month post‐KP clinic visit.
Key Findings:
The ≤40 μmol/L group (n=43) had a 10‐year cumulative incidence of liver transplant/death of 8.5% compared with 42.9% for the >40 μmol/L group (n=94) (p = 0.001).
At 2 years of age, the ≤40 μmol/L group had significantly lower total bilirubin, aspartate aminotransferase, alanine aminotransferase, gamma‐glutamyltransferase, bile acids, and spleen size, as well as significantly higher albumin and platelet counts.
In addition, during 734 person‐years of follow‐up, those in the ≤40 μmol/L group were significantly less likely to develop splenomegaly, ascites, gastrointestinal bleeding, or clinically evident portal hypertension.
The 137 patients included in this study were only a small fraction of the 756 children enrolled in these studies. 232 children failed to achieve normalized serum bilirubin levels by 6 months following KP, 279 children did not have a 6‐month post‐KP serum bilirubin value, and 108 children did not have serum available for bile acid testing.
My take: Only a fraction of children with BA normalize their bilirubin by 6 months after Kasai procedure. In those with normalized bilirubin (T bilirubin <1.5 mg/dL or conjugated <0.2 mg/dL), elevated serum bile acid levels indicate a high risk for progressive liver disease.
Antetokounmpo, after being asked if he considered the past season a failure:
Do you get a promotion every year at your job? No, right? So every year, your work is a failure? No. Every year, you work towards something, which is a goal: It’s to get a promotion, to be able to take care of your family, provide a house for them, or take care of your parents. It’s not a failure, it’s steps to success. There’s always steps to it. Michael Jordan played for 15 years and won 6 championships. The other 9 years were a failure? That’s what you’re telling me.
There’s no failure in sports. There’s good days, bad days, some days you are able to be successful, some days you’re not, some days it’s your turn, some days it’s not your turn. That’s what sport’s about. You don’t always win, some other people are gonna win. And this year, someone else is gonna win. Simple as that.
So 50 years from 1971-2021 that we didn’t win a championship, it was 50 years of failure? No it was not, there were steps to it, and we were able to win one, hopefully we can win another one.
Real Madrid manager Carlo Ancelotti’s reaction:
What Antetokounmpo said was fantastic … Failure is when you don’t try to do something as well as you can. When you try to do your best, you have a clear conscience, and that’s never a failure, not just in sport but in life.
My take: I like Giannis’ response so much (there’s a 2 minute video at the link). His sentiments align with my beliefs. If/when I work hard, this often leads to good outcomes. However, even if the outcome is not what I wanted, I have no regrets.
“When You Reach for the Stars You May Not Quite Get One, But You Won’t Come Up With a Handful of Mud Either” – Leo Burnett