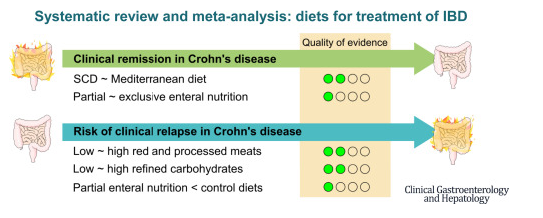
This was a systematic review of prospective controlled trials (n=27) of solid food diets for the induction or maintenance of remission in IBD.
Key findings:
For induction of remission in Crohn’s disease (CD), the Mediterranean diet was similar to the Specific Carbohydrate Diet (low certainty of evidence), and partial enteral nutrition (PEN) was similar to exclusive enteral nutrition (very low certainty of evidence).
PEN reduced risk of relapse (very low certainty of evidence), whereas reduction of red meat or refined carbohydrates did not (low certainty of evidence).
For ulcerative colitis, diets were similar to controls (very low and low certainty of evidence).
My take: Most of the dietary treatments for IBD have low to very low certainty of evidence regarding their effectiveness. Dietary changes are very likely to be helpful but more studies with rigorous endpoints are still needed.
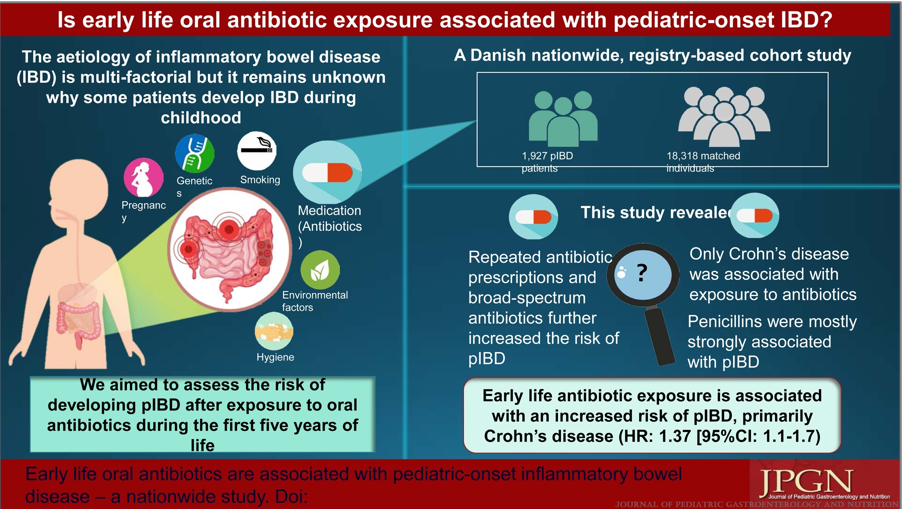
Oral antibiotic exposure during the first 5 years of life was associated with a higher risk of developing pIBD (HR = 1.33, P <0.0001). The risk was also increased if patients had ≥4 antibiotic prescriptions compared to no antibiotics (HR = 1.33, P <0.0001).
Broad-spectrum antibiotics increased the risk of pIBD compared to narrow-spectrum antibiotics (HR = 1.29, P < 0.0001).
When stratified by IBD subtypes, only Crohn disease was significantly associated with exposure to antibiotics (HR = 1.37, P = 0.002).
My take: This study indicates that antibiotics (and/or serious infections) are associated with an increased the risk of pediatric Crohn’s disease but the absolute risk is very low. We still have a lot to learn about how environmental exposures, including diet, infections, antibiotics, and pollution, contribute to the increasing prevalence of inflammatory bowel disease.
Related blog posts:
Early Antibiotics -Minimal Risk for Crohn’s Disease The cumulative risk of CD at the 11th birthday for children exposed to antibiotics in their first year of life was 0.16% compared to 0.11% for children unexposed to antibiotics in their first year of life.
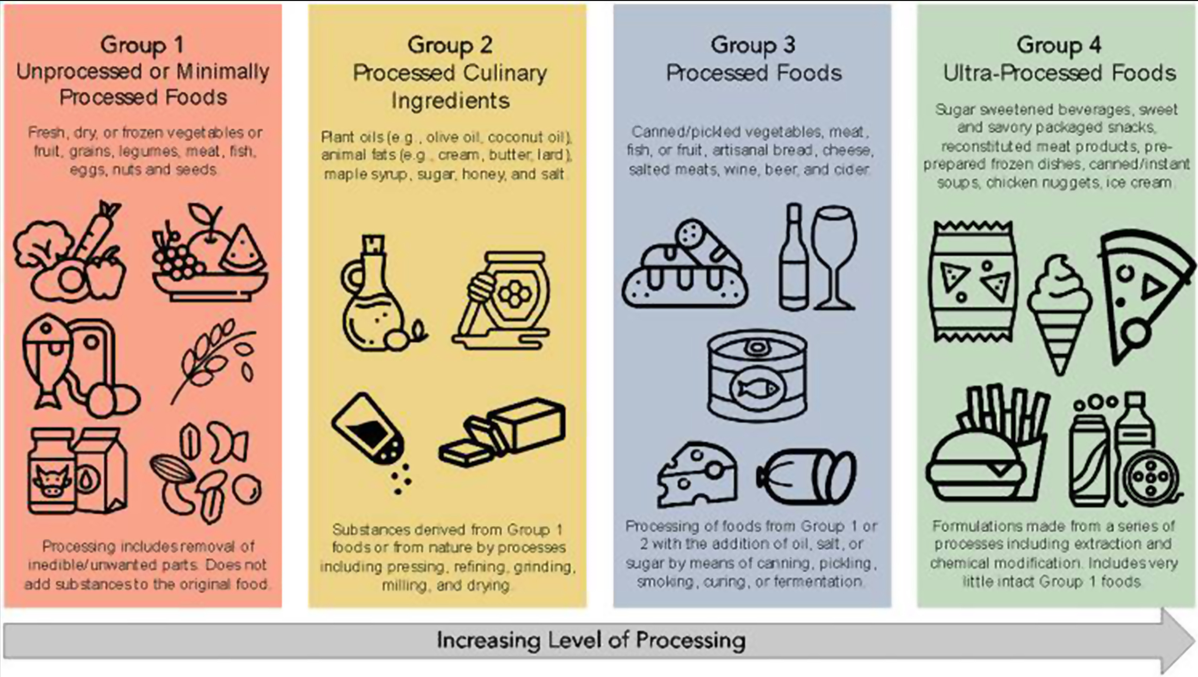
Figure 1 from editorial: The NOVA classification of food
A total of 1,068,425 participants were included (13,594,422 person-years) among 5 cohort studies published between 2020 and 2022. The average age of participants ranged from 43 to 56 years. Key findings:
Crohn’s disease: During follow-up, 916 participants developed CD, and 1934 developed UC. There was an increased risk for development of CD for participants with higher consumption of ultra-processed foods compared with those with lower consumption (HR, 1.71; 95% CI, 1.37–2.14; I2 = 0%) and a lower risk of CD for participants with higher consumption of unprocessed/minimally processed foods compared with those with lower consumption (HR, 0.71; 95% CI, 0.53–0.94; I2 = 11%).
Ulcerative colitis: There was no significant association between risk of UC and ultra-processed foods (HR, 1.17; 95% CI, 0.86–1.61; I2 = 74%) or unprocessed/minimally processed foods (HR, 0.84; 95% CI, 0.68–1.02; I2 = 0%).
The associated editorial by Fitzpatrick et al, notes that “there are plausible mechanisms that explain the associations of higher UPFs and development of CD, such as: (1) displacing the intake of minimally processed foods and subsequently reducing exposure to beneficial micronutrients, antioxidants, and phytochemicals; (2) driving overconsumption of total calories7; and (3) increasing exposure to non-nutritive food substances that have been implicated in the development of CD in pre-clinical studies…The notion is that a lower UPF intake is better, but a cutoff value remains elusive.”8
My take (borrowed from editorial): “the population studies have indicated that the extremes of UPF intake are related to risk of CD and that such associations are underpinned by plausible biological mechanisms, suggesting causality.”
In 2012, this blog highlighted a study which showed that “only 31.1% of 206 patients with IBD would have been eligible to participate in any of the selected RCTs.” (Post: According to the study which you would never qualify for…).
This study utilized data for children initiating biologics from two prospective real‐world cohorts and one retrospective cohort.
Key findings:
Only 62 of 164 (38%) children with moderate–to‐severe disease would have been eligible for inclusion in the original RCTs.
The steroid-free remission rate was higher in the eligible children (51%) than in the ineligible children (31%; OR 2.3 [95%CI 1.2–4.5]; p = 0.01)
The main exclusion criterion was prohibited previous therapies (47%)
My take (borrowed from authors): “Remission rates were higher among eligible children raising the concern that results presented in regulatory RCTs in paediatric IBD do not necessarily reflect the patient‐mix in the real‐world and should be interpreted with caution when applied to clinical practice.”
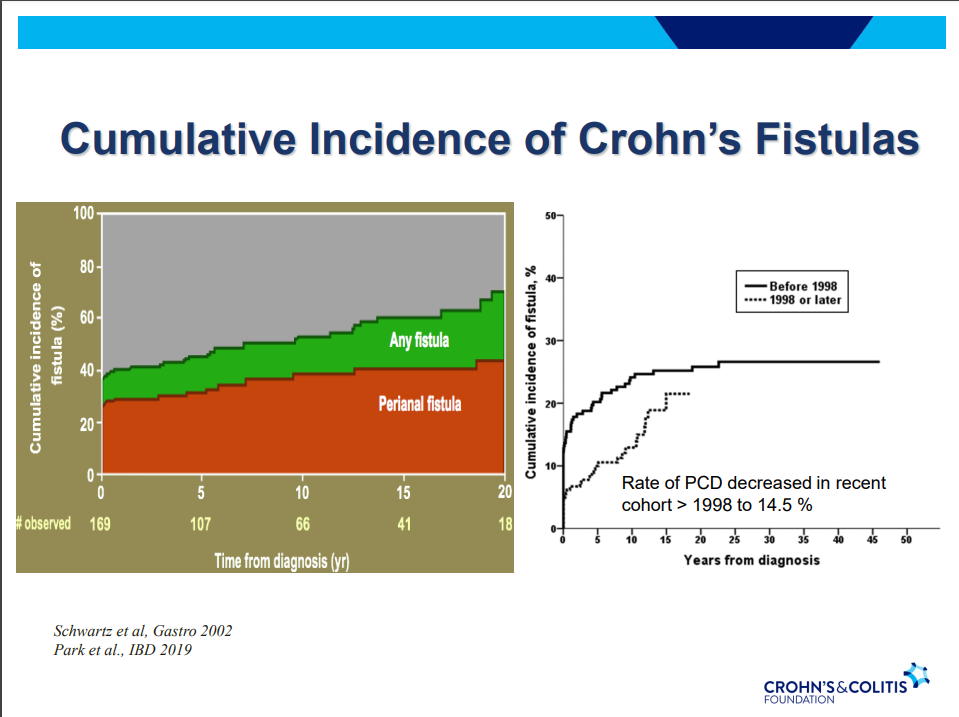
Another very good review by David Schwartz on The Daunting Duo: Management of Stictures and Fistula. Below are some of my notes and some slides; my notes may contain errors in transcription or omission. Can get access to all 49 slides here: IBD Pro CCFA 2023 Atlanta
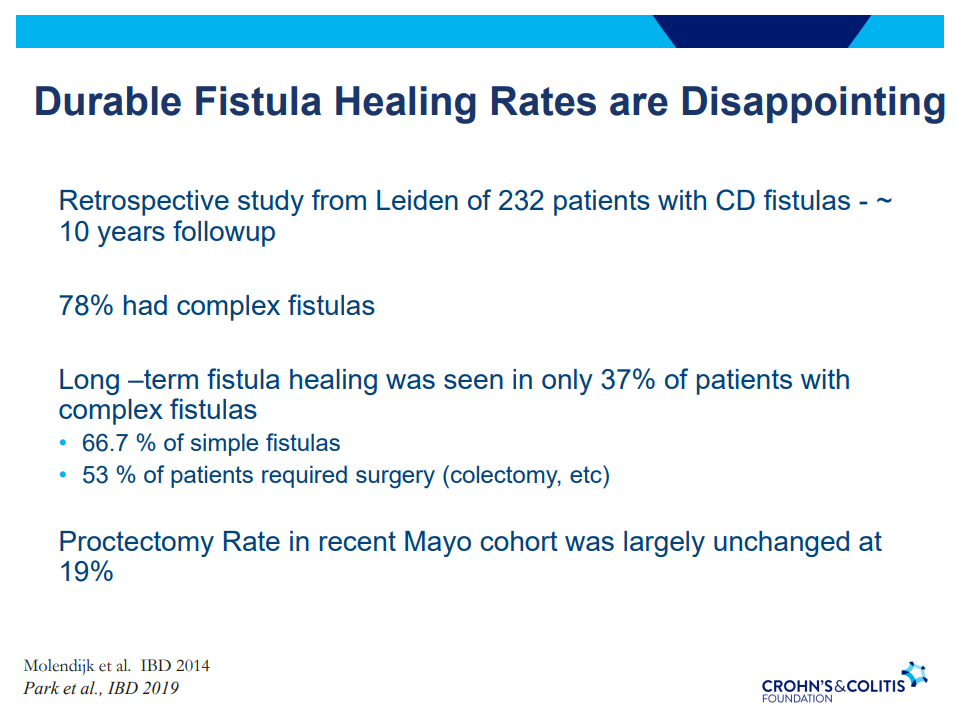
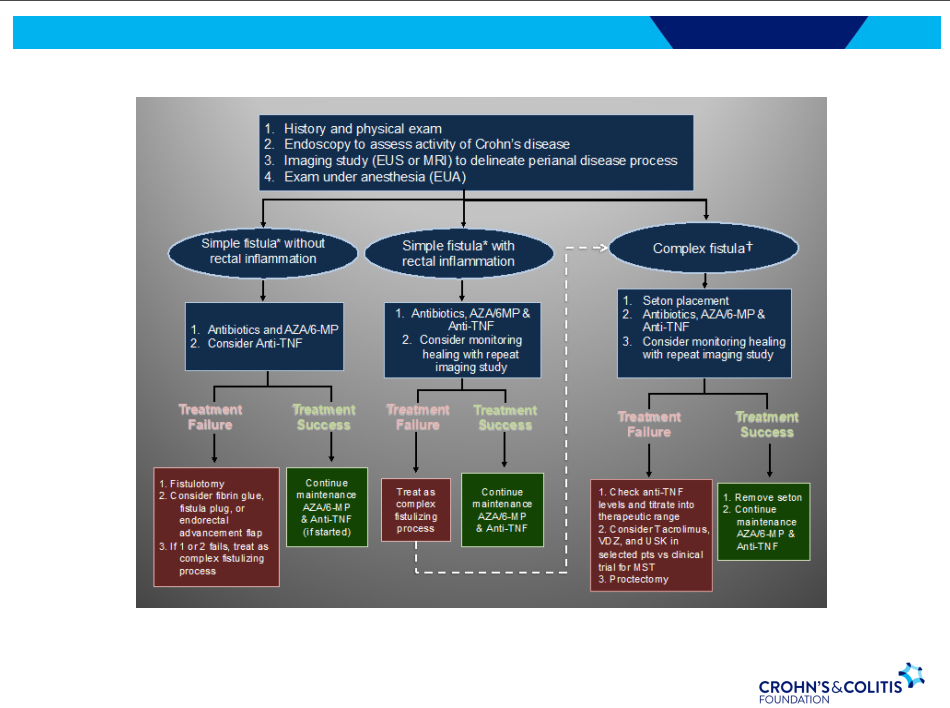
Fistula healing rates are poor
78% have complex fistulas
Long-term healing: 67% with simple fistulas but only 37% with complex fistulas
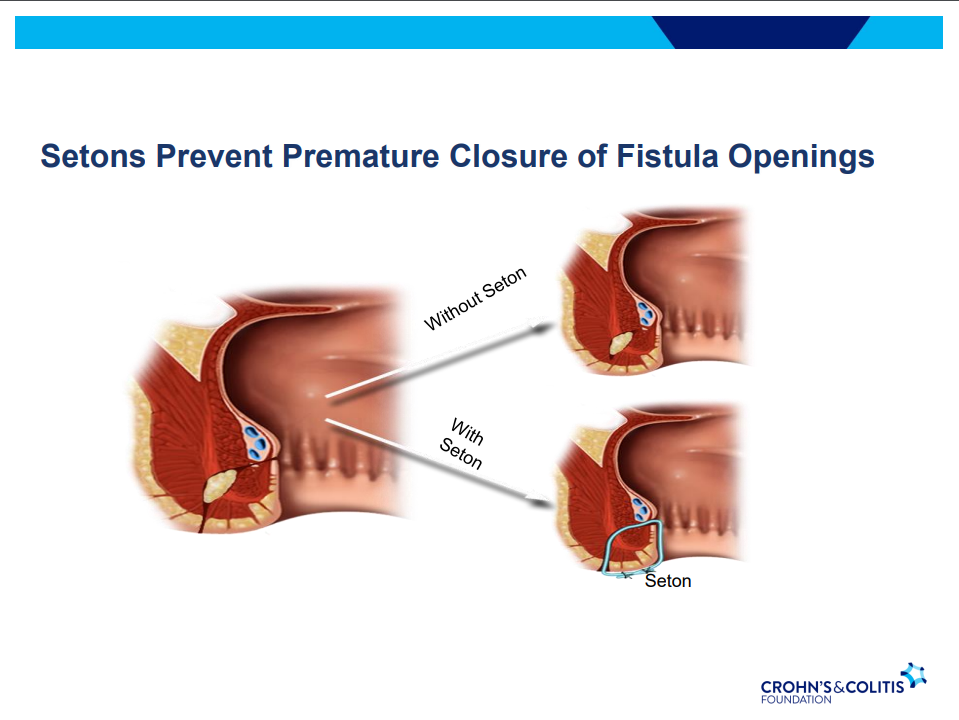
Seton placement prior to biologic therapy increases likelihood of better outcomes
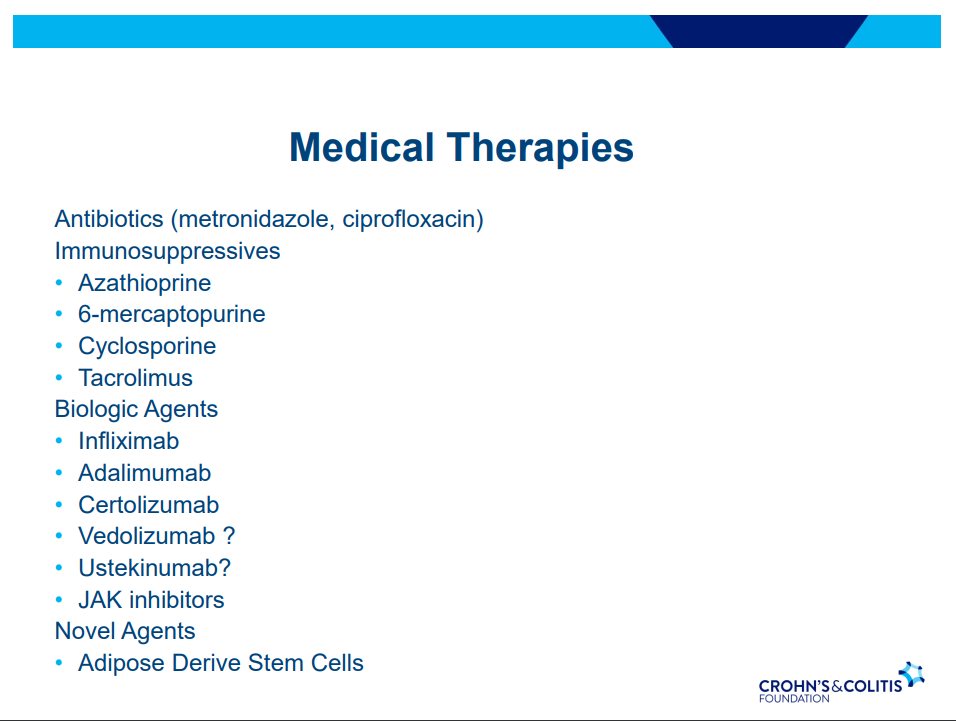
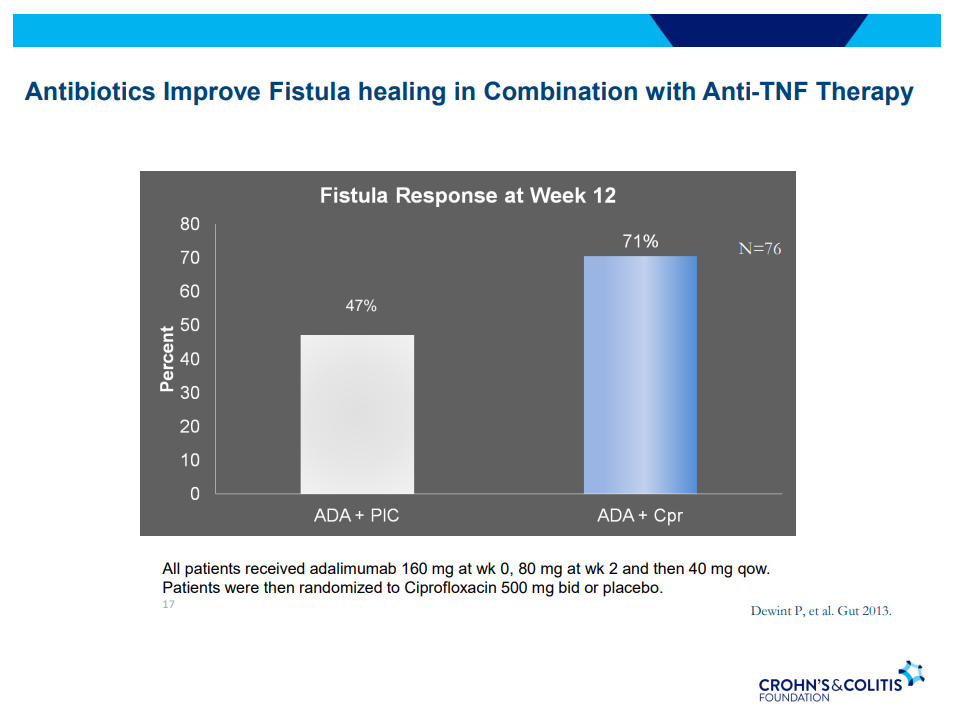
Antibiotic therapy recommended until Seton removed (not short-term treatment) –improved healing rates along with medical therapy
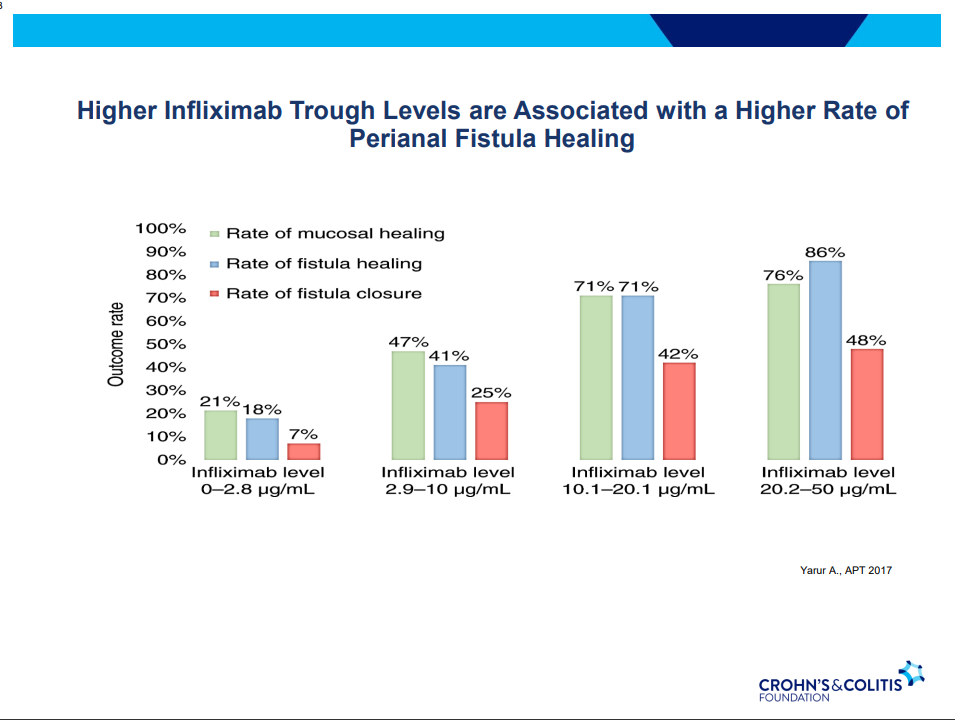
Anti-TNF therapy effective in ~40% long-term; higher rates of healing with higher anti-TNF levels
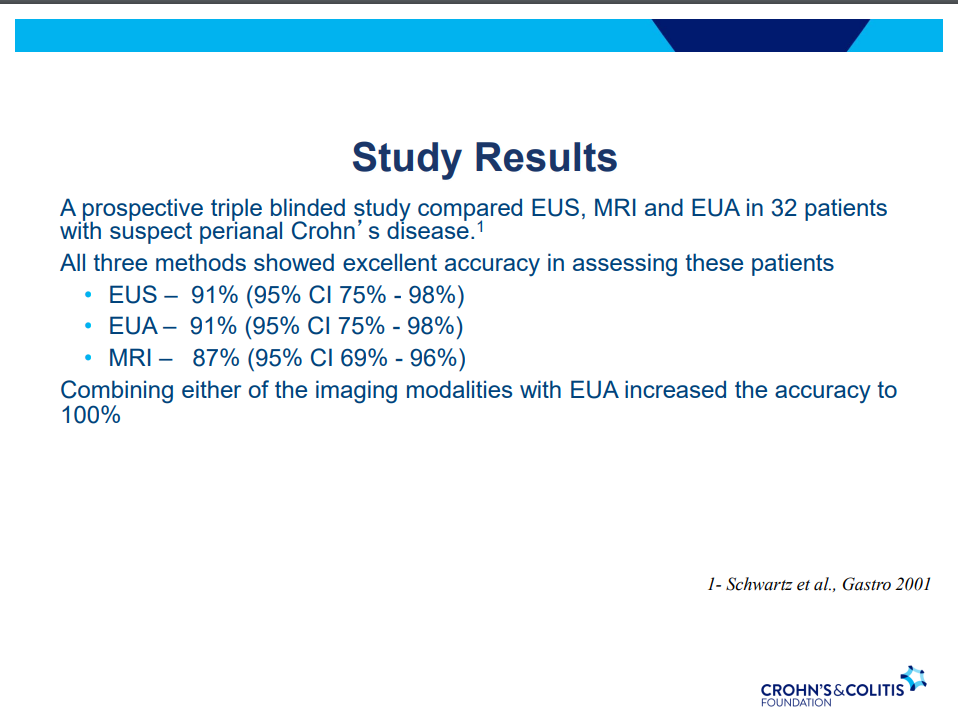
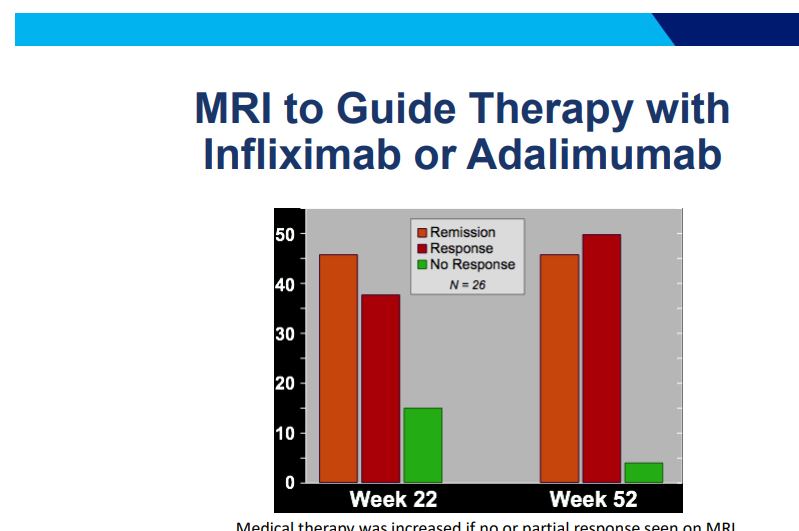
MRI and/or EUS helpful in improving fistula healing rates
Ustekinumab and Vedolizumab both had fistula healing rates ~40%
Adipose derived stem cells with ~50% healing rates (study with high placebo healing rate too ~37%); changes local cytokine profile, cells gone in about 2 weeks but goal for changing trajectory
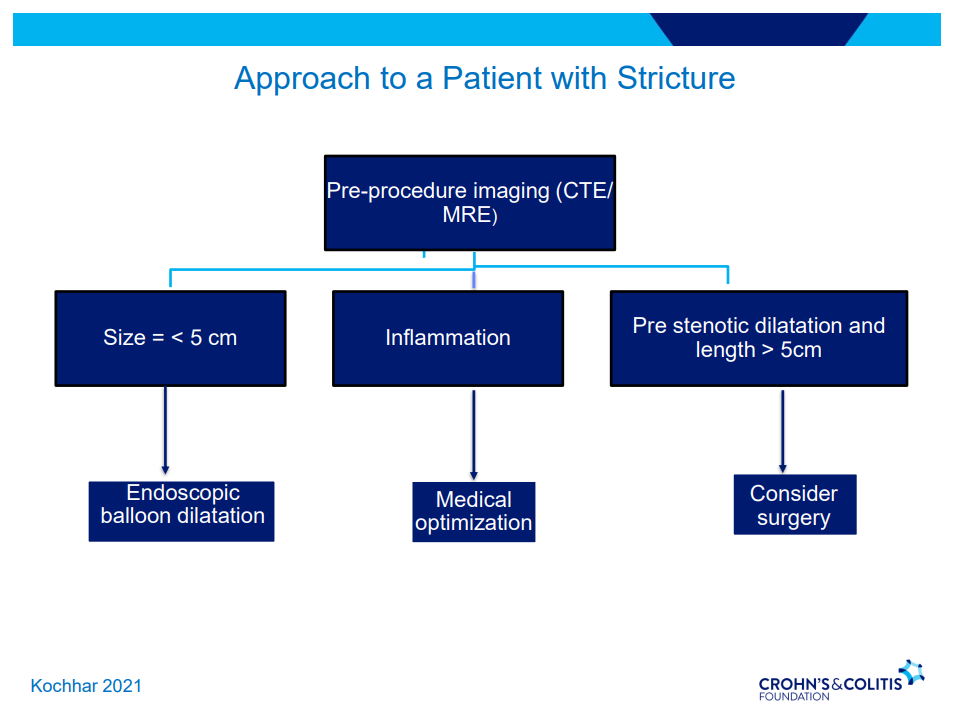
Strictures
5-24% with stricturing phenotype
No effective medical treatments
Endoscopic balloon dilatation in shorter strictures (<5 cm) without associated abscess or fistula (needs imaging prior)
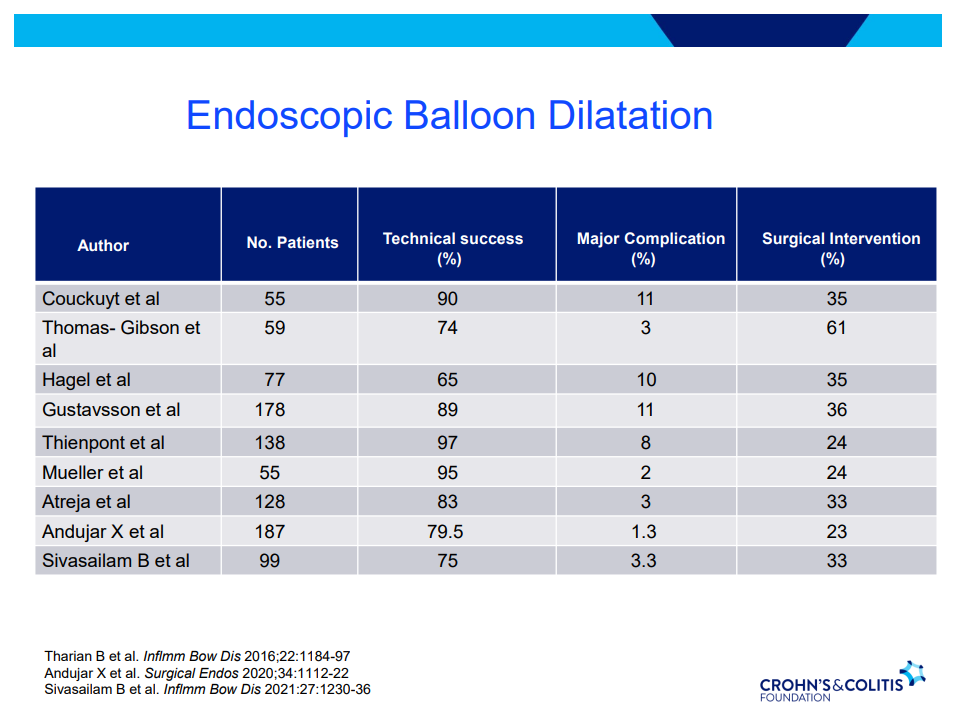
One-third of balloon dilated strictures will still wind up needing surgery despite dilatation. 5-10% risk of complication. Goal is 15 mm or more (Dr. Schwartz typically does not increase by more than 3 sizes from baseline in one session)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This is third day summarizing some of the talks at the regional CCFA conference. Erin Forster presented on Treatment with Oral Advanced Therapy. Below are my notes and some of the slides; my notes may have errors of omission or transcription. Can get access to full slide set: (n=22) here: Treatment with Oral Advanced Therapy
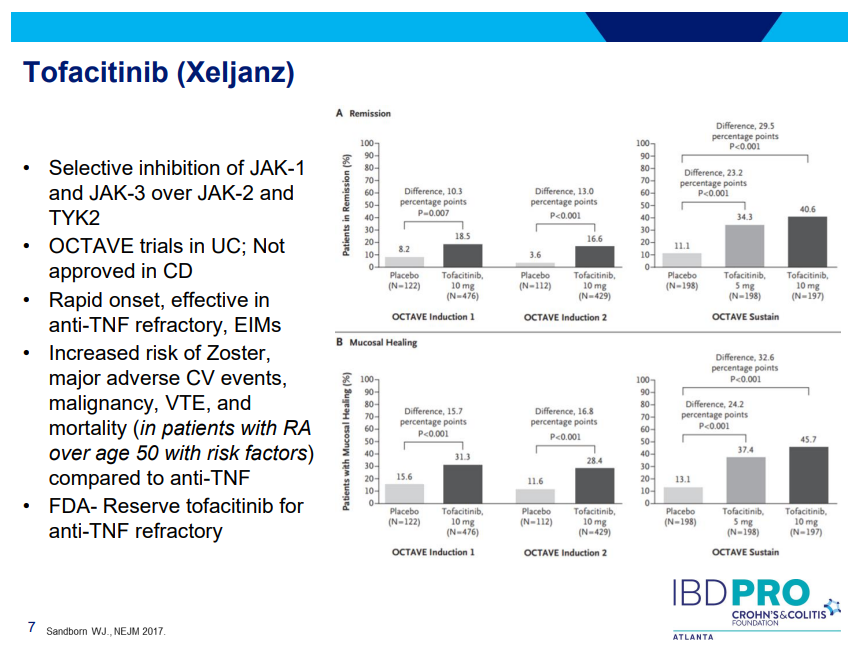
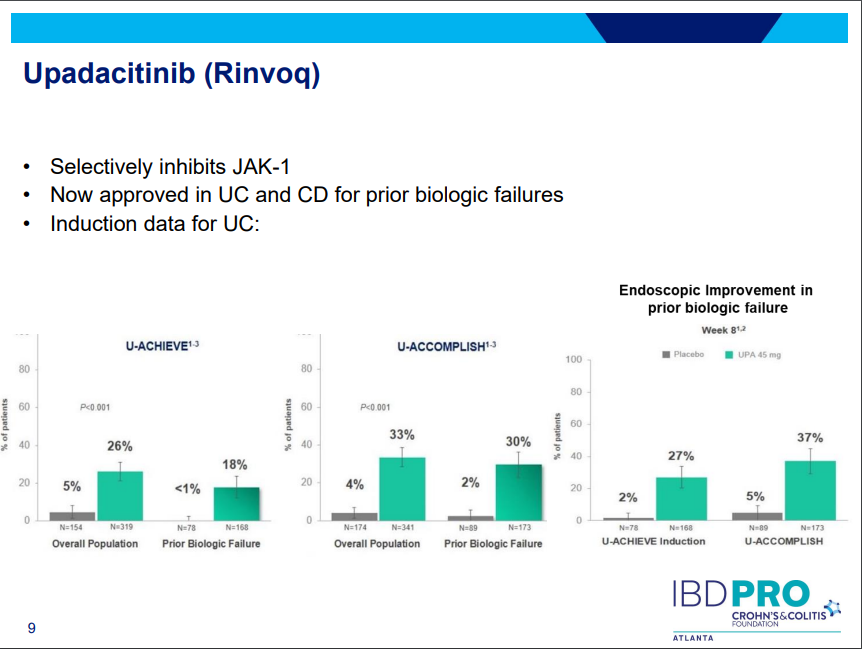
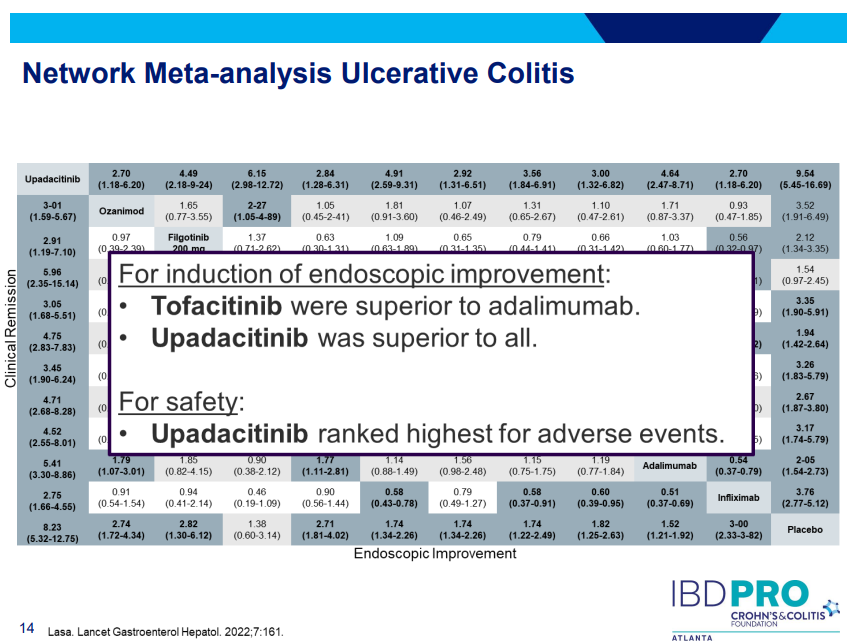
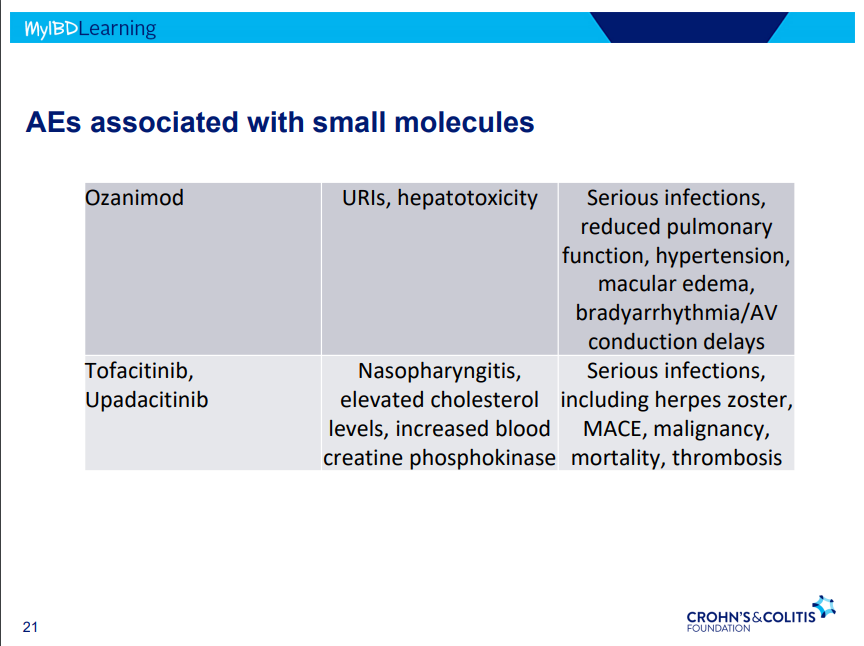
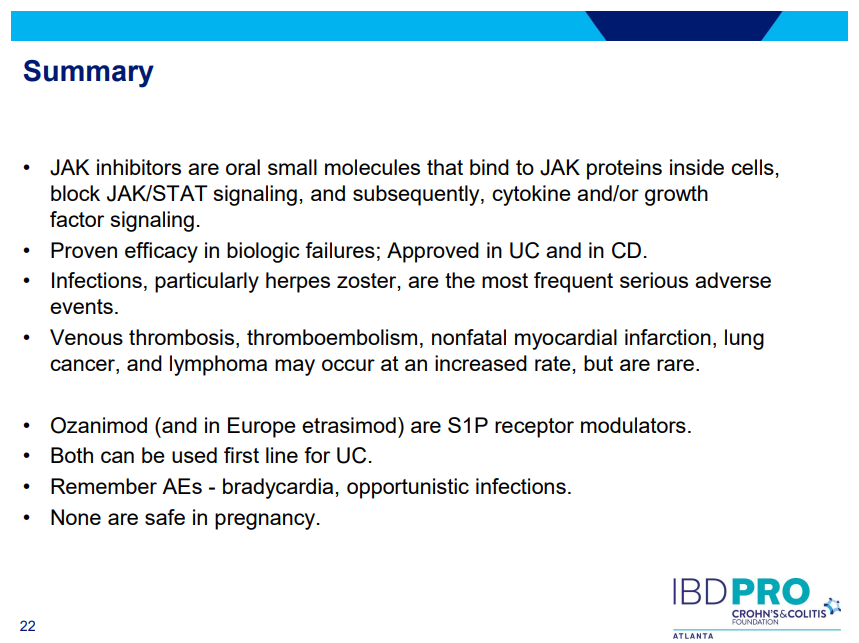
JAK inhibitors (Tofacitinib, Upadacitinib) have rapid onset of action and are taken orally
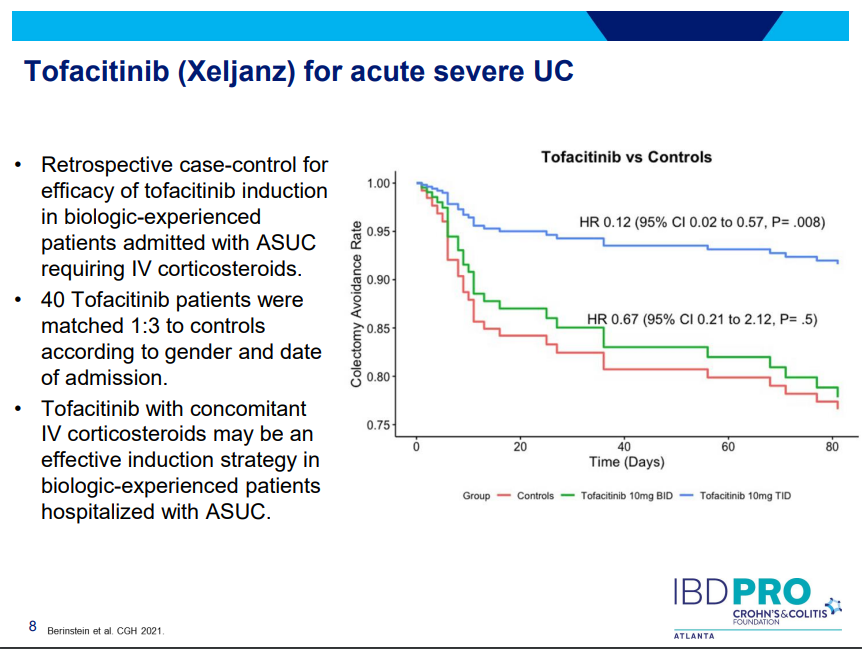
Tofacitinib (Xeljanz) -concern about cardiovascular events was derived from elderly rheumatologic patients. Cardiovascular events are rare. Higher dose (TID) (in the hospital) associated with lower colectomy rates in acute severe ulcerative colitis.
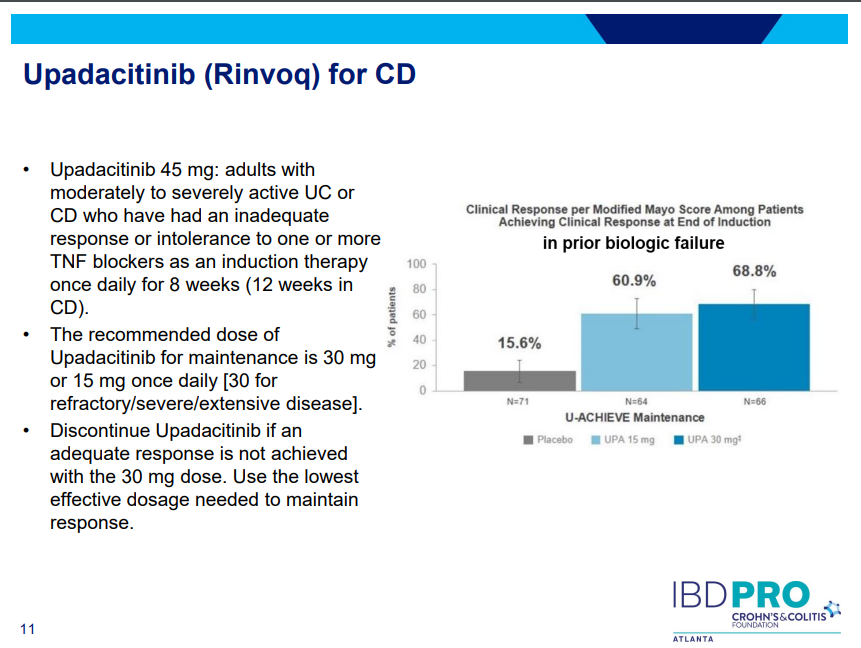
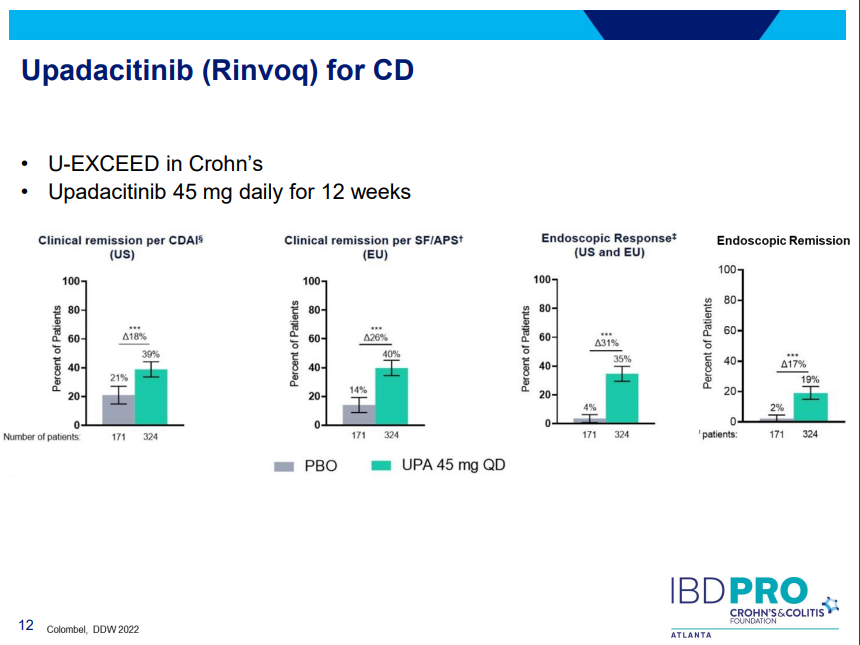
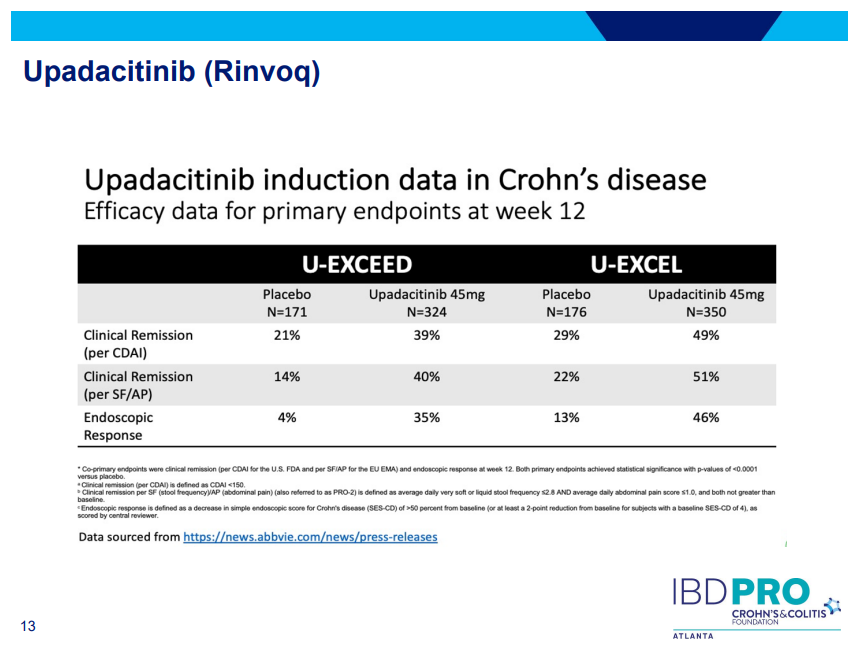
Upadacitinib (Rinvoq) -now approved for CD and UC. Higher dosing could affect liver function (especially if underlying liver disease). Also, JAK inhibitors as a class have similar safety concerns: increased herpes zoster and concerns for cardiovascular concerns (esp if >50 years)..
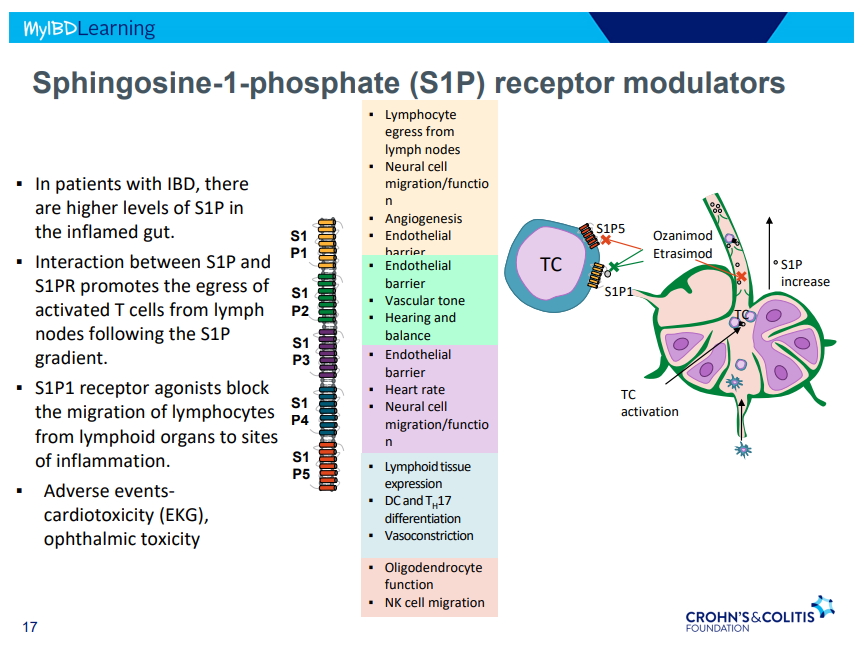
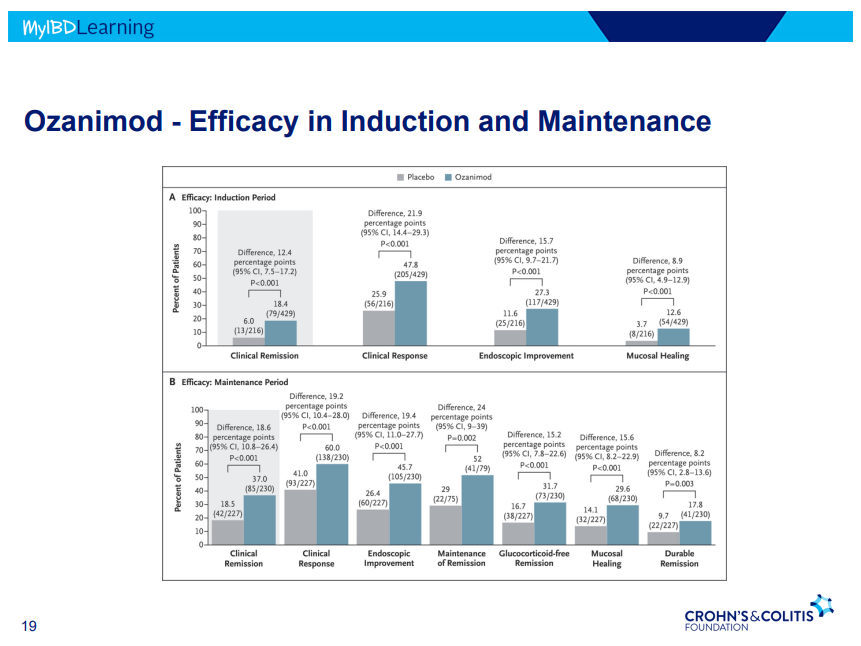
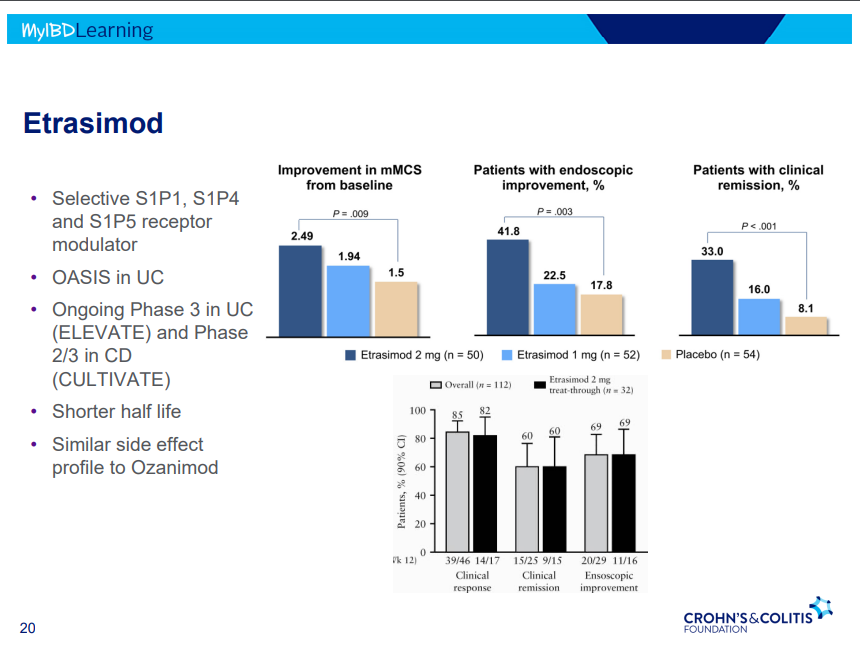
S!P receptor modulators: Oznaimod, Etrasimod & Amiselimod. Can cause bradycardia -have to check EKG prior.
There were a bunch useful lectures at CCFA 2023 regional conference in Atlanta. Here are some of my notes and slides from Doug Wolf‘s lecture; my notes may have errors of omission or transcription. Can get access to full slide set (n=37) here: Dose Escalation of Biologic Therapy and Dual Biologic Therapy
If loss of response to anti-TNF, consider dose escalation by either re-induction or increasing (doubling) dose. Re-induction is less costly
Dose escalation generally not effective for vedolizumab
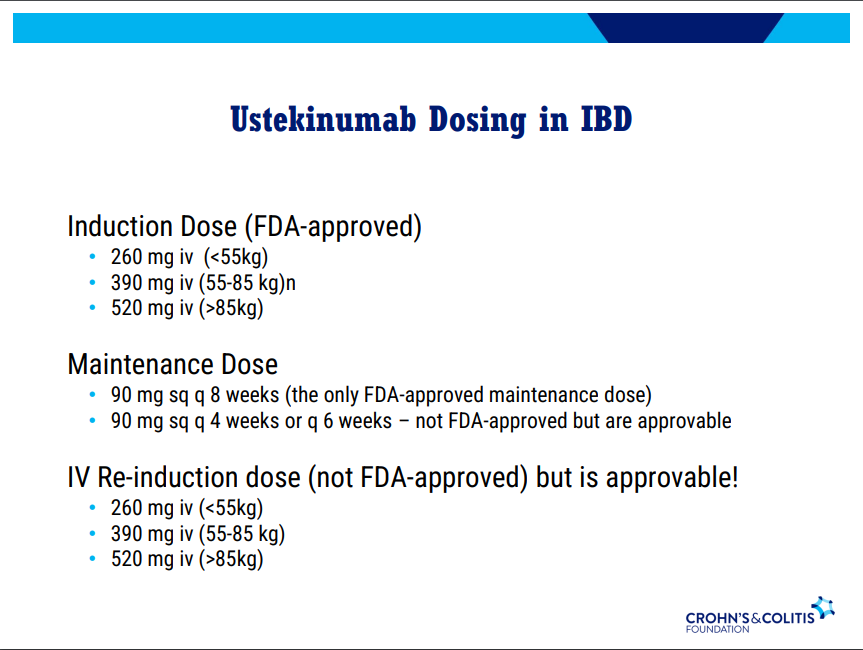
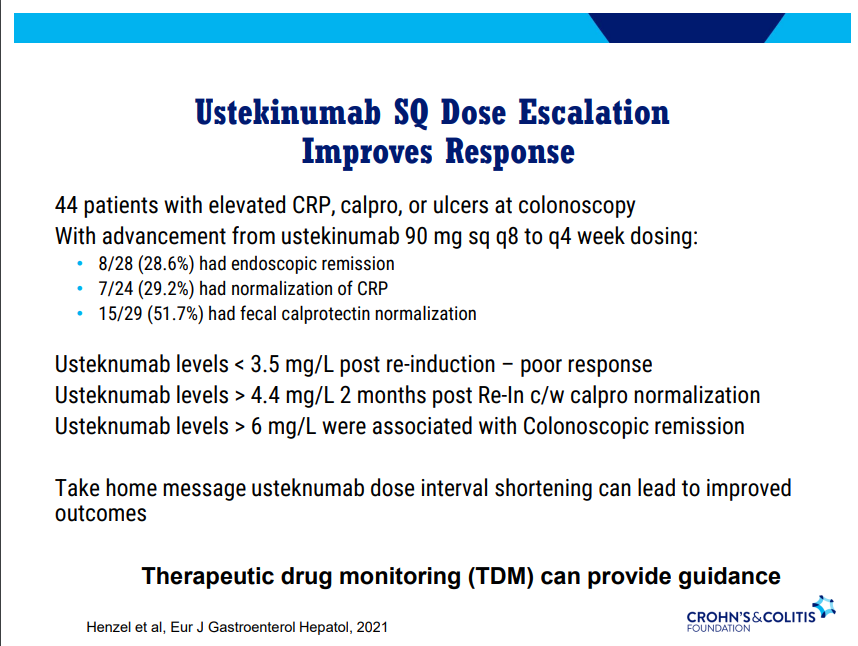
Dose escalation (increased frequency) with ustekinumab can be effective. Therapeutic drug monitoring can provide guidance. Re-induction can also be effective in half of patients (especially in patients with either no prior biologics or one prior biologic)
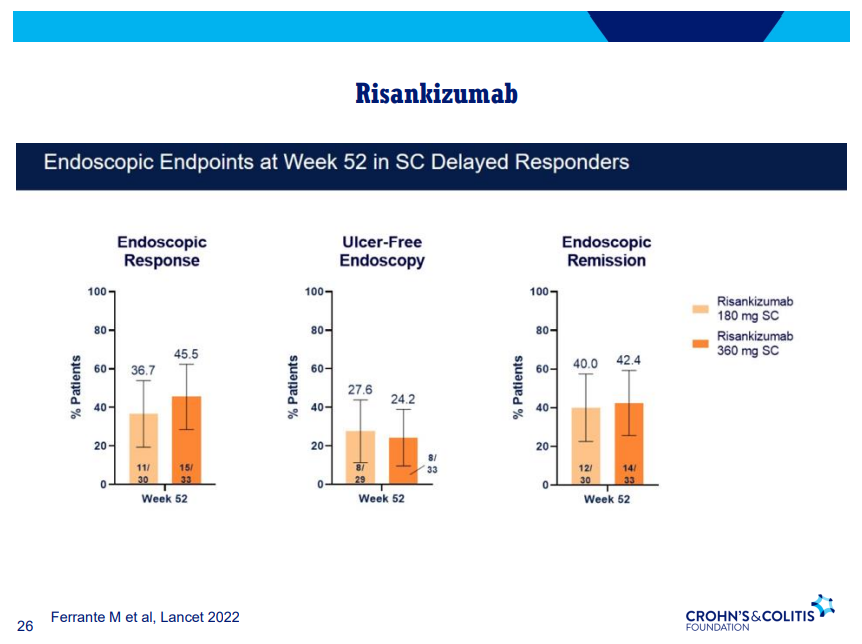
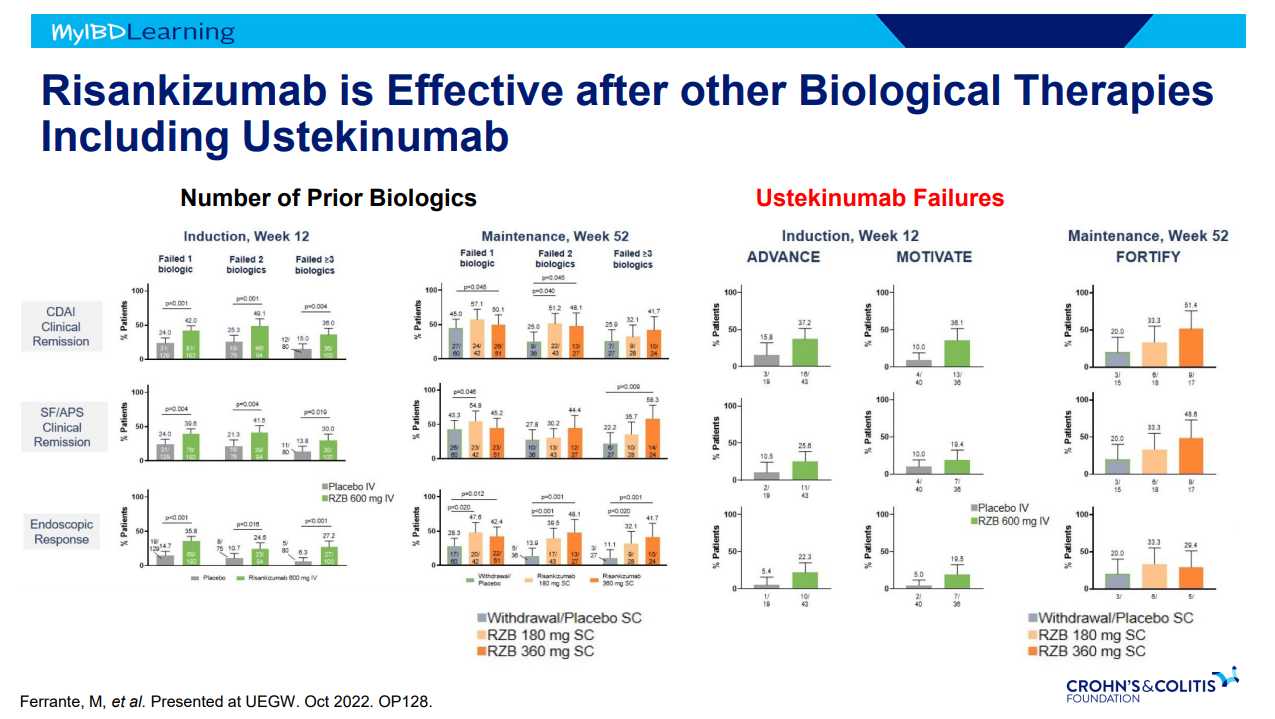
Risankizumab can still work in patients who had not responded by 12 weeks (delayed responders)
Discussed several combination treatments -no large studies thus far
I recently attended a regional CCFA conference. David Rubin gave several terrific lectures. Here are some of my notes and some slides from this lecture. My notes may contain transcription errors as well as important omissions. Can get access to full set of slides here: Biologics and Their Biosimilars
“Biologics and Their Biosimilars“
What is a Biologic Therapy?
Dr. Rubin makes a point of explaining the term to patients. It is a protein made in a living cell that targets another protein. Term “biologic” can sound scary to patients. Usually given IV because they cannot be absorbed through the small bowel.
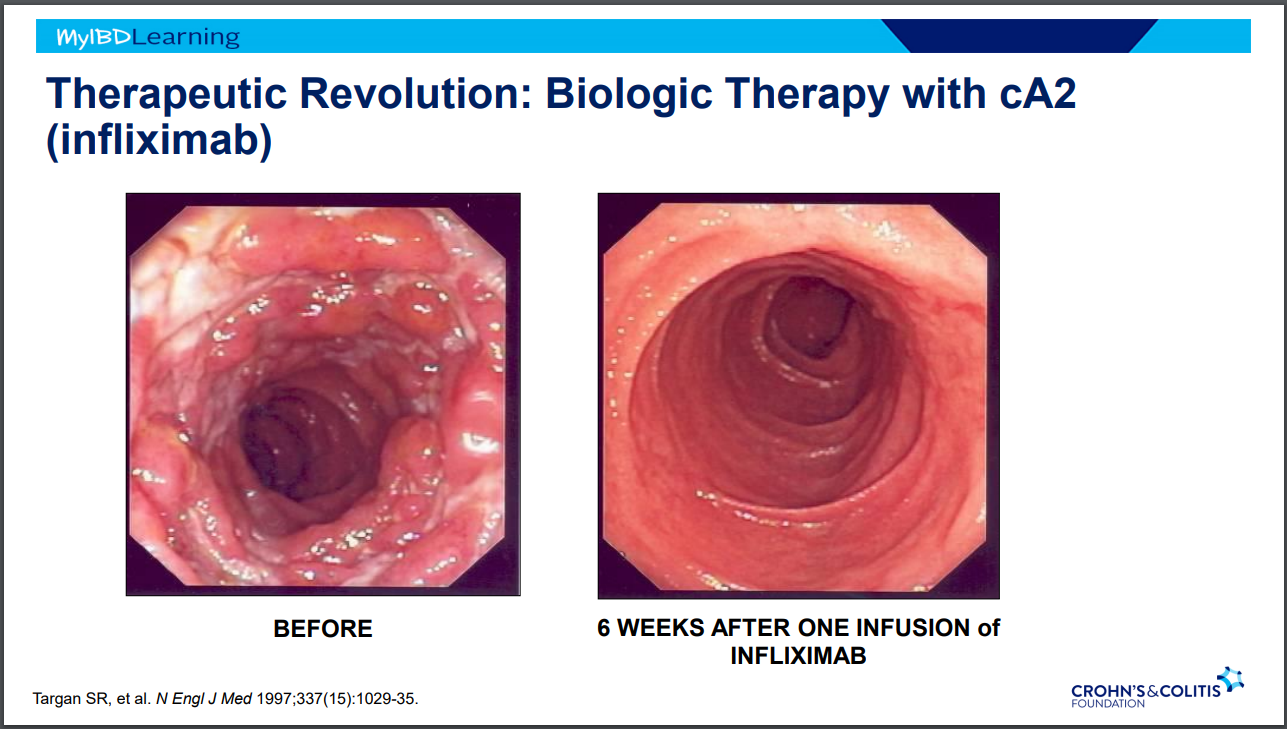
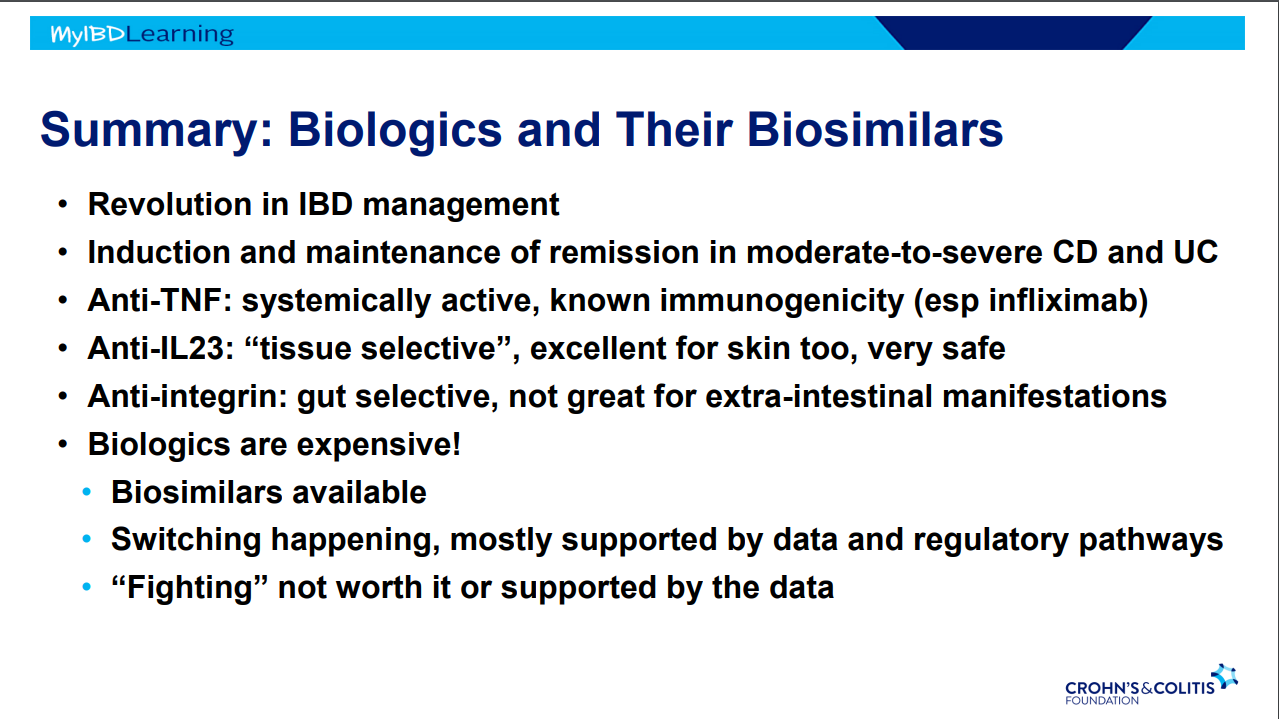
IBD Treatment Revolutions
Steroids -overnight changed mortality in IBD
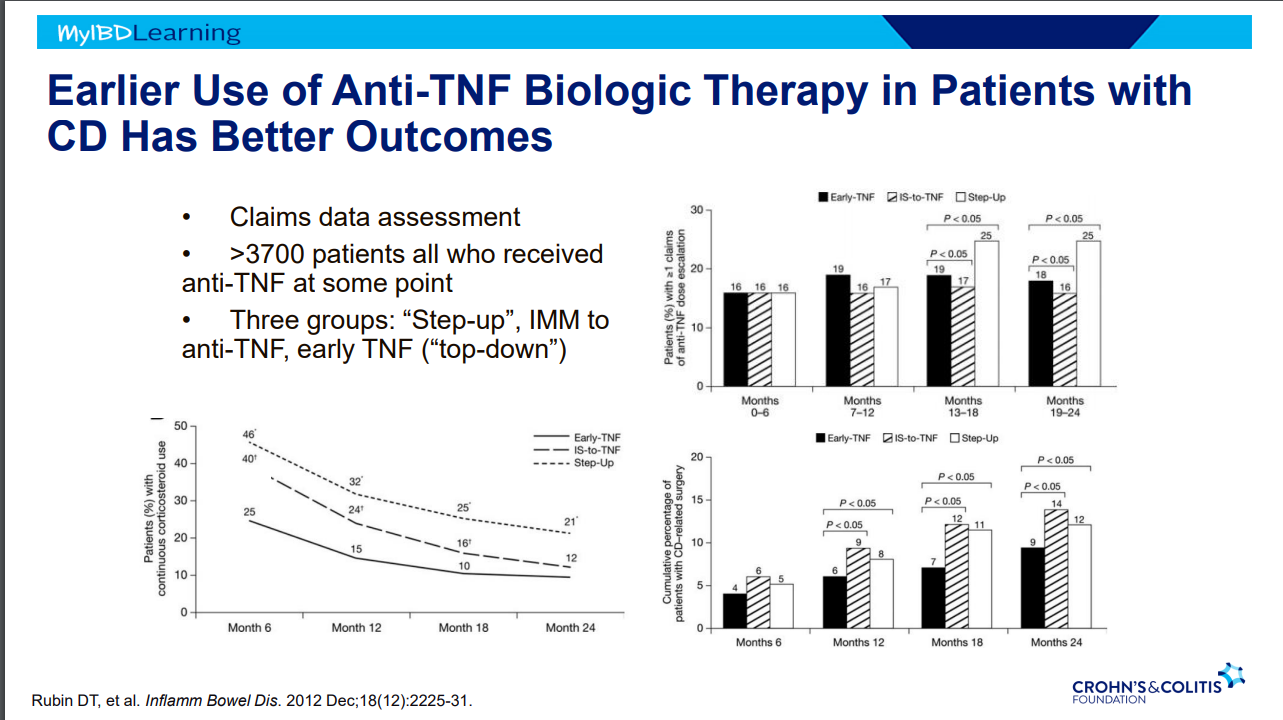
Anti-TNF Therapy in IBD -taught many lessons. Treat earlier –>better outcomes.
Anti-TNF Therapy
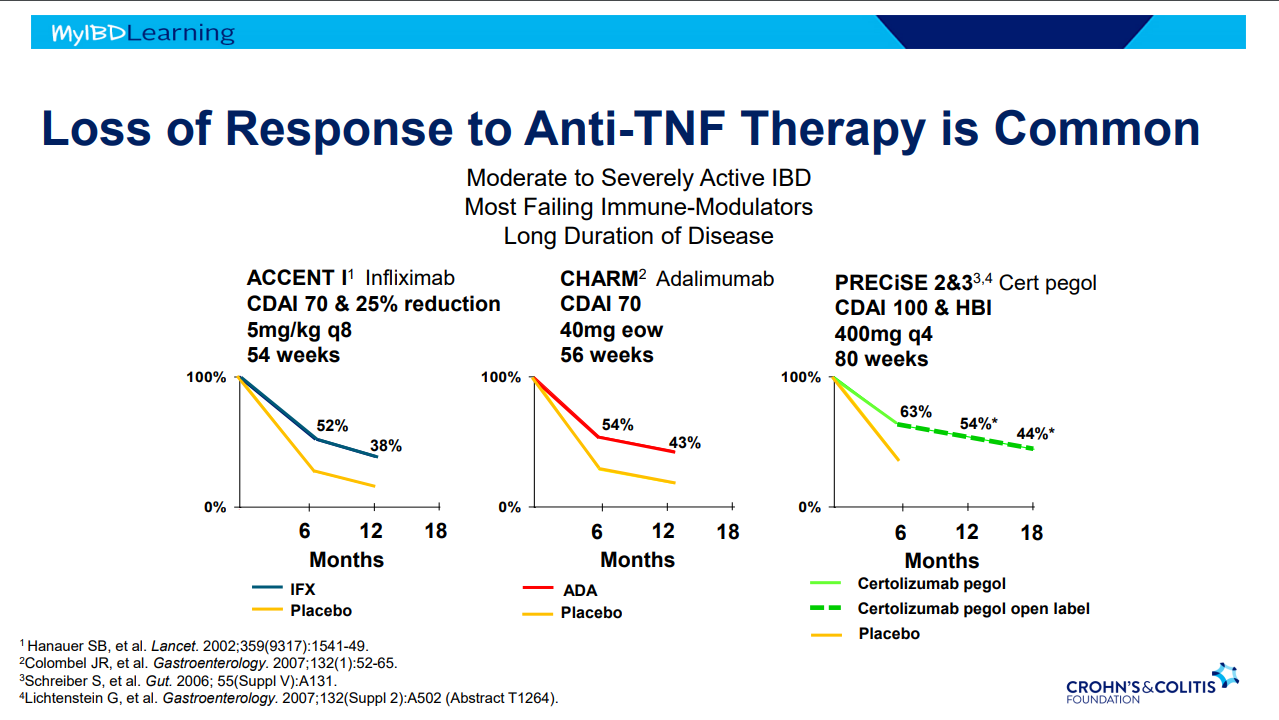
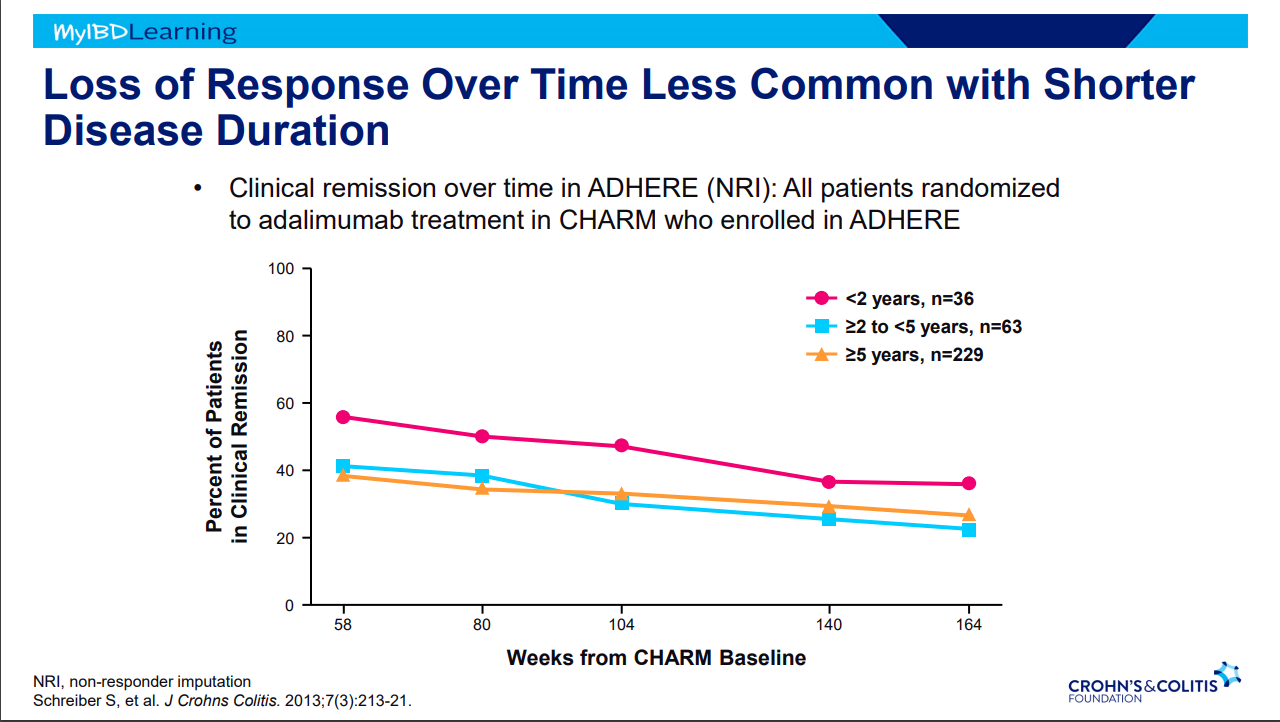
Frequent loss of response.
Earlier treatment with biologics result in better outcomes.
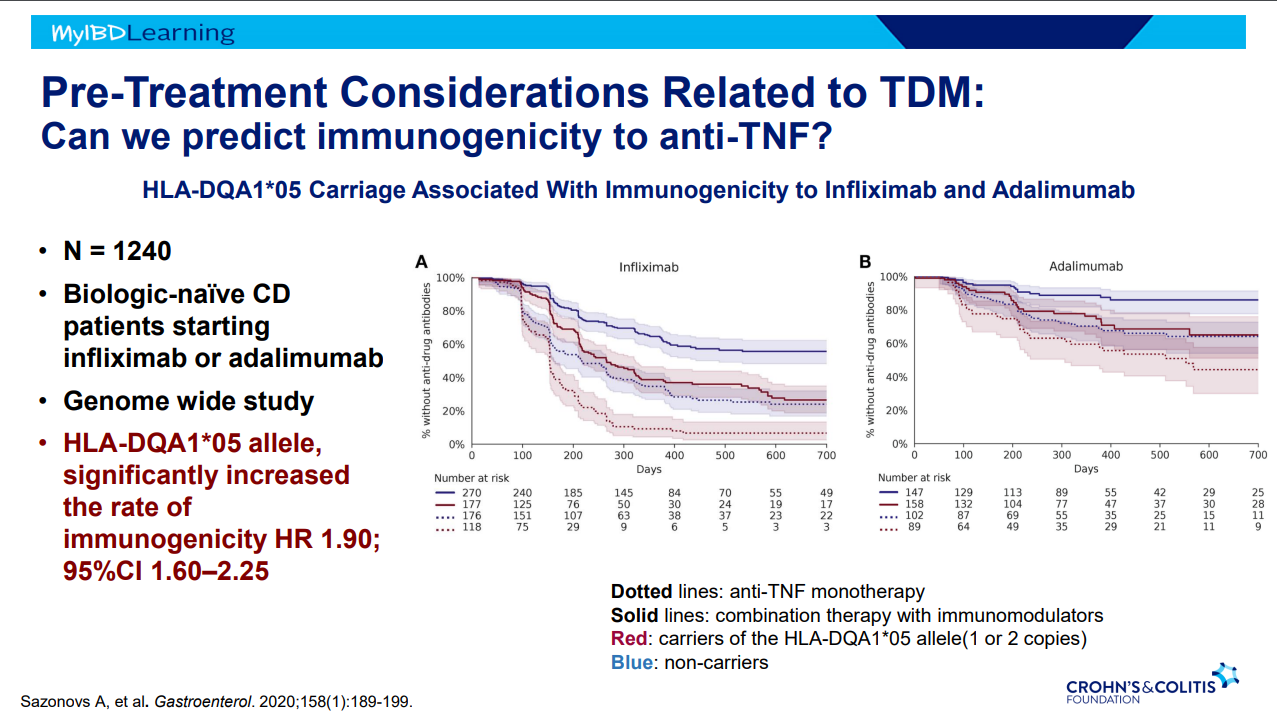
Immunogenicity is mainly an issue with anti-TNF agents and not much of an issue with other biologics. Episodic therapy is a big risk factor for anti-drug antibodies.
If staying with in-class medication, after anti-drug antibodies, need to take additional measures to prevent anti-drug antibodies (eg. Immunomodulators).
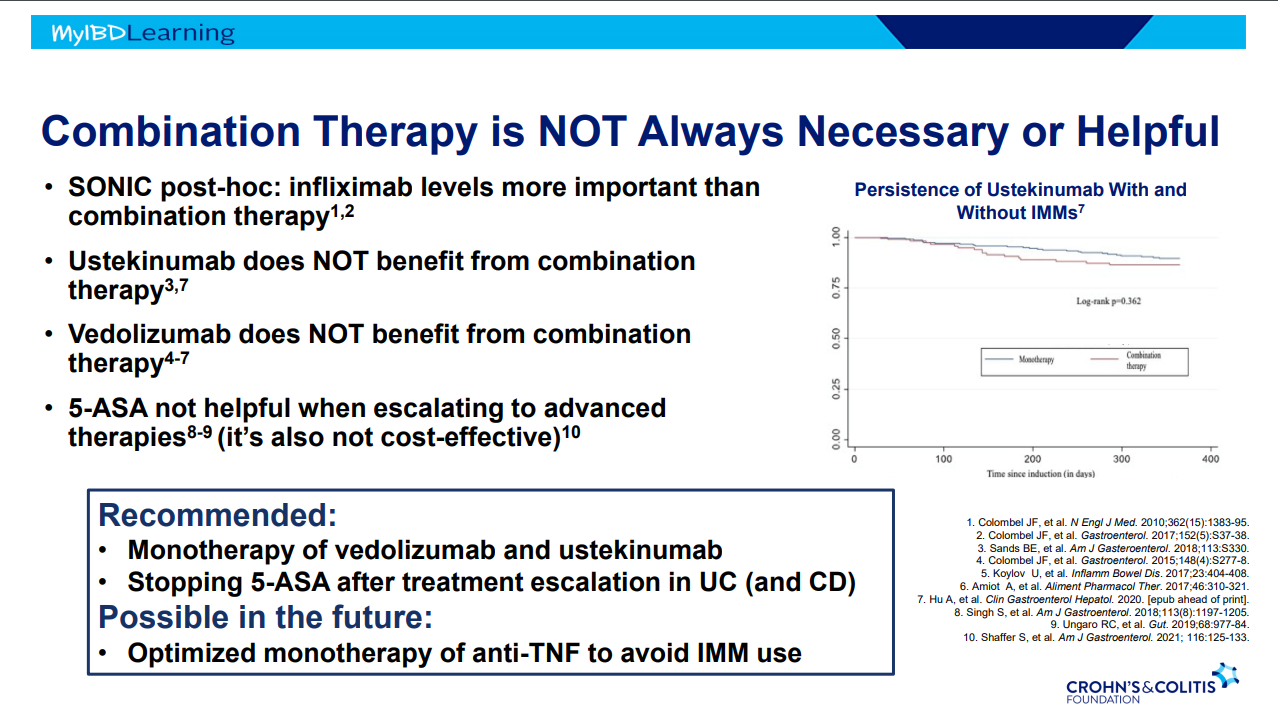
Combination therapy is more effective (SONIC, UC SUCCESS trials). This is due to using multiple mechanisms of disease control, reduction in anti-drug antibodies, and elevated serum drug levels.
Good therapeutic levels appears to deliver similar results as combination therapy
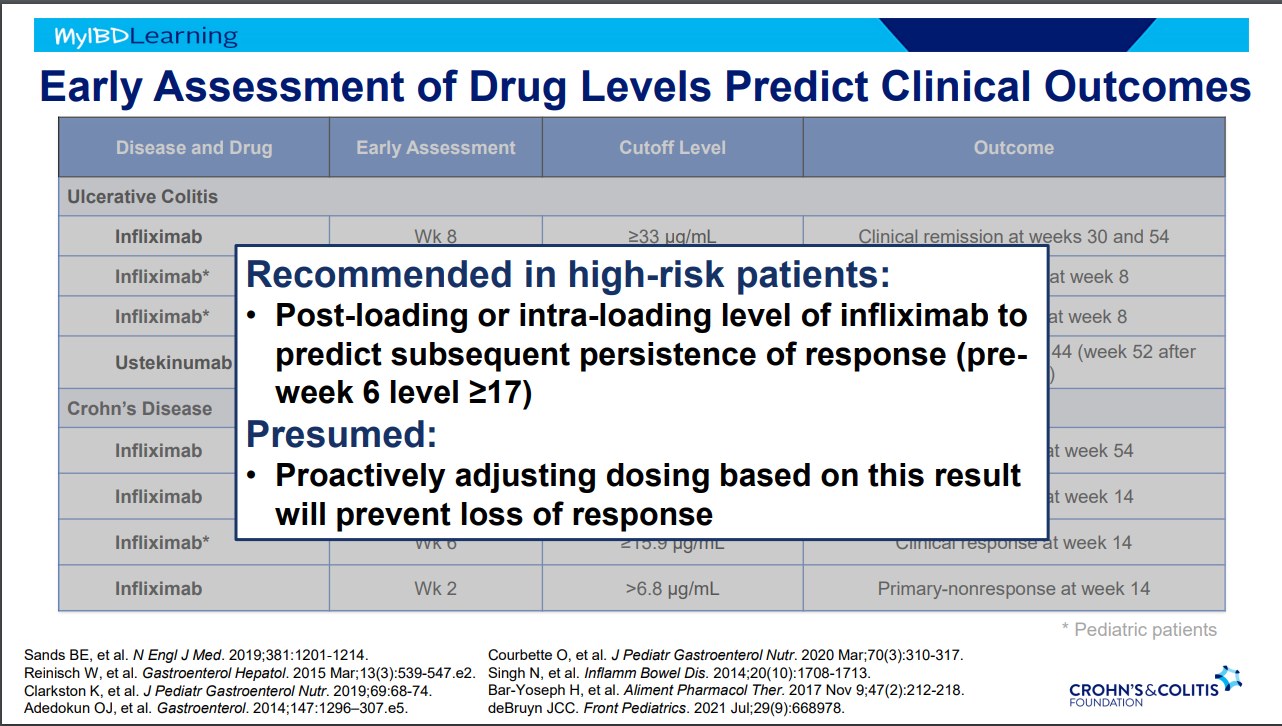
Pre-week 6 level of 17 or greater, associated with good response in maintenance. If level is low, presumption is that higher dosing will be beneficial.
Higher levels of infliximab trough levels needed for perianal fistula healing (improved with ciprofloxacin). Higher levels could be causally-related to healing or could be a marker that there is less inflammation and a patient is responding.
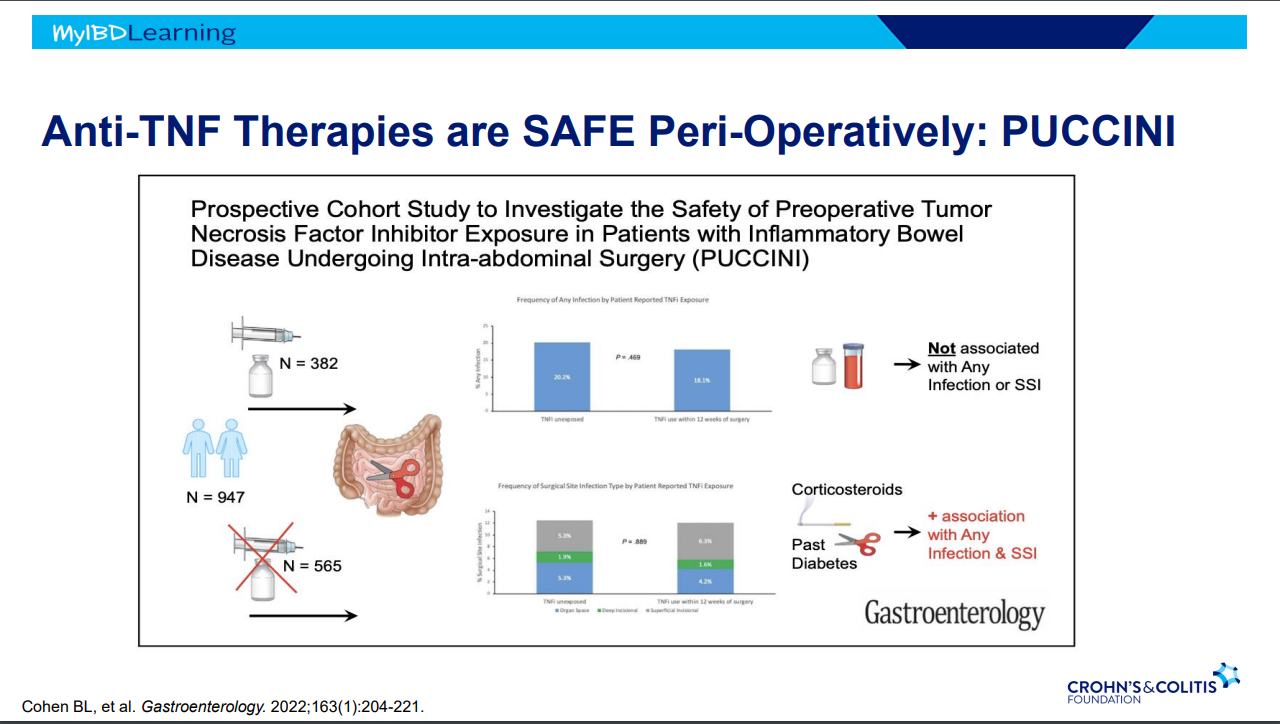
Anti-TNFs do not appear to increase risk of infections (see PUCCINI study)
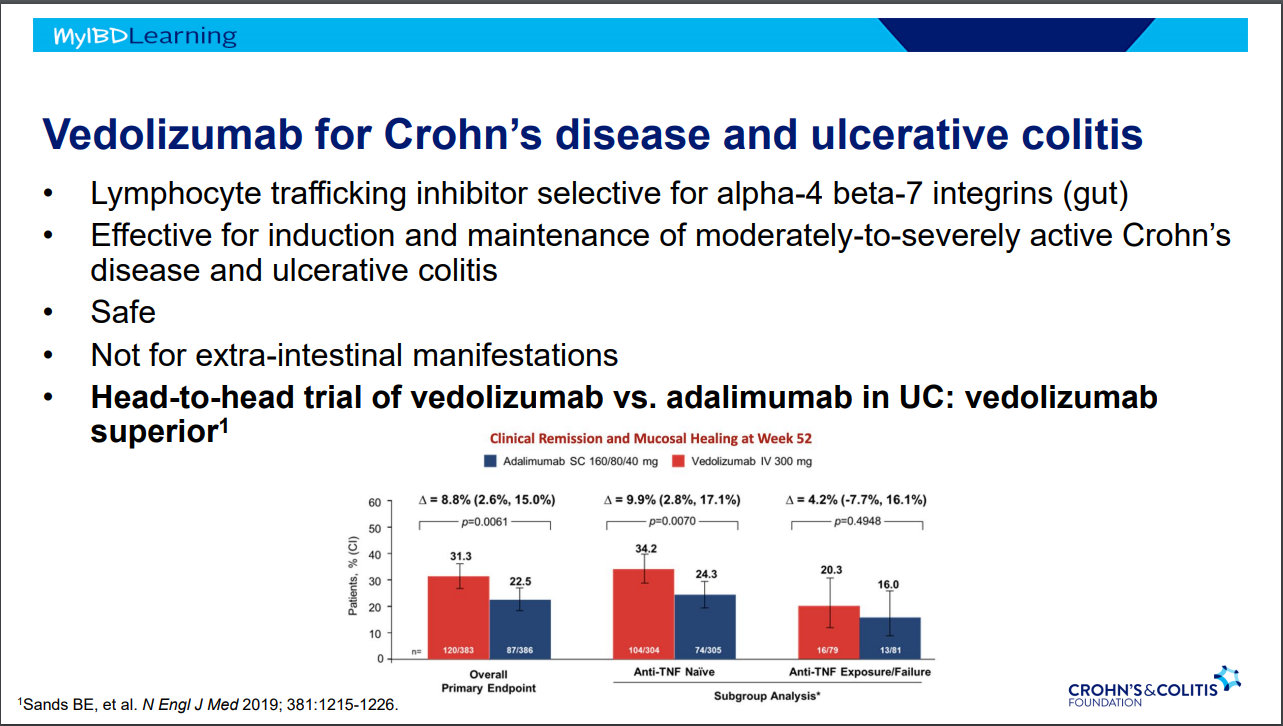
Vedolizumab -terrific safety profile. No PML, no malignancy risk
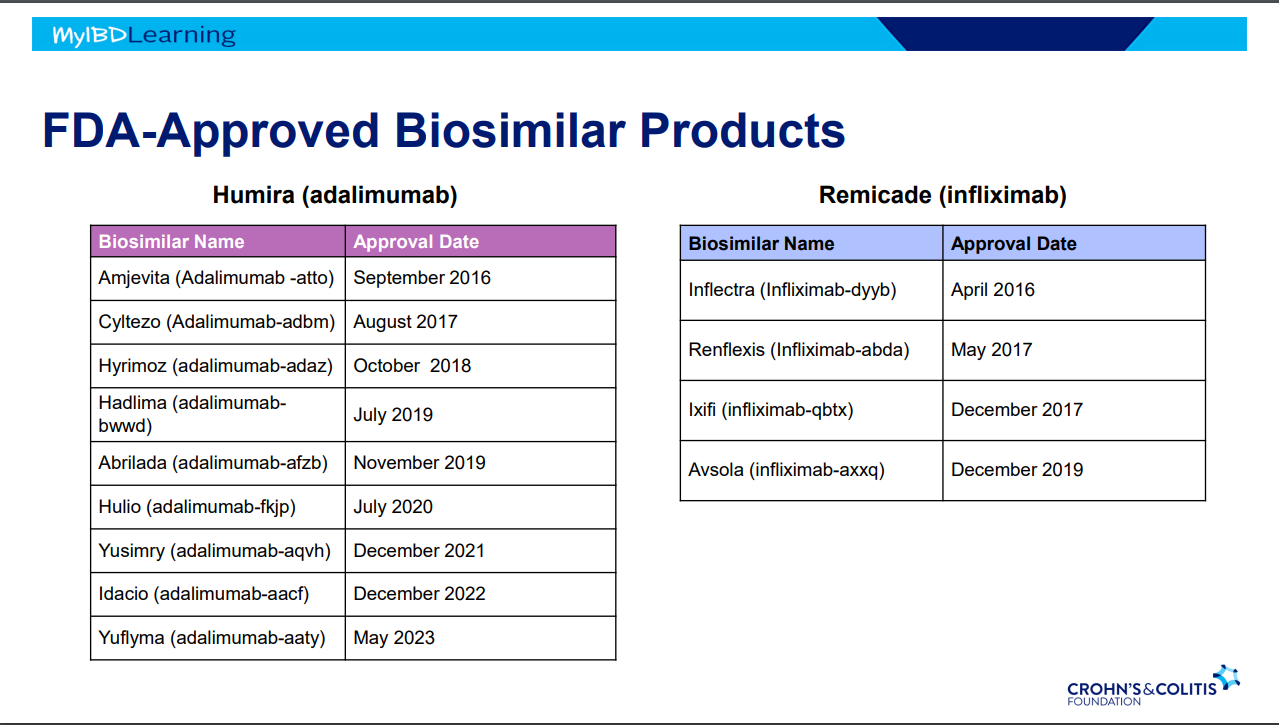
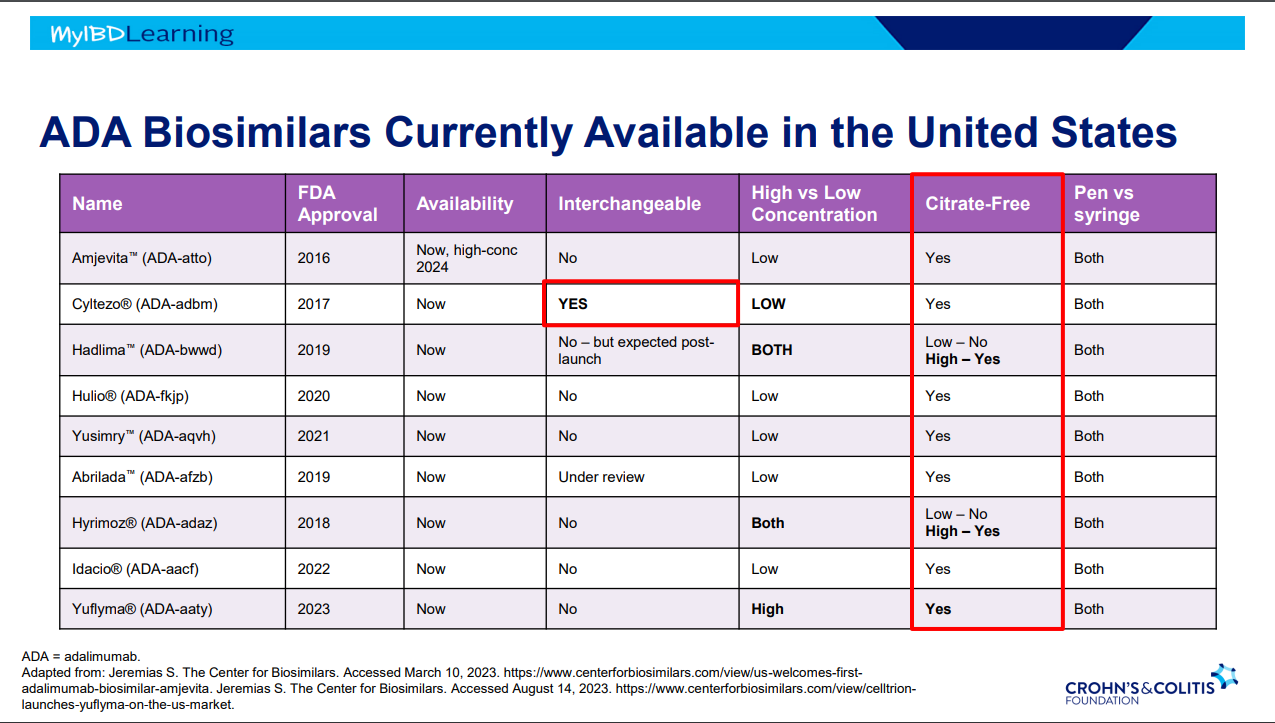
Biosimilars:
If biosimilar found effective for one approved condition, extrapolation given to all indications
IBD switching studies have NOT shown increased loss of response. Consider reassess prior to switch to help determine if patient truly in remission prior to switch. Switching often blamed for loss of response when many times the disease was not under good control prior to switch
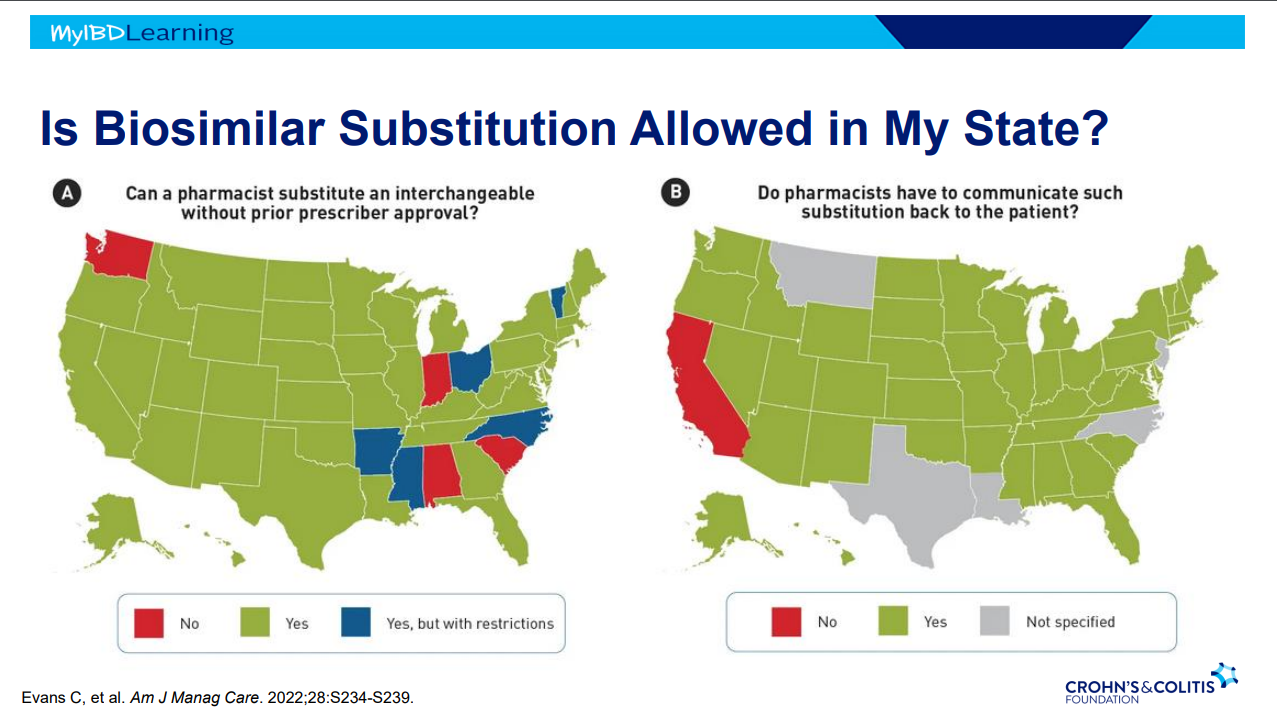
Interchangeable indicates that the drug can be switched by pharmacists
Biosimilars are saving insurers money but no proof that this is saving patients money
Anti-drug antibodies will cross-react to biosimilars
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this study, 133 ot 184 patients in clinical remission agreed to switch to subcutaneous infliximab. Key findings:
At visit 3, a relapse occurred in 10.2% (n = 6 of 59), 7.3% (n = 3 of 38), 16.7% (n = 3 of 18), and 66.7% (n = 10 of 15) (P < .001) of patients receiving 5 mg/kg every 8 weeks (5Q8W), 10Q8W, 10Q6W, and 10Q4W, respectively.
Dose escalation to 240 mg every other week led to recapture clinical remission in 93.3% (n = 14 of 15).
Infliximab serum levels increased after the switch (P < .0001) except for patients receiving 10 mg/kg every 4 weeks.
Conclusion (borrowed from authors): Switching from intravenous to subcutaneous infliximab 120 mg every other week is safe and well accepted, leading to a low risk of relapse in IBD patients except for those receiving 10Q4W; these patients likely require 240 mg every other week
Reduced (41.7%) or stable (36.8%) serum levels of IFX after the switch (difference: V1-V0) were associated with higher risk of relapse than increased serum levels (>1 μg/mL; 12.7%; P = .020 and P = .019, respectively)
Patients receiving IV infusion of IFX 10Q4W had a higher risk of relapse (odds ratio, 12.4; P = .017). In addition to having significantly higher serum levels than in other IFX IV regimens, this group of patients did not see a rise in IFX concentrations at V1, in contrast to other IFX regimens.
Being overweight increases the clearance of CT-P13 SC, with an increase in clearance of 43.2% for a weight increase from 70 to 120 kg. The presence of antibodies to IFX also increases clearance by 39%. Finally, a decrease in serum albumin level (42 g/L vs 3.2 g/L) increases the clearance by 30.1%.
My take:
Monitoring IFX levels would be helpful in patients switching from IV to SC administration, especially in higher risk groups (eg. high baseline dosing, positive anti-drug antibodies, low serum albumin, overweight individuals)
My experience with SC biologics has been that there is a much higher rate of non-adherence than with IV infusions. If/when SC biologics are used more often, I will need to implement more intensive followup to assure patients receive both the needed medication and the needed monitoring.
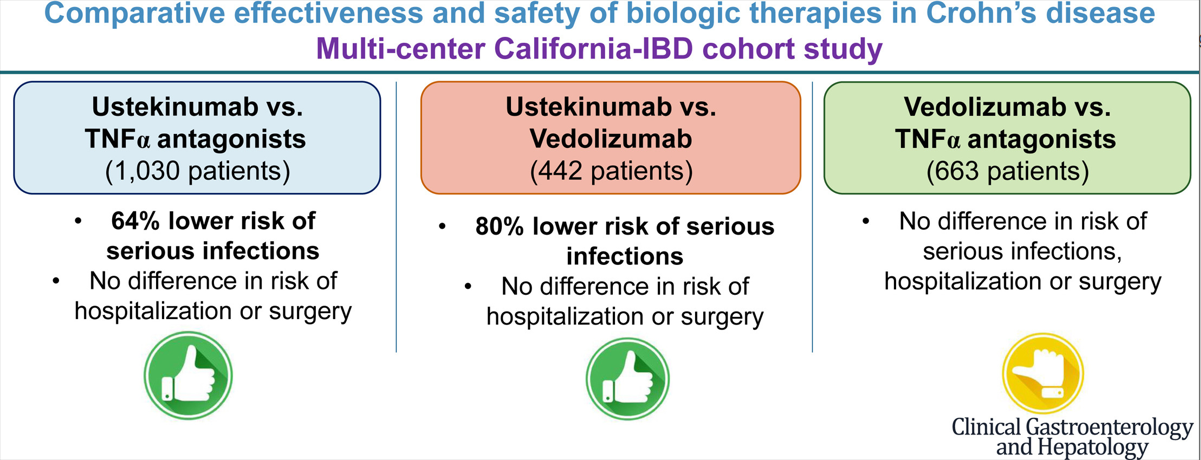
There is limited head-to-head data comparing the effectiveness of the biologics used for inflammatory bowel disease. In this study, the authors used a “series of propensity score (PS)-matched cohort studies comparing TNF-α antagonists vs vedolizumab vs ustekinumab in a large, diverse, multicenter, electronic health record (EHR)-based cohort.”
This graphical abstract summarizes the findings, though the first cohort (ustekinumab vs TNFalpha population is actually 1545 not 1030):
Key findings:
Ustekinumab-treated patients with CD (n = 515) experienced a lower risk of serious infections (hazard ratio [HR], 0.36), without any difference in the risk of hospitalization (HR, 0.99) or surgery (HR, 1.08) -compared to patients receiving TNF alpha antagonists (n=1030)
Ustekinumab-treated patients with CD (n = 221) experienced a lower risk of serious infections (HR, 0.20), without significant differences in risk of hospitalization (HR, 0.76) or surgery (HR, 1.42) -compared to vedolizumab-treated patients (n=221)
Compared with TNF-α antagonists (n = 442), vedolizumab-treated patients with CD (n = 221) had a similar risk of serious infections (HR, 1.53), hospitalization (HR, 1.32), and surgery (HR, 0.63).
The increase rate of infections with vedolizumab compared to ustekinumab could be an indication of lower efficacy with vedolizumab as the medication itself has a high safety profile.
In the discussion, the authors comment further on head-to-head studies and lack of these as well. “Biemans et al23 observed that ustekinumab-treated patients were more likely to achieve corticosteroid-free clinical remission (69 patients in each arm, vs vedolizumab; 46.4% vs 29.0%; P = .04) and biochemical remission (42.1% vs 13.2%; P = .01) at 12 months, although these rates were not significant at earlier time points.”
My take: This study provides further evidence that ustekinumab is a good option for Crohn’s disease with regard to both safety and efficacy.