Pictures from today’s CCFA Fundraiser -we had about 25 GI Care for Kids staff/family attending this year; this is not including Skittles (the dog)



Related blog post: Healthcare Hero: Dr. Benjamin Gold

Pictures from today’s CCFA Fundraiser -we had about 25 GI Care for Kids staff/family attending this year; this is not including Skittles (the dog)
Related blog post: Healthcare Hero: Dr. Benjamin Gold
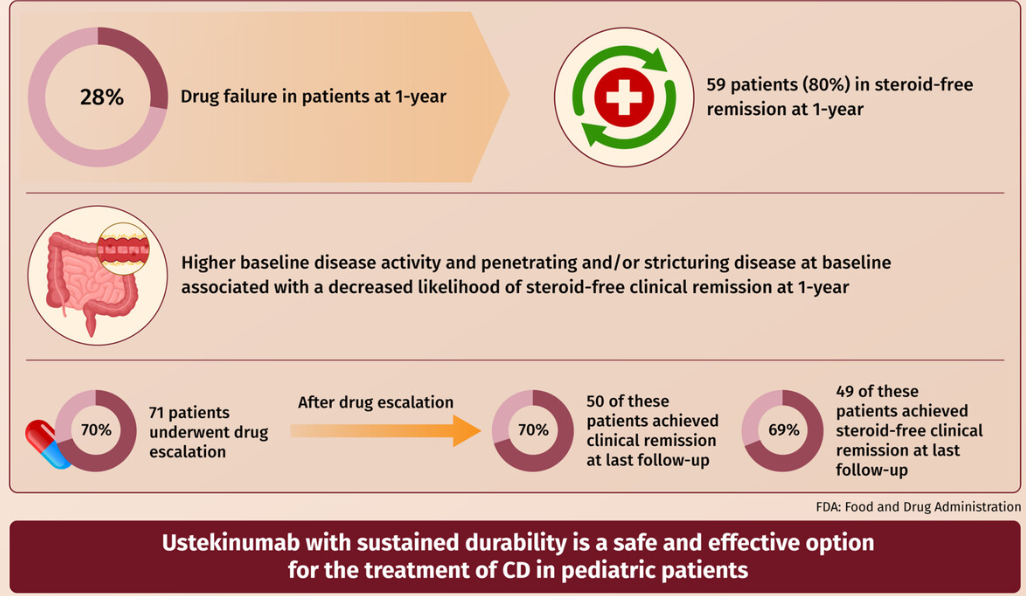
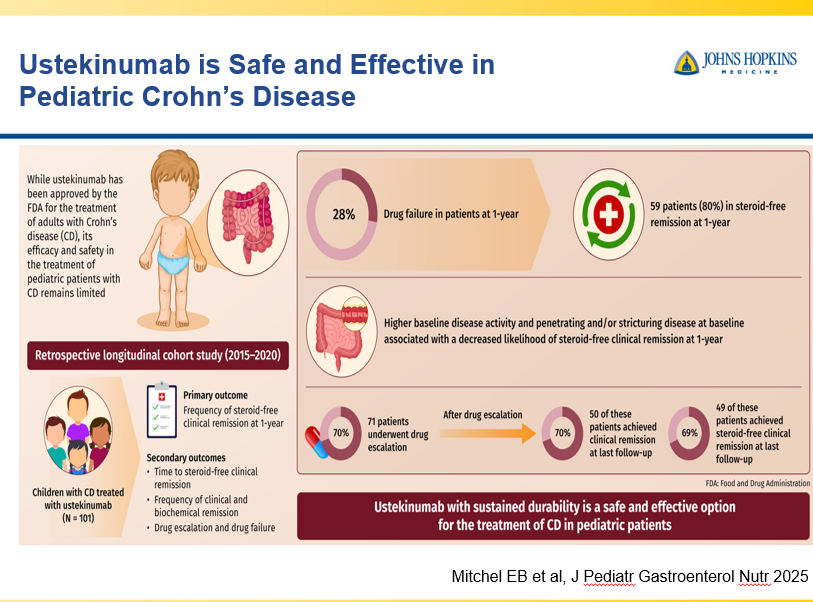
EB Mitchell et al. JPGN 2025;80:653–663. Ustekinumab is safe and effective in pediatric patients with Crohn’s disease
This was a retrospective longitudinal cohort study of 101 children with CD treated with ustekinumab from two large centers between 2015 and 2020. The median follow-up time on ustekinumab was 16.6 months.
Key findings:
My take: More pediatric data showing efficacy for ustekinumab is important. My sense, though, is that newer IL-23 specific agents are going to eclipse ustekinumab in pediatrics as they are doing in adults.
Related blog posts:
J Burisch et al. Clin Gastroenterol Hepatol 2025; 23: 386-395. Open Access! The Cost of Inflammatory Bowel Disease Care: How to Make it Sustainable
This article is a terrific review of care cost drivers in inflammatory bowel disease (IBD) but it does not actually have useful information on how to make the costs of care sustainable.
Key points:
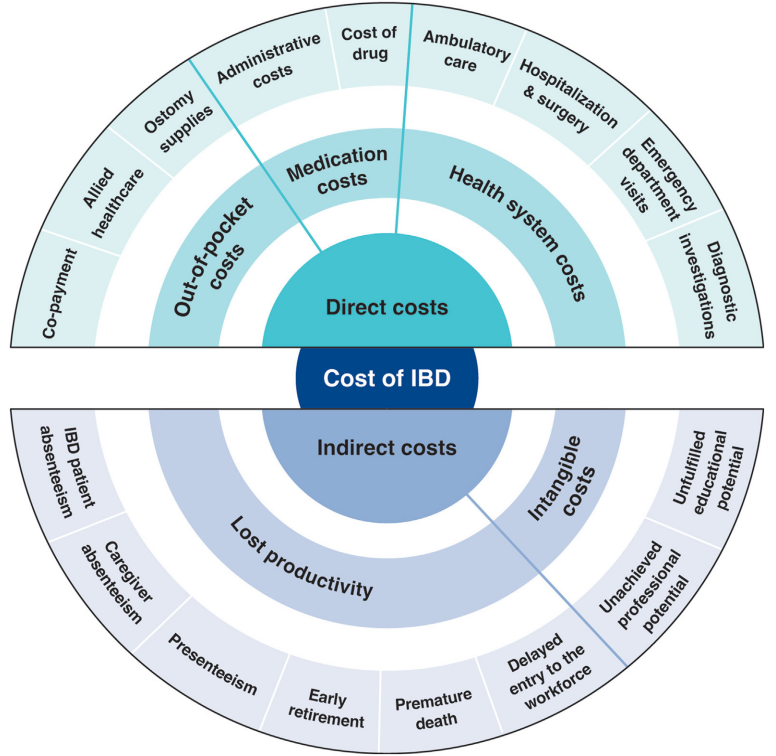
In terms of improving cost sustainability, here is what the authors propose “Strategies for cost reduction in the clinical treatment of IBD”:
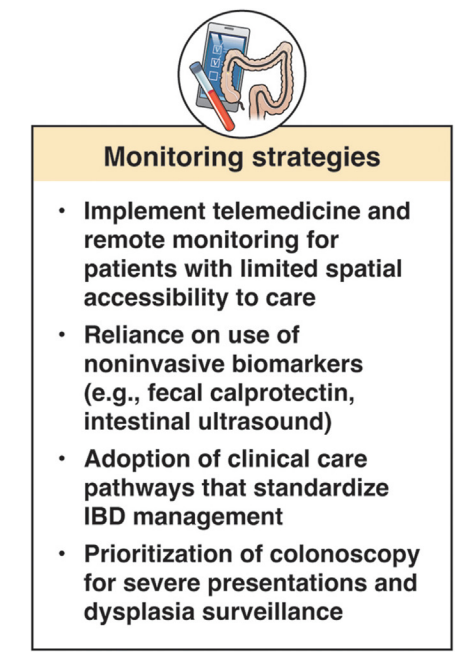
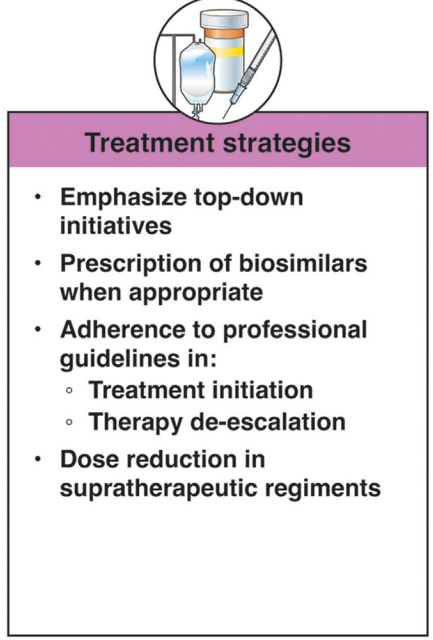
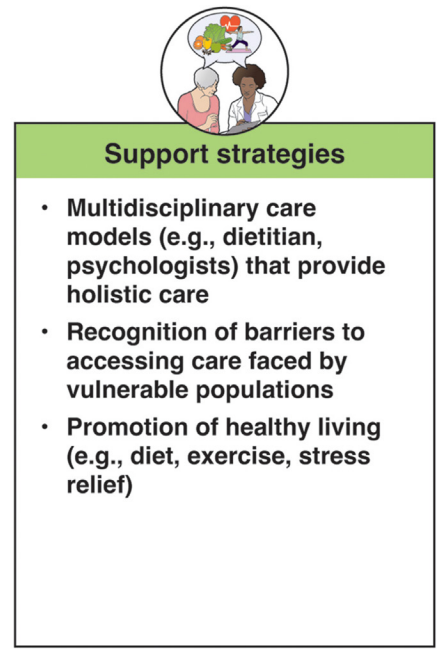
My take: This article highlights the cost drivers in IBD but does not identify a path that appears to help address affordability.
This article is one of 11 articles in special issue discussing the future of IBD care.
Related blog posts:
RS Dalal et al. Clin Gastroenterol Hepatol 2025; 23: 662-664. Outcomes After Dose Intensification of Risankizumab for Crohn’s Disease
This retrospective study reviewed adults with Crohn’s disease (CD) who underwent dose intensification of maintenance from 360 mg every 8 weeks to every 6 weeks (n=11) or every 4 weeks (n=11).
Key findings:
My take: This small study suggests that the majority of patients with a loss of response to standard dosing can be recaptured with dose intensification.
Related blog posts:

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
JD Lewis et al. Clinical Gastroenterology and Hepatology. 2024; Volume 22, Issue 12, 2475 – 2486.e14. Open Access ! Provider Specialization in Inflammatory Bowel Diseases: Quality of Care and Outcomes
Methods: This was a retrospective cohort of newly diagnosed patients with IBD using data from Optum’s deidentified Clinformatics Data Mart Database (2000–2020). The study included 772 children treated by 493 providers and 2864 adults treated by 2076 providers.
Key findings:
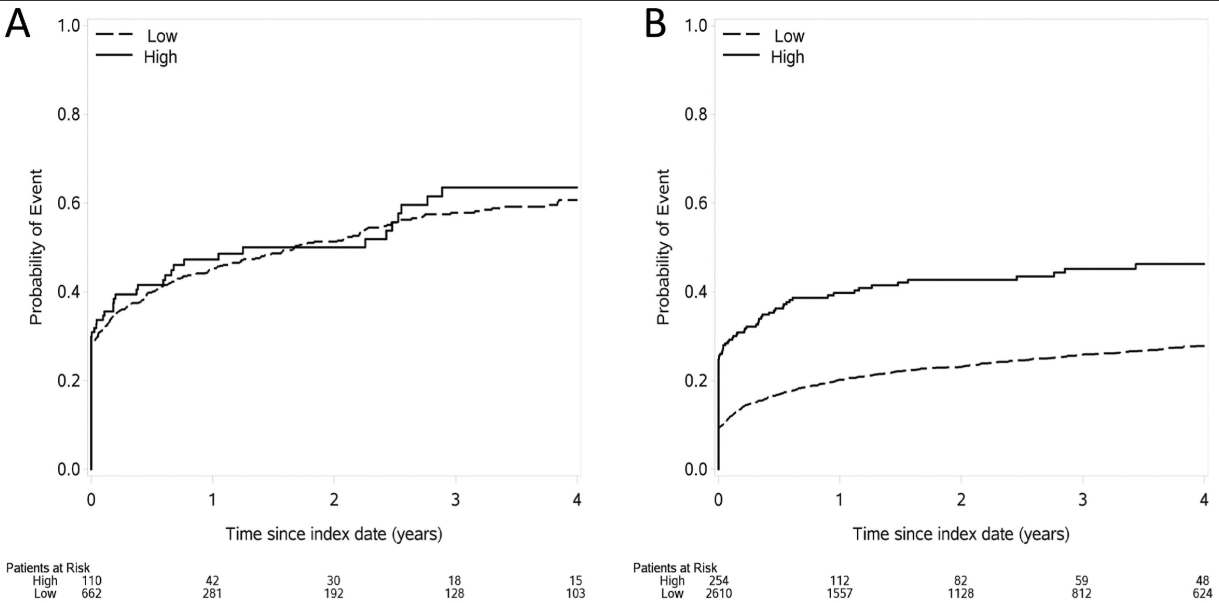
My take: This study indicates significant treatment disparities between IBD-focused care providers and providers without an IBD focus in the care for adults, but not in the care of children. This could be related to improved collaboration among pediatric care providers, better training, and parental involvement.
In addition, this study focused on patients with newly-diagnosed disease. Treatment is more complicated in patients who have not responded to initial treatments; as such, IBD-focused providers may be more important in this population.
Related blog posts:
R Panaccione et al. Clinical Gastroenterology and Hepatology 2025; In press. Open Access! Extended Risankizumab Treatment in Patients With Crohn’s Disease Who Did Not Achieve Clinical Response to Induction Treatment
Addendum -updated reference: R Panaccione et al. Clinical Gastroenterology and Hepatology 2025; 23: 2012-2022. Open Access! Extended Risankizumab Treatment in Patients With Crohn’s Disease Who Did Not Achieve Clinical Response to Induction Treatment
Methods: Per the study design, patients who did not achieve SF/APS clinical response following induction could receive 12 weeks of extended treatment with RZB, either via administration of the higher (1200 mg) IV RZB dose evaluated in ADVANCE and MOTIVATE or by initiation of SC RZB at doses (180 mg and 360 mg) used in FORTIFY maintenance therapy.
Key findings:
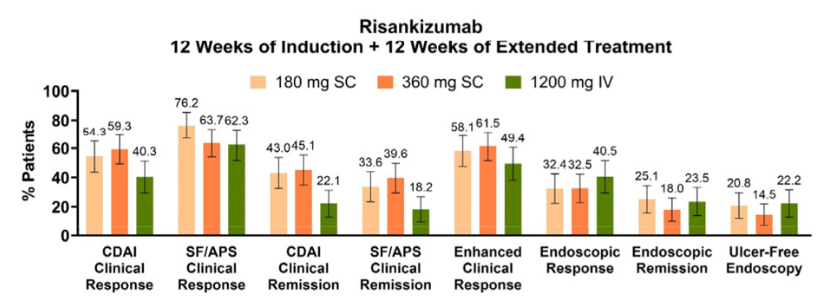
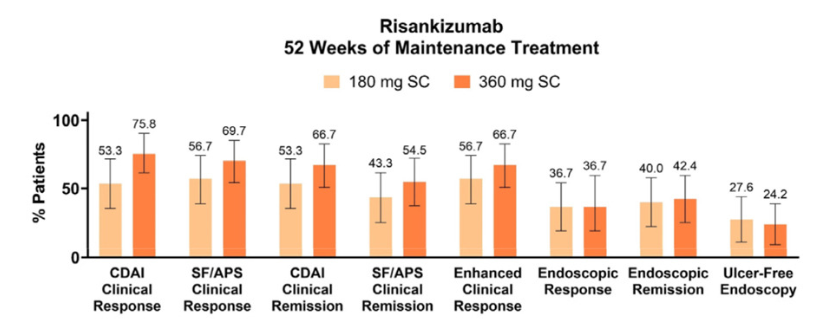

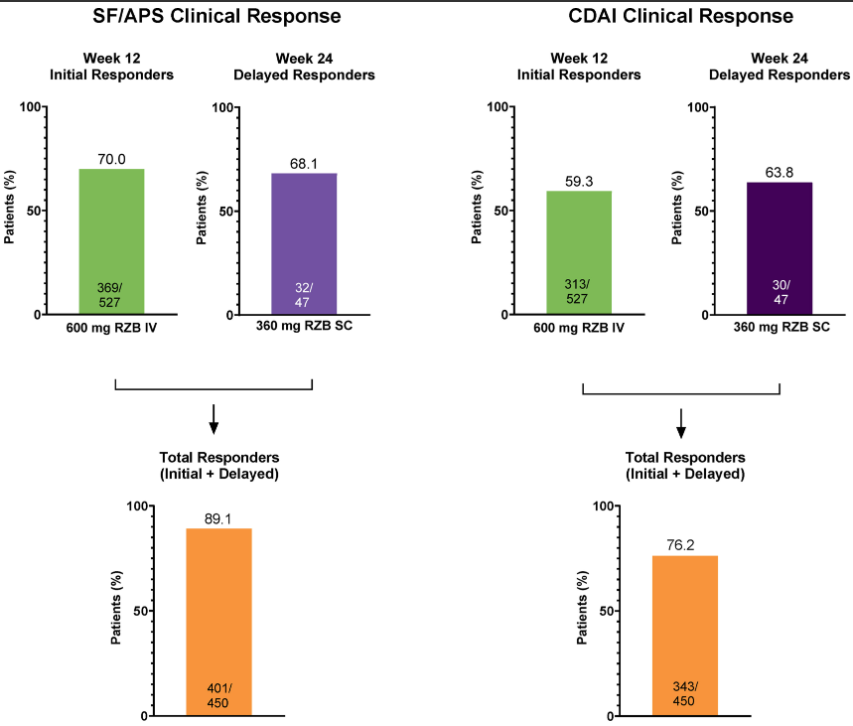
My take: While there is a very good response with initial risankizumab therapy in Crohn’s disease, it looks like judgment on response needs to wait until 24 weeks as there are many who do not respond at 12 weeks who will subsequently respond to treatment.
Related blog posts:
J McCurdy et al. AP&T 2025; https://doi.org/10.1111/apt.70081. The Impact of Setons on Perianal Fistula Outcomes in Patients With Crohn’s Disease Treated With Anti-TNF Therapy: A Multicentre Study
This study included 221 patients — 81 with setons and 140 without setons. Patients were treated with their first anti-TNF therapy for perianal fistulizing Crohn’s disease (PFCD) after undergoing a pelvic MRI between 2005 and 2022 from 6 North American centers. Our primary outcome was major adverse fistula outcome (MAFO), a composite of repeat local surgical intervention, hospitalization, or fecal diversion for PFCD.
Key findings:
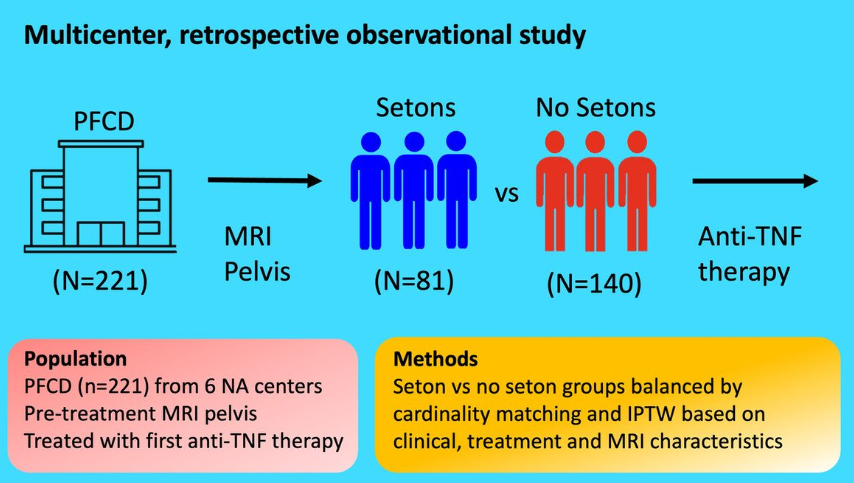
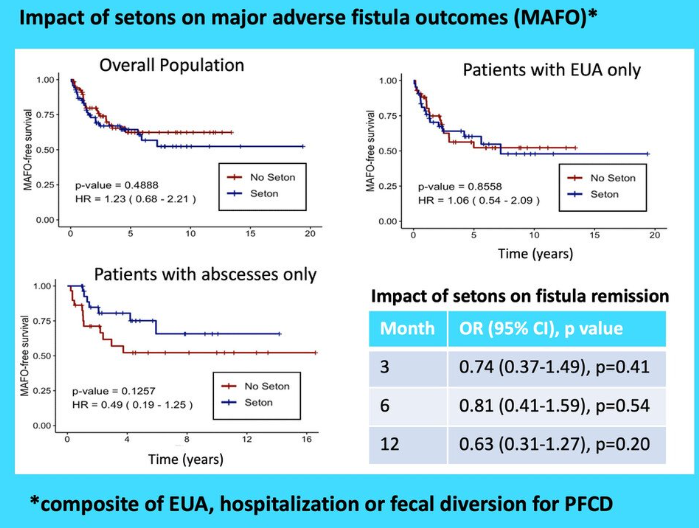
My take: This study indicates that seton placement may not be needed in patients who are starting anti-TNF therapy with fistulizing disease, especially if there is not an abscess present.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
O Atia et al. Infammatory Bowel Diseases, 2025, 31, 617–624. Durability of the First Biologic in Children and Adults With Ulcerative Colitis: A Nationwide Study from the epi-IIRN
This was a nationwide Israeli study with 15,111 patients with UC, of whom 2322 (15%) received biologics, with a median follow-up of 7.0 years. The dataset includes ~98% of the Israeli population; “the accuracy of medication data is high, as the Israeli health care system provides medications almost free of charge through the HMOs, and the electronic dispensing of drugs contributes to reliable and precise data.”
Key findings:
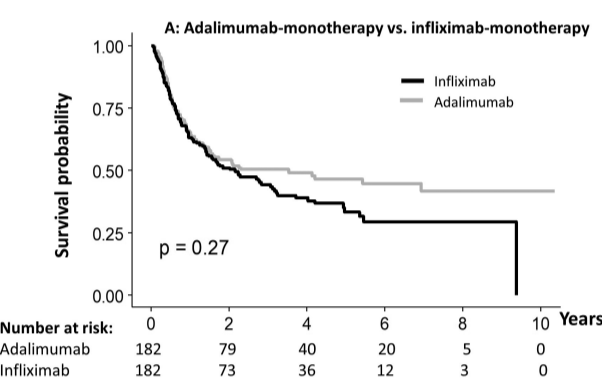
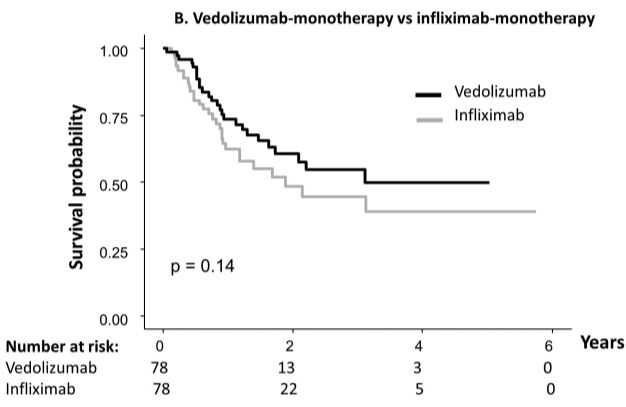
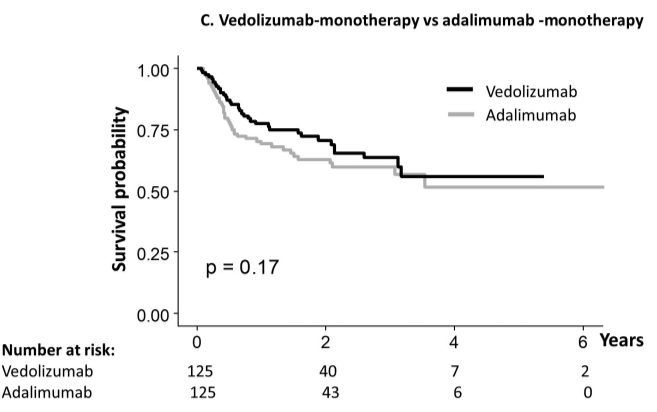
My take: When looking at the durability plots, the three main biologics in this study, infliximab, adalimumab and vedolizumab, performed similarly. Whether therapeutic drug monitoring would influence theses results is not clear. It is interesting that a recent study in the pediatric population found that combination therapy was important for adalimumab and not infliximab (see: Why Do Children Taking Adalimumab Benefit from Methotrexate Dual Therapy?)
Related blog posts:
Also, from AGA Today (3/20/25): FDA Approves Guselkumab To Treat Patients With Crohn’s Disease
HCPlive (3/20, Campbell) reports the FDA on Thursday announced the approval of “guselkumab (Tremfya) for the treatment of adults with moderately to severely active Crohn disease.” The announcement from Johnson and Johnson claims the “approval is based on data from multiple phase 3 trials, including the GALAXI trials, which found guselkumab outperformed ustekinumab (Stelara) for multiple endoscopic endpoints. The agent now boasts indications for moderately to severely active Crohn disease and moderately to severely active ulcerative colitis (UC).” This is the fourth indication for guselkumab in the US
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
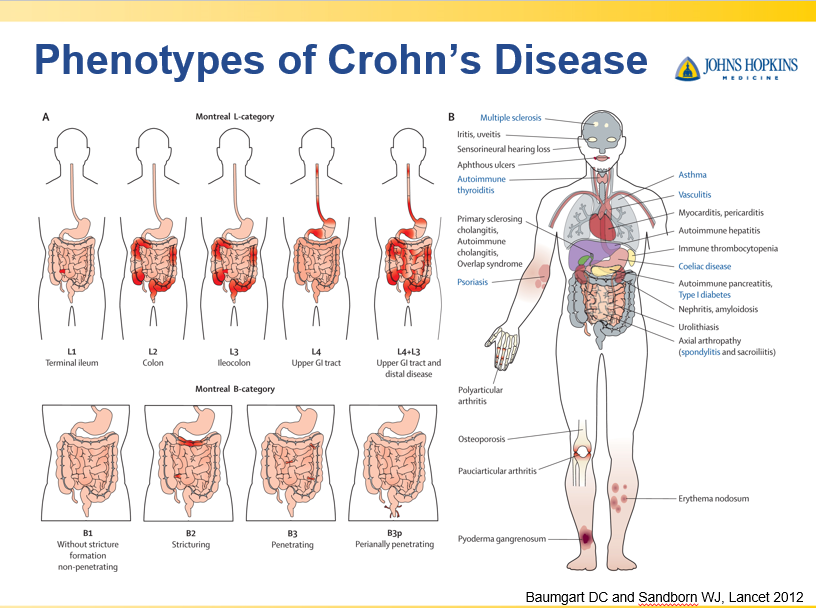
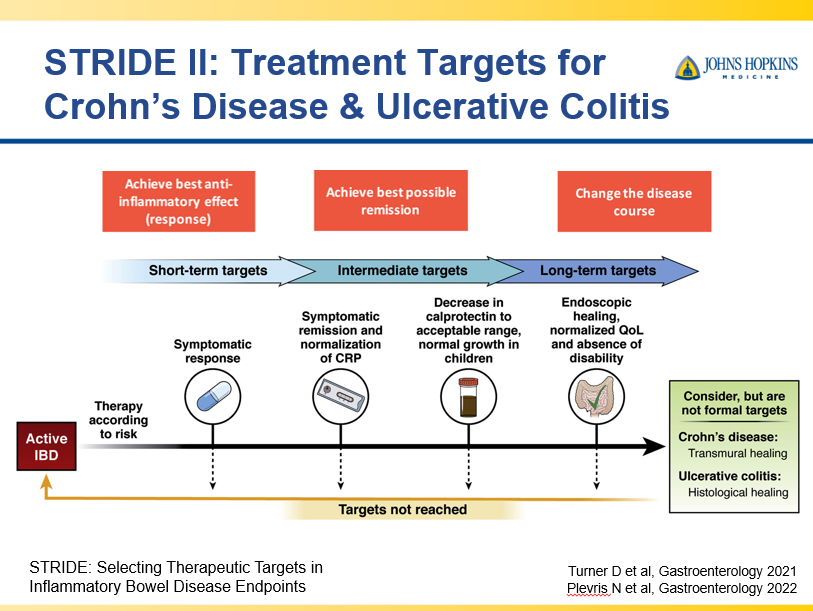
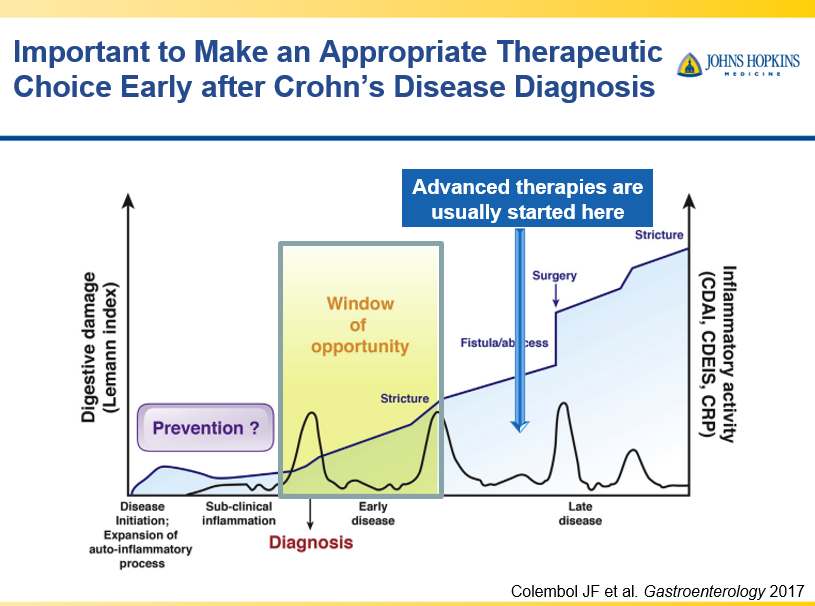
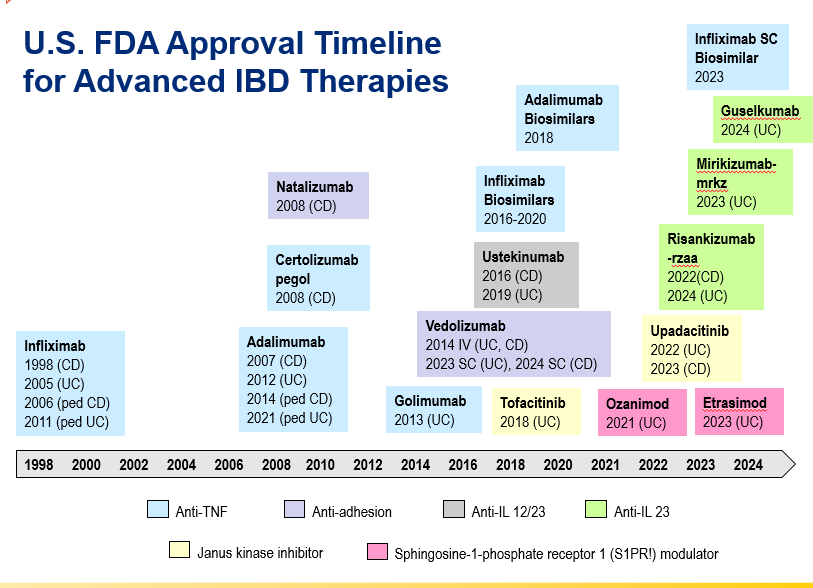
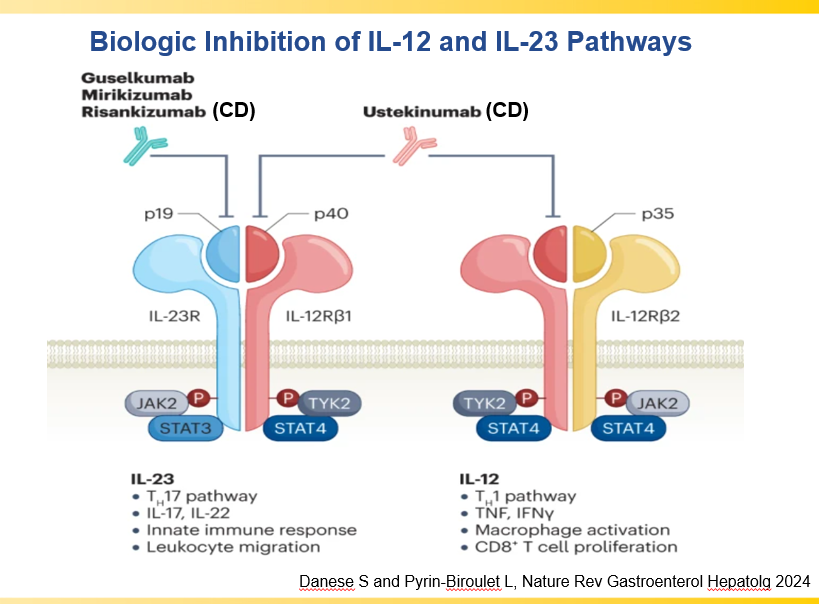
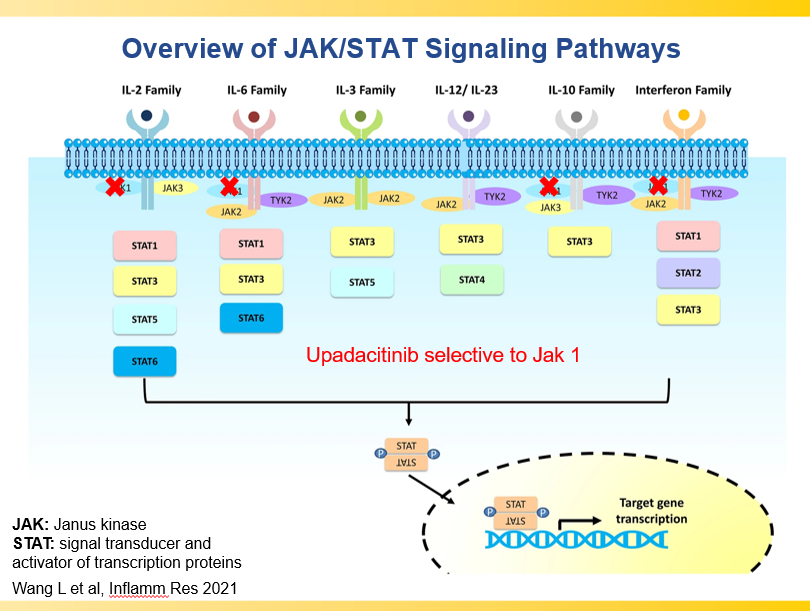
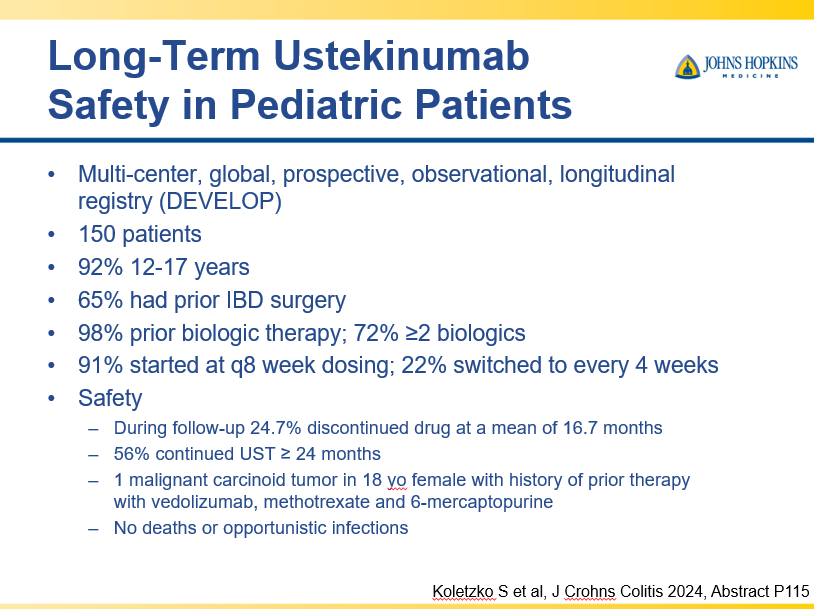
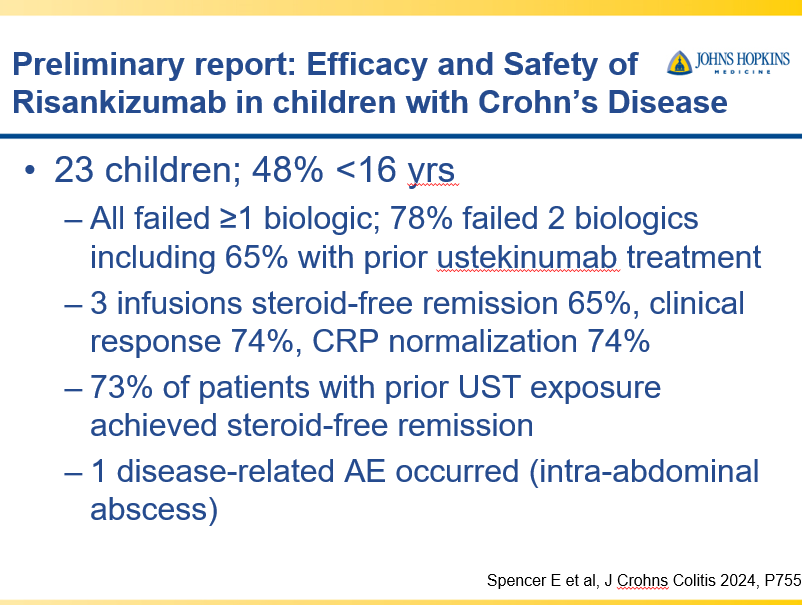
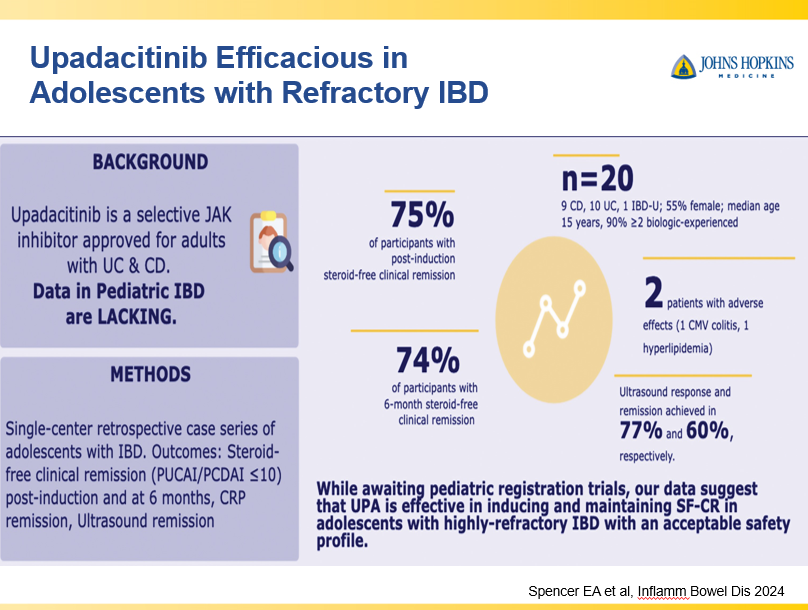
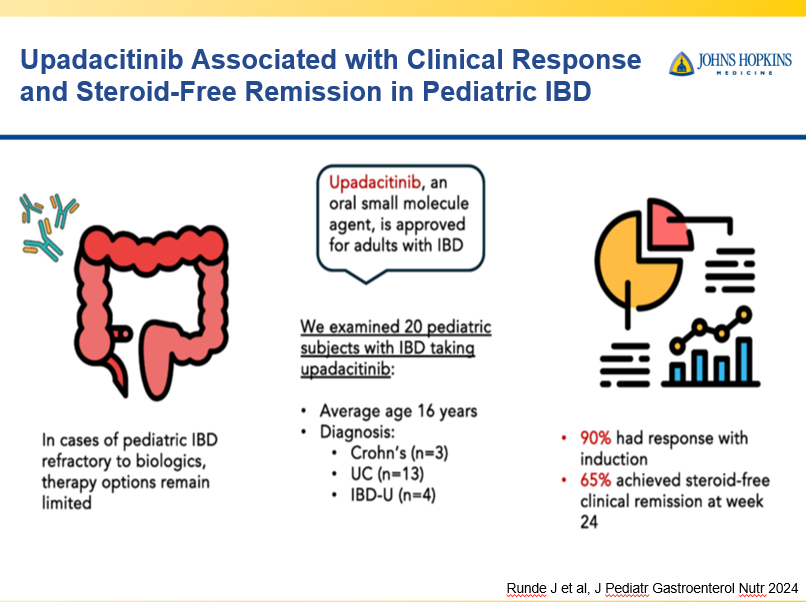
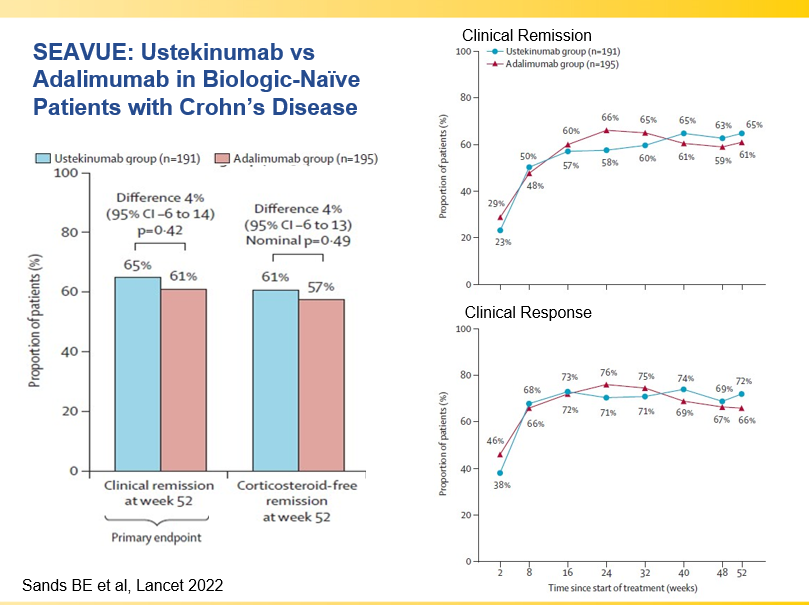
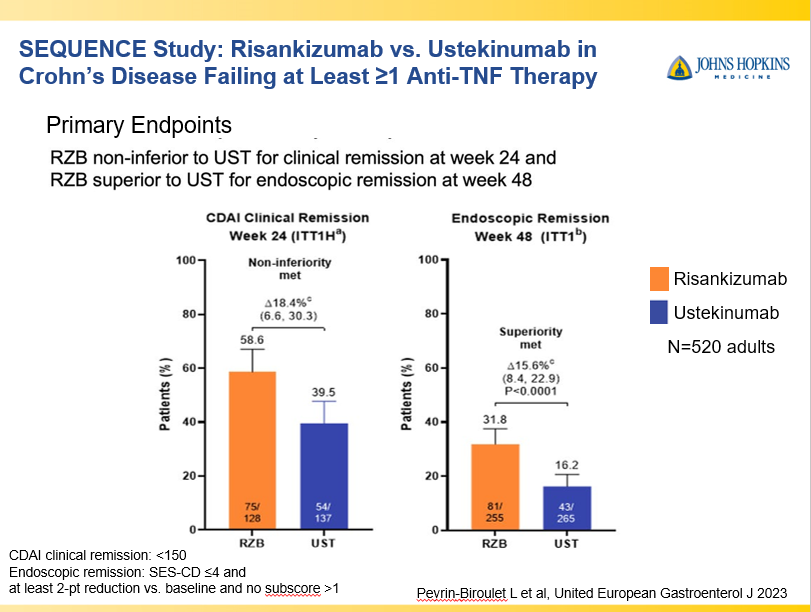
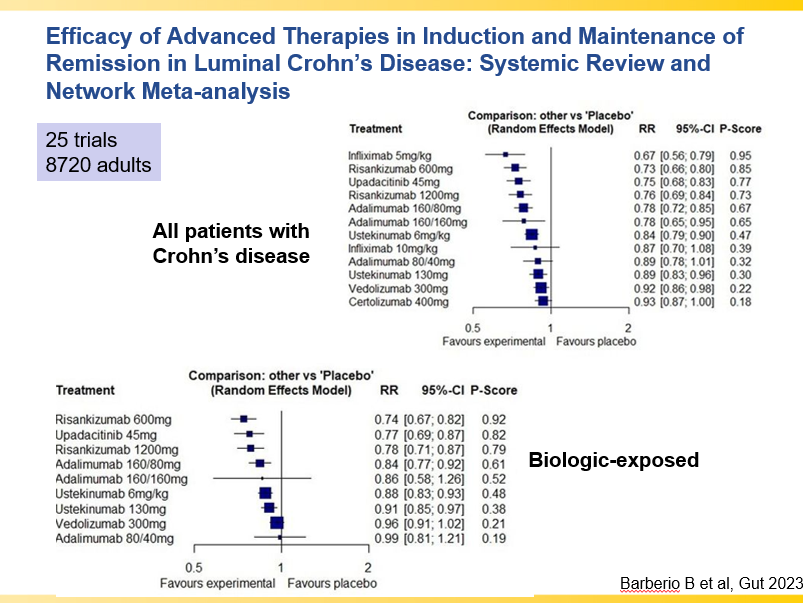
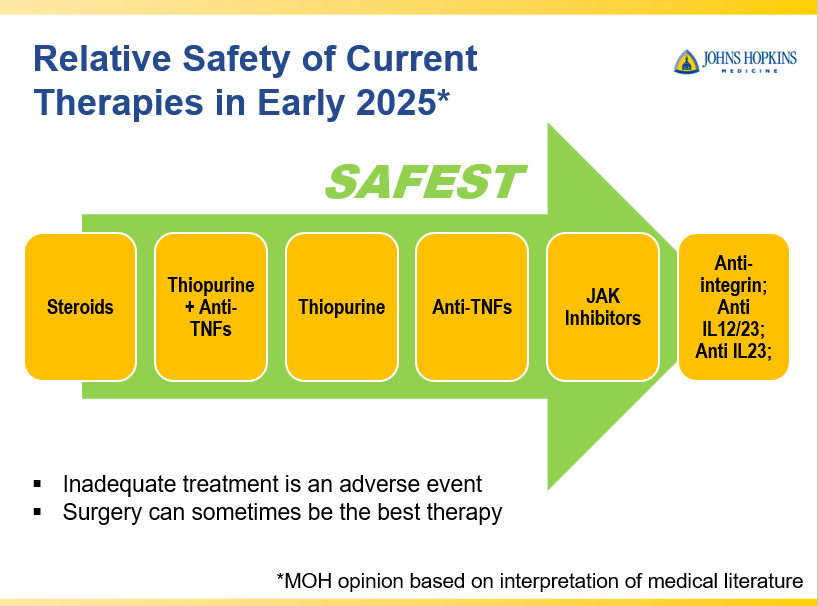
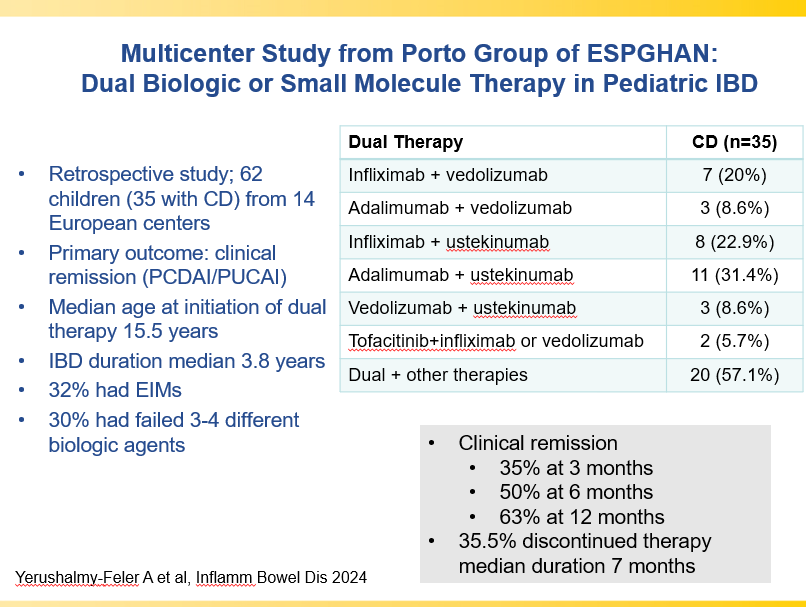
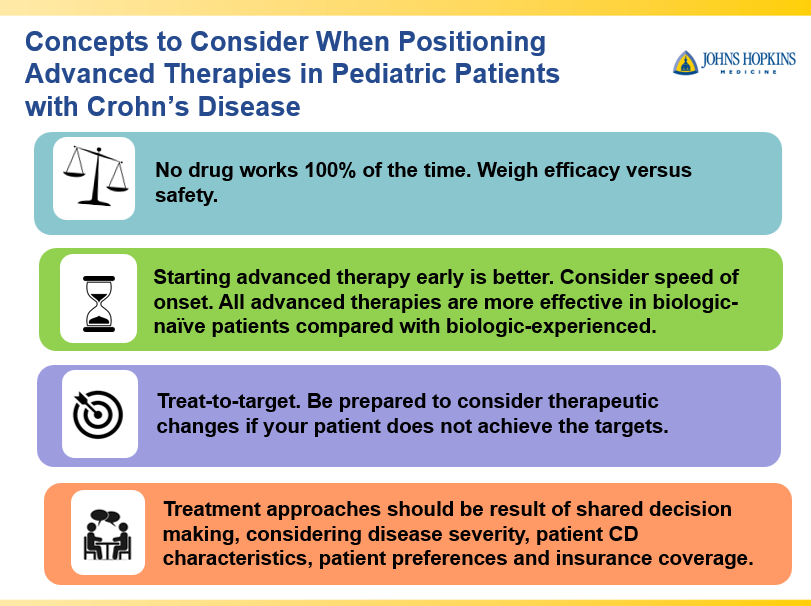
Recently, Dr. Maria Oliva-Hemker gave our group an excellent update on Crohn’s disease therapies. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
Key points:
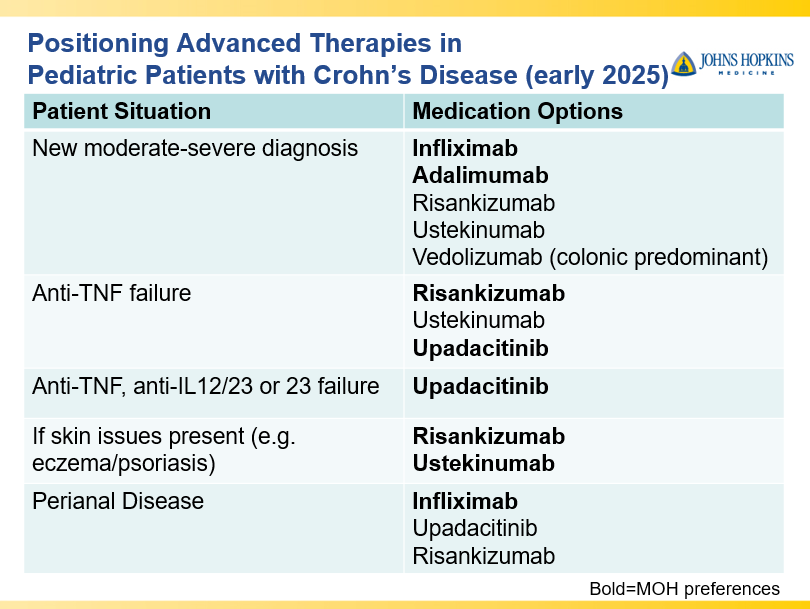
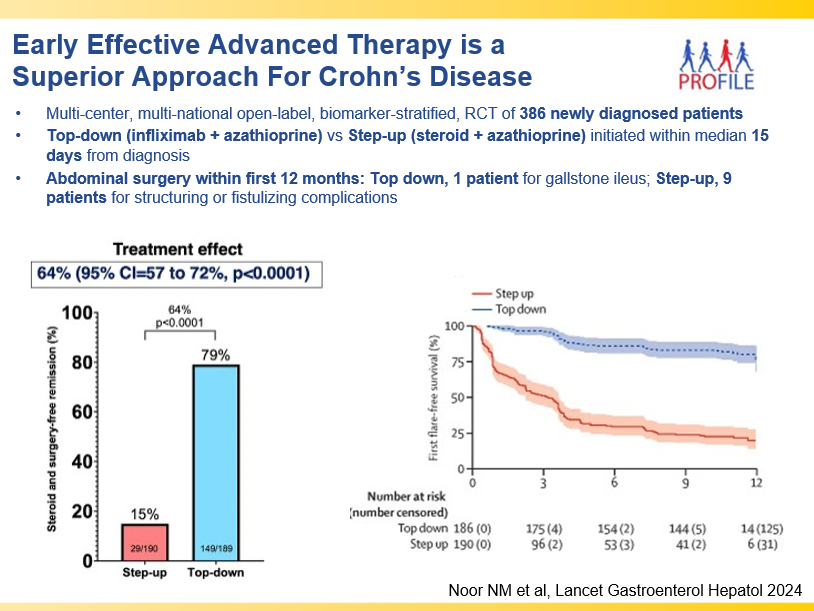
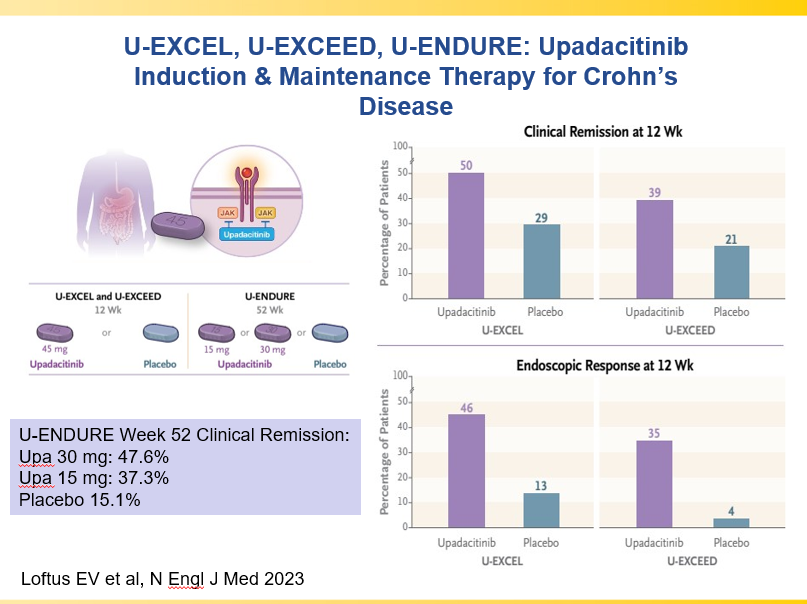
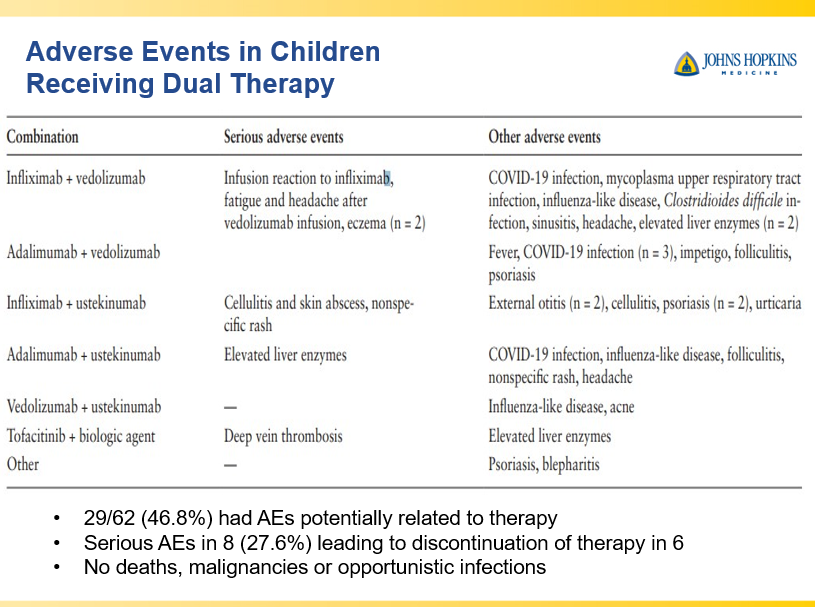
Though Dr. Oliva-Hemker’s lecture did not focus on ulcerative colitis, she did note that their center has recommended frequent colonoscopies (often yearly) in many of their patients with the combination of ulcerative colitis and PSC. This is due cases of colon cancer in their pediatric cohort.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Congratulations to Dr. Benjamin Gold who is one of the honored heros at this year’s CCFA Take Steps. Also, congratulations to Clara Cann and Lauren Leonard who are being recognized as well.
Link: Register for Take Steps 2025 (4/26/25)