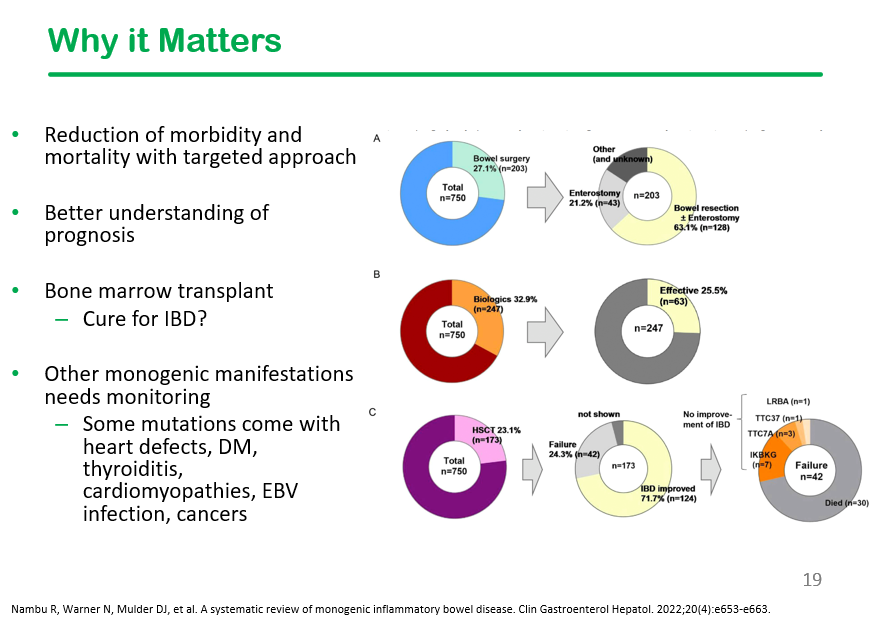
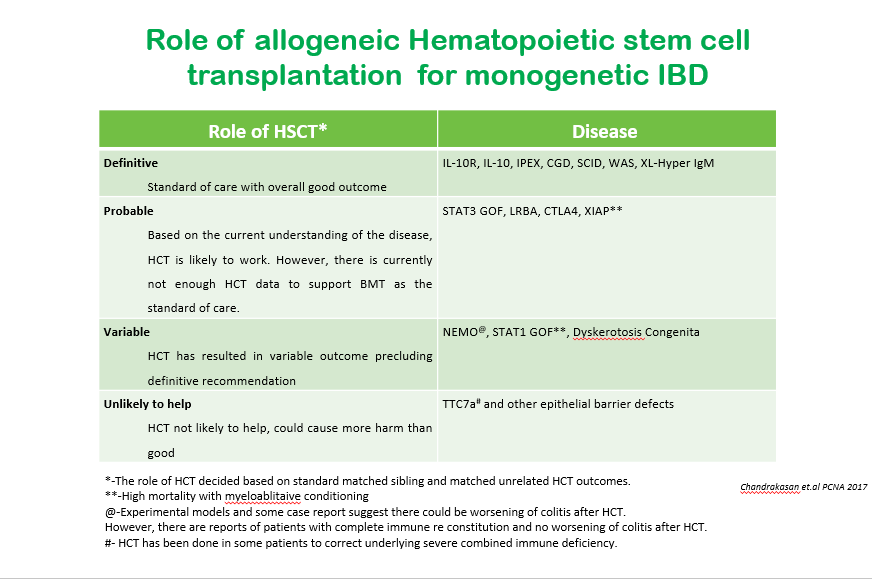
At our center, we are fortunate to work with an immune dysregulation clinic (Dr. Shanmuganathan Chandrakasan, Dr. Taylor Fitch) that helps sort out patients with inflammatory bowel disease with underlying monogenetic disorders. This is very important as specific treatments, including hematopoietic stem cell transplants (HCST), may be needed. The likelihood of an underlying monogenetic disorder is much more frequent in the VEO population. A recent talk on this topic by Taylor Fitch was given to our group. Here are some of the slides:
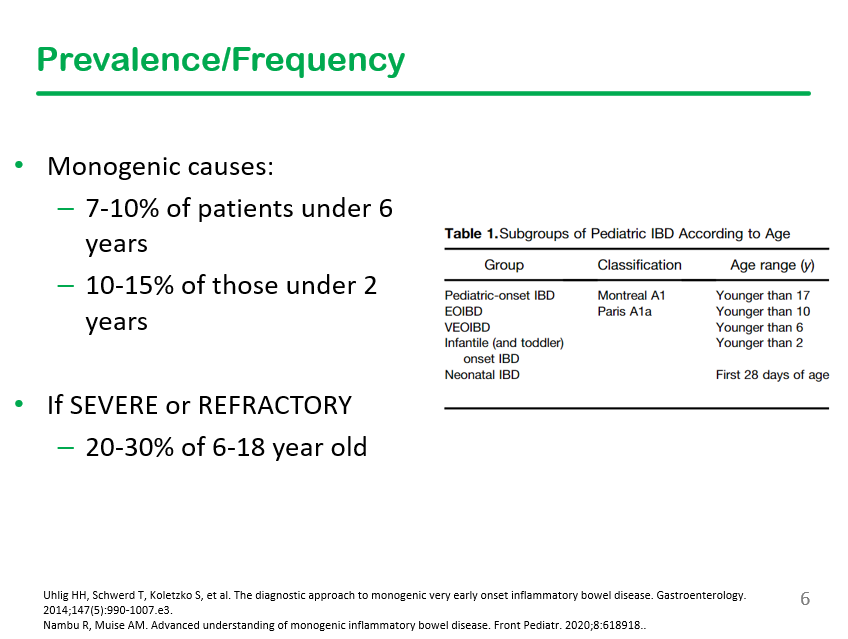
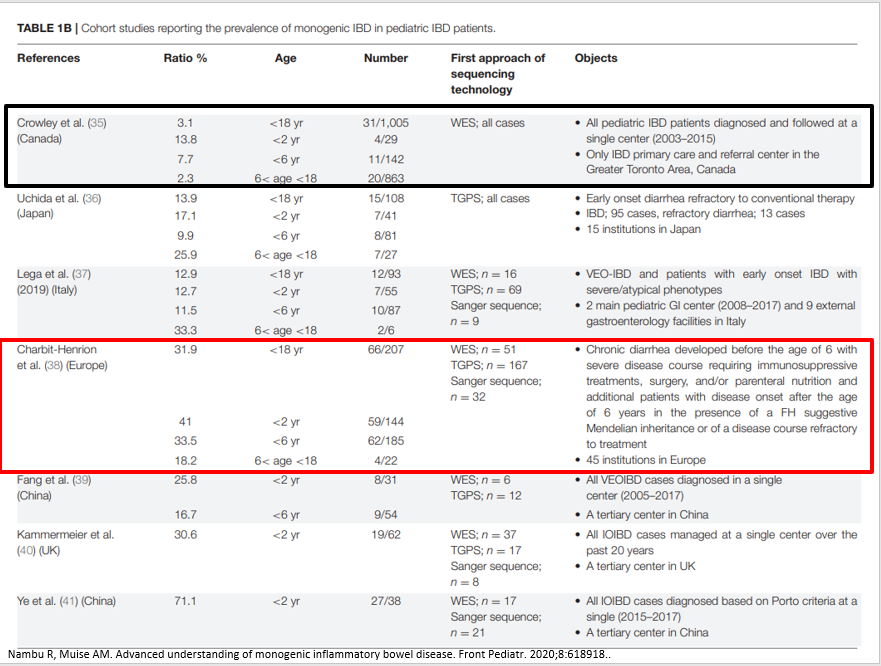
Generally, about 2% of those older than 6 years of age have monogenetic disorders, but it is much higher in those with severe or refractory disease.
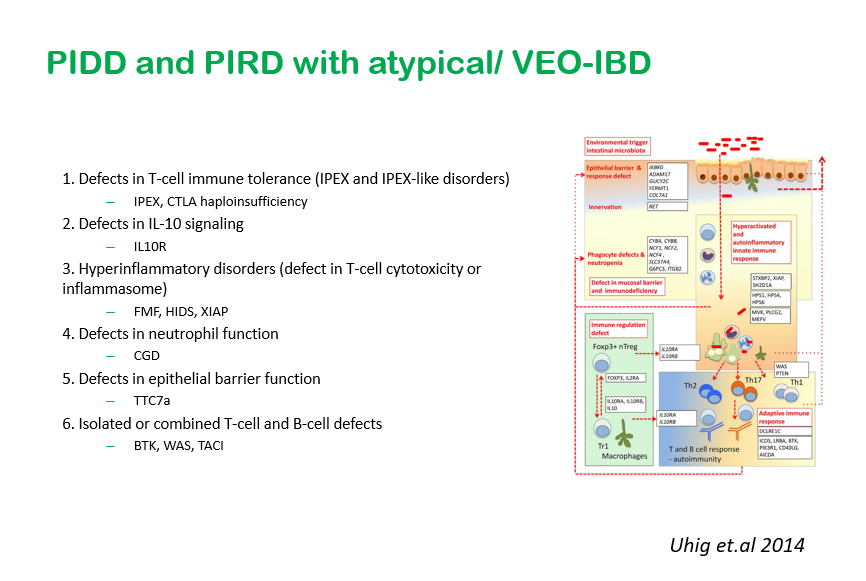
This slide shows six major categories of immune defects.
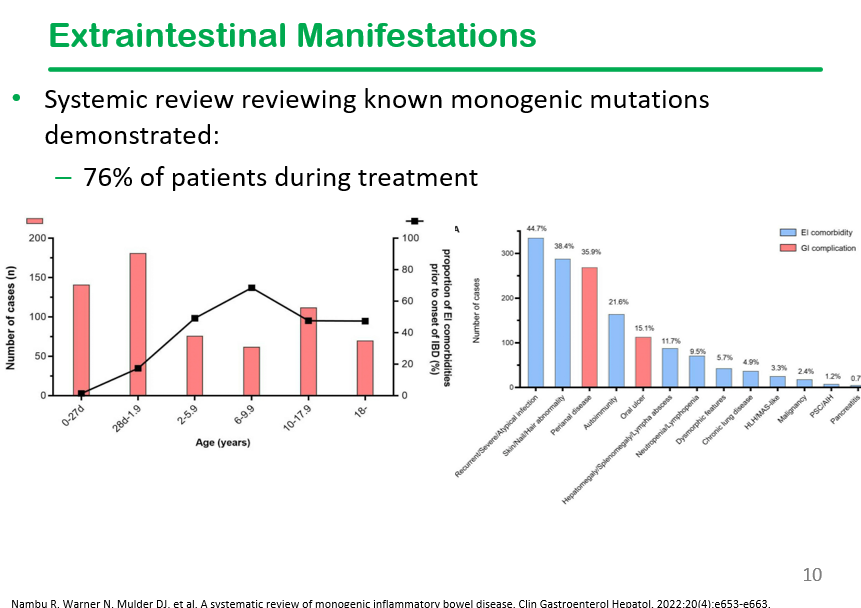
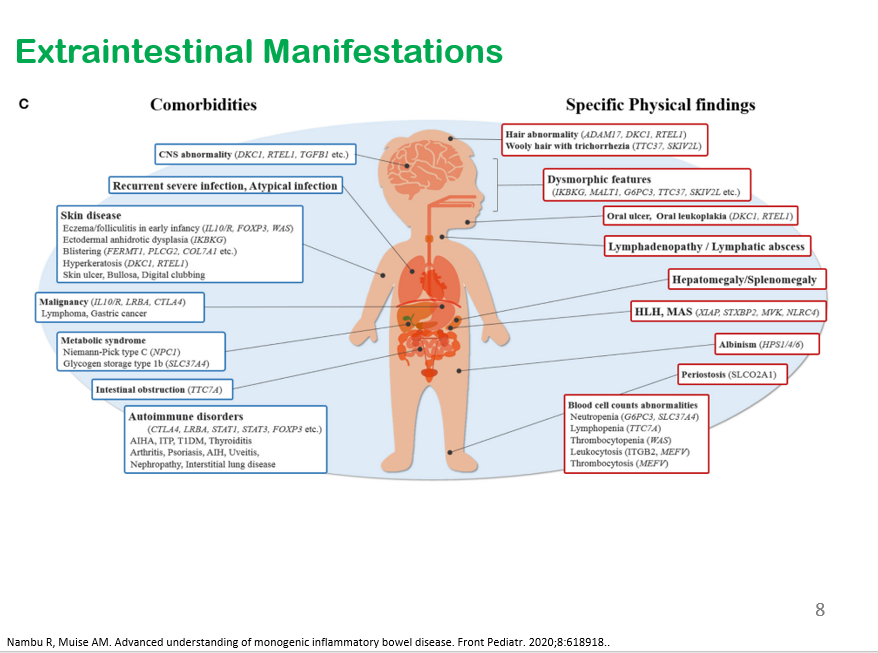
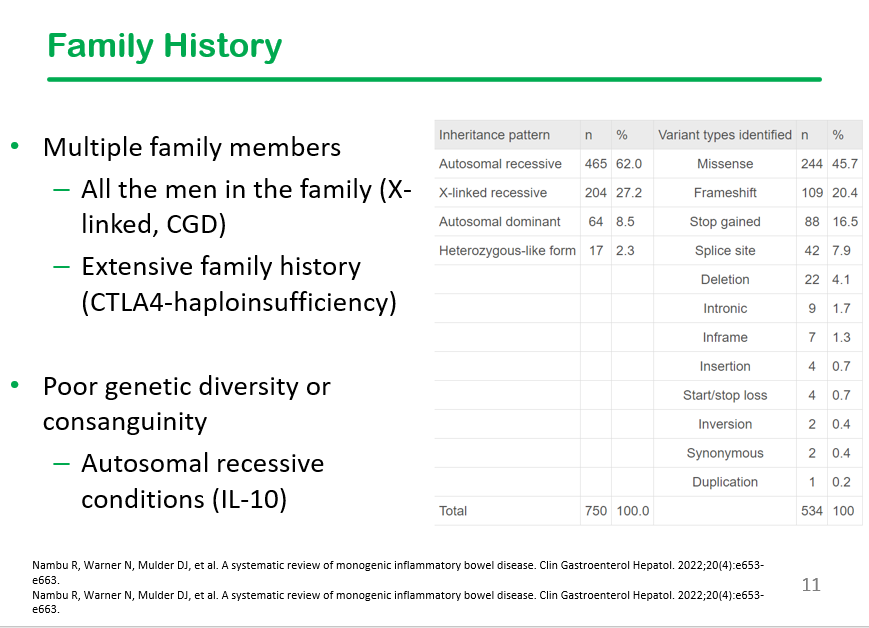
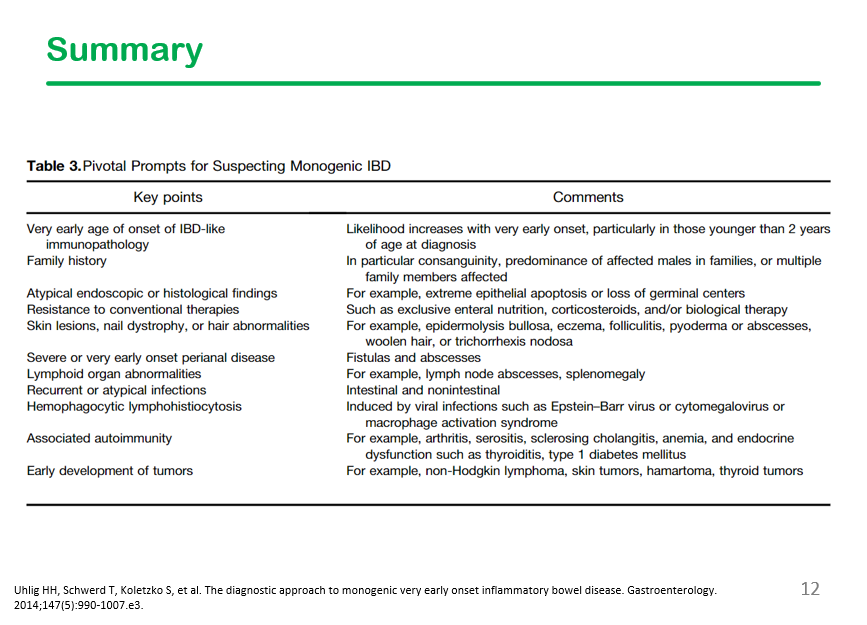
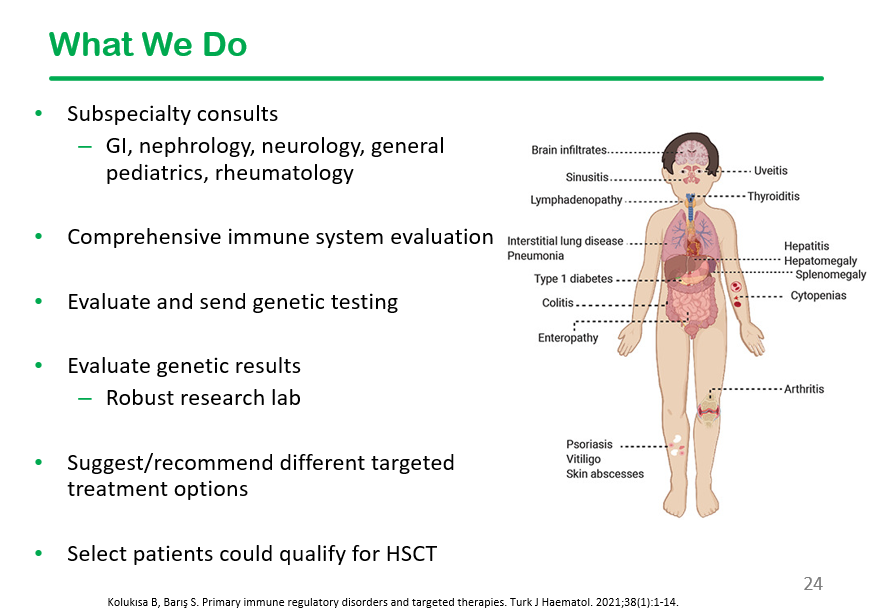
This slide shows the high frequency of extraintestinal manifestations in patients with monogenetic disorders, particularly recurrent infections, skin/hair abnormalities, and autoimmunity. Perianal disease is also frequent in this population.
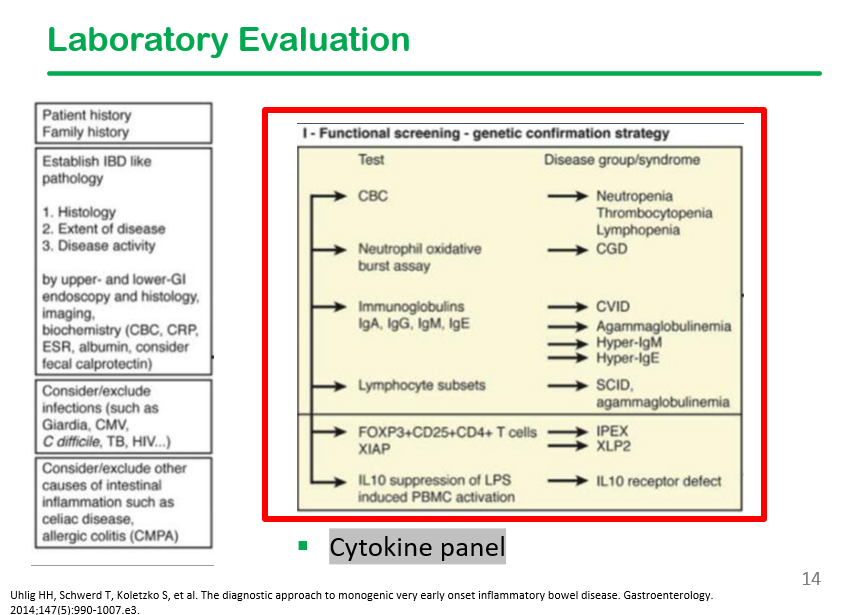
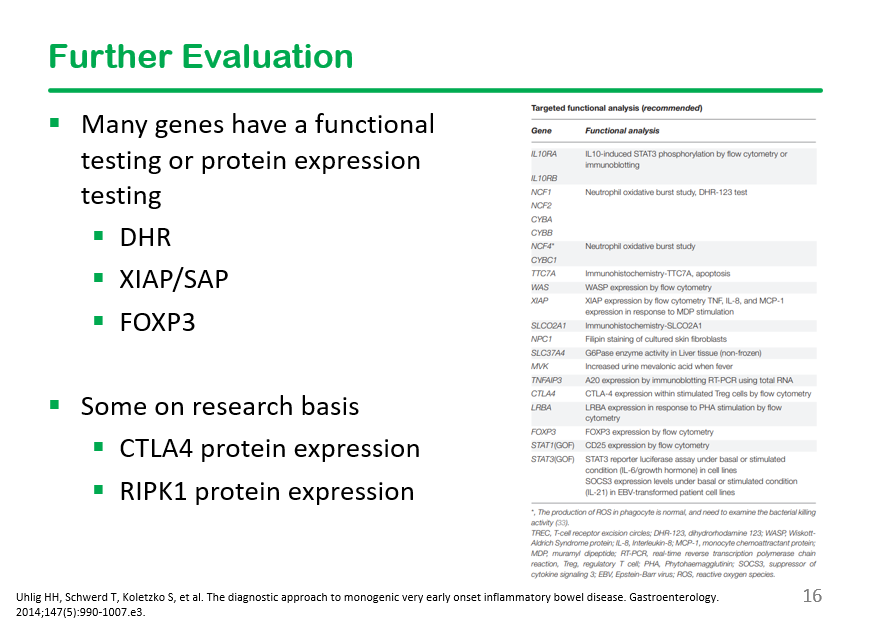
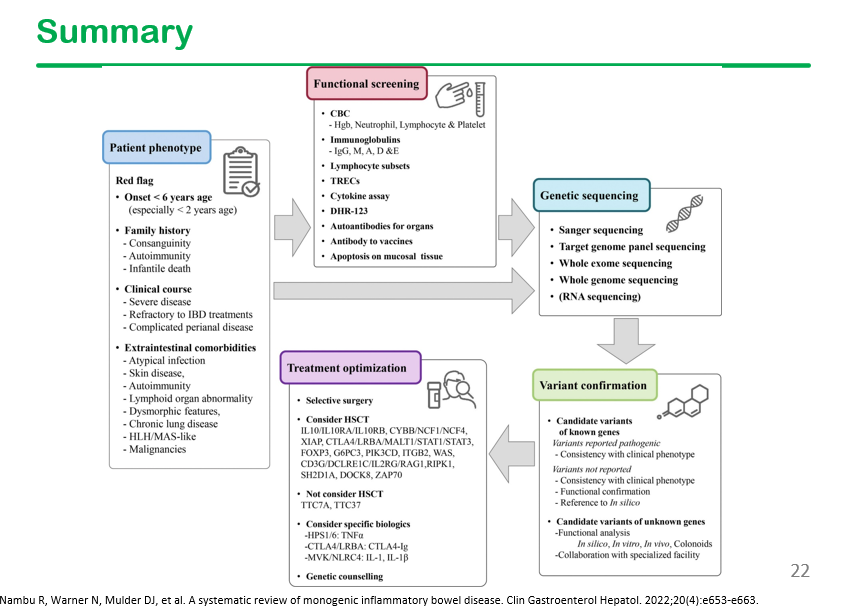
In the discussion, it was noted that DHR testing is often unreliable, especially if the specimen is not run promptly.
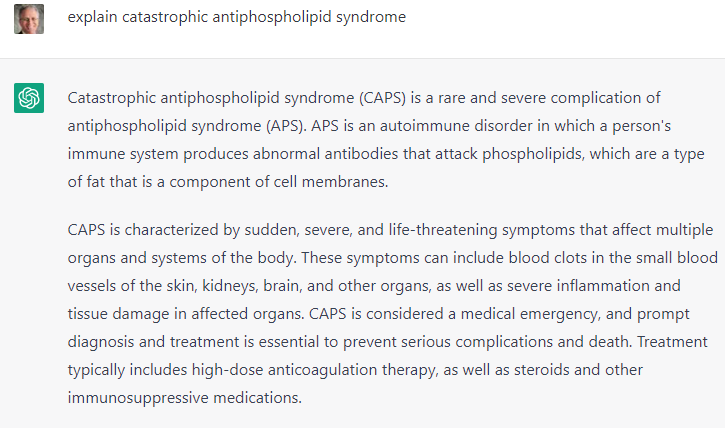
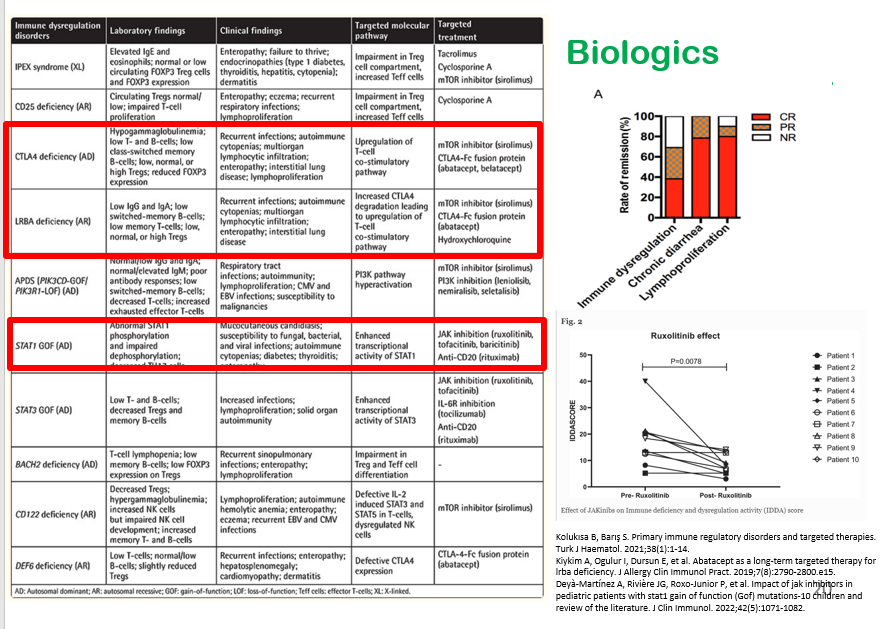
My take: I have had several patients with IBD/immune dysregulation, including a patient with CTLA4 and a patient with TTC7A. Making these diagnoses led to specific treatment recommendations. The patient with CTLA4 is doing well with abatacept therapy.
For those in Atlanta, a referral can be made via EPIC order and/or via contact with immune dysregulation team members. Epic order:

Related blog posts:
- Patterns and Puzzles with Very Early Onset Inflammatory Bowel Disease
- Targeted Therapy for Autoinflammatory Very Early Onset Inflammatory Bowel Disease
- How Very Early Onset-Inflammatory Bowel Disease is Different, Plus One | gutsandgrowth
- VEO-IBD -Useful “Position” Paper is Really a Review
- When To Perform Genetic Testing In The Setting Of Inflammatory Bowel Disease | gutsandgrowth
- Selected Slides from NASPGHAN 2022 Postgraduate Course (Part 2)
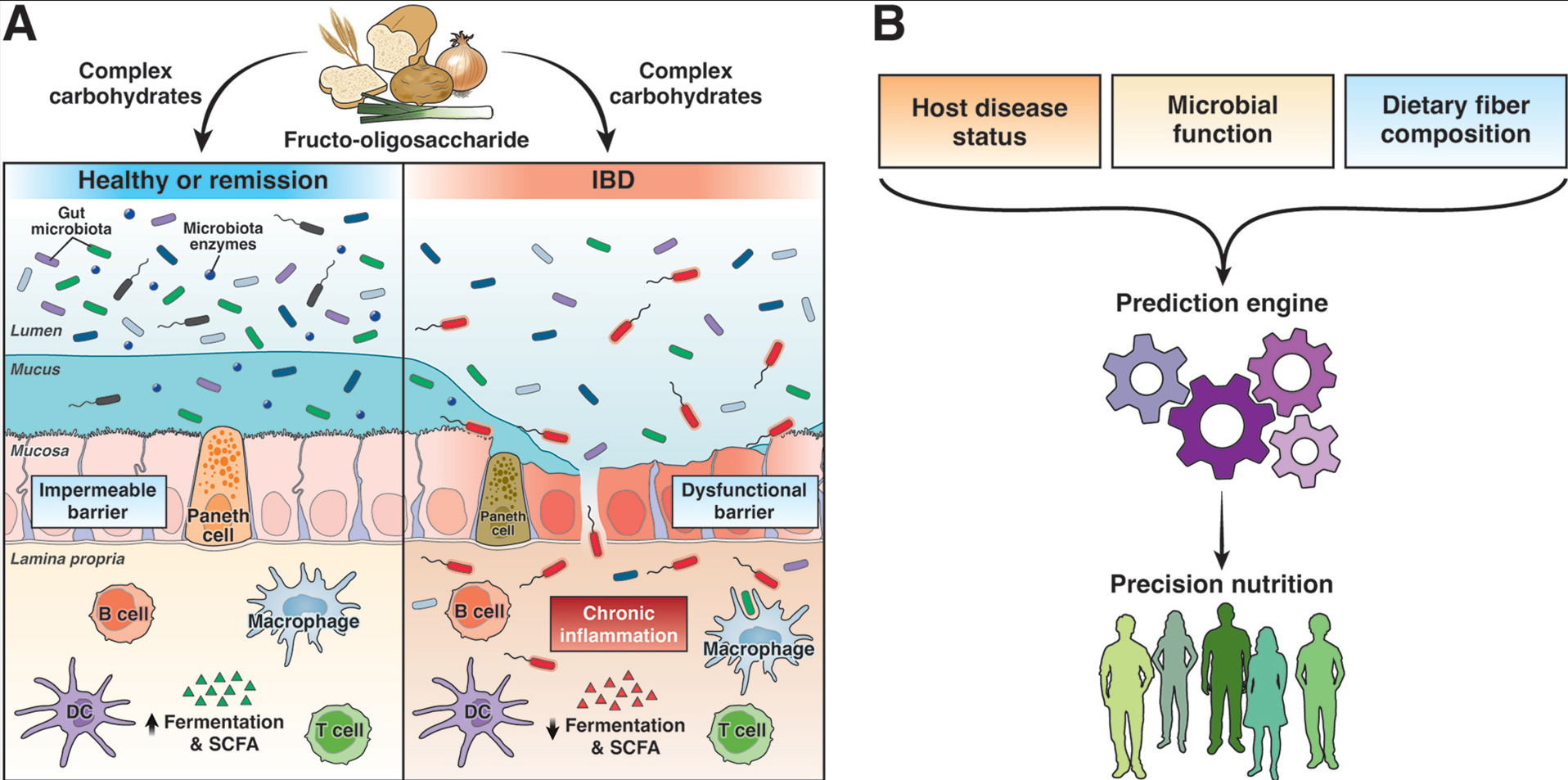
- Getting Lost in the Pathophysiology of Inflammatory Bowel Disease | gutsandgrowth
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.