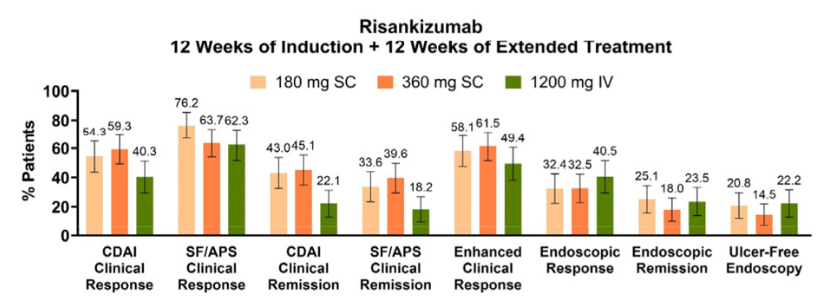
Methods: Per the study design, patients who did not achieve SF/APS clinical response following induction could receive 12 weeks of extended treatment with RZB, either via administration of the higher (1200 mg) IV RZB dose evaluated in ADVANCE and MOTIVATE or by initiation of SC RZB at doses (180 mg and 360 mg) used in FORTIFY maintenance therapy.
Key findings:
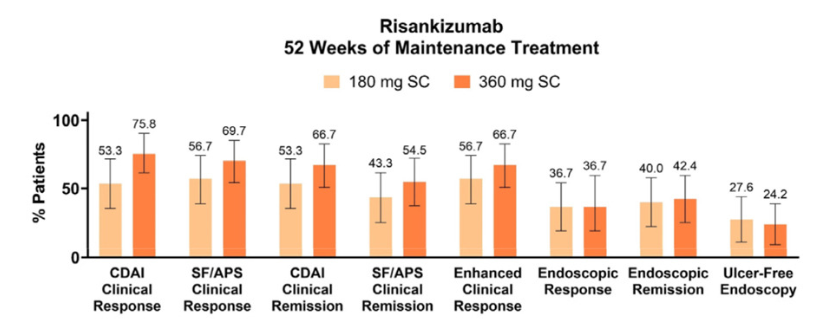
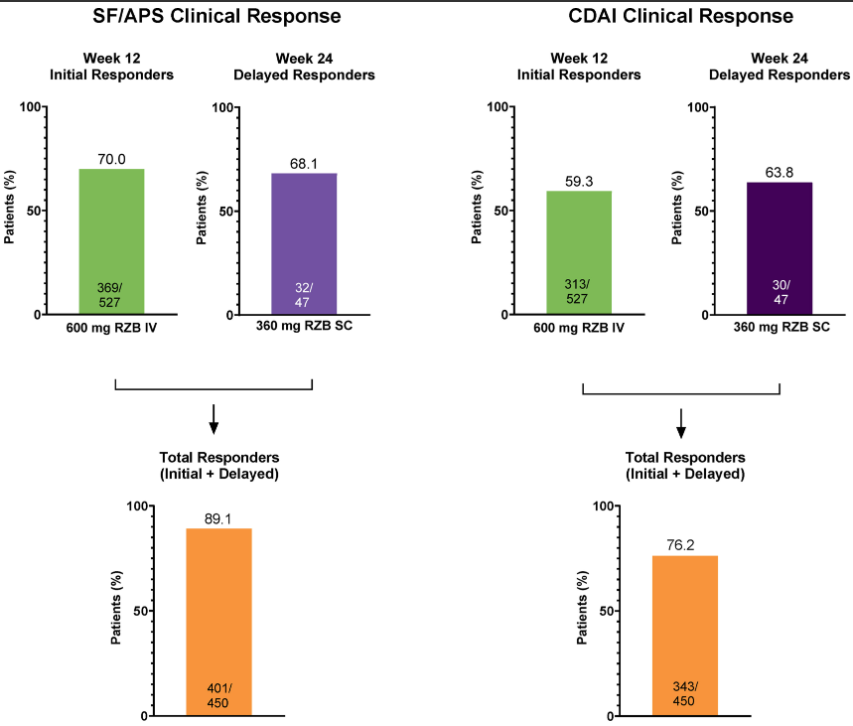
Over 60% of initial nonresponders achieved clinical response with extended RZB treatment. These patients also demonstrated improved clinical and endoscopic outcomes during the extended treatment period, which were sustained or continued to improve during maintenance.
My take: While there is a very good response with initial risankizumab therapy in Crohn’s disease, it looks like judgment on response needs to wait until 24 weeks as there are many who do not respond at 12 weeks who will subsequently respond to treatment.
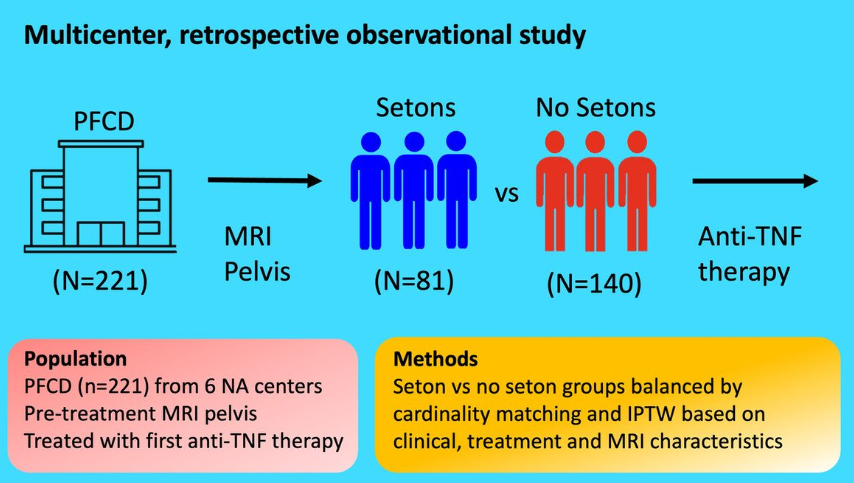
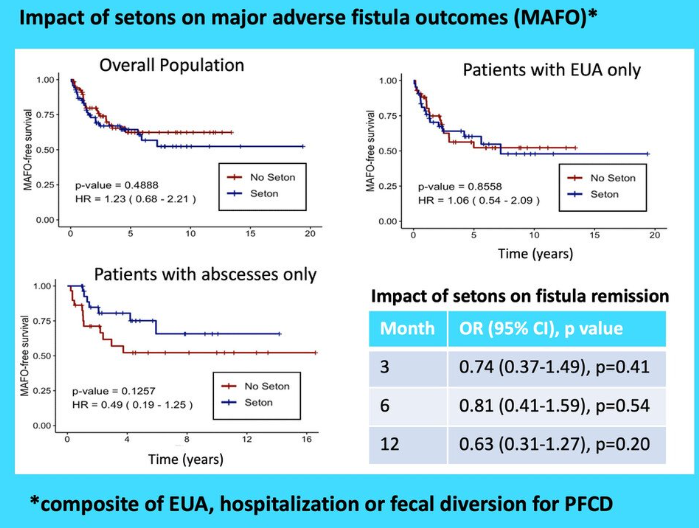
This study included 221 patients — 81 with setons and 140 without setons. Patients were treated with their first anti-TNF therapy for perianal fistulizing Crohn’s disease (PFCD) after undergoing a pelvic MRI between 2005 and 2022 from 6 North American centers. Our primary outcome was major adverse fistula outcome (MAFO), a composite of repeat local surgical intervention, hospitalization, or fecal diversion for PFCD.
Key findings:
Patients with setons had similar rates of MAFO (HR 1.23; 95% CI, 0.68–2.21) and fistula remission at 6 months (OR, 0.81; 95% CI, 0.41–1.59) and 12 months (OR, 0.63; 95% CI, 0.31–1.27) compared to patients without setons
In patients with abscesses, there were lower rates of MAFO (HR, 0.49; 95% CI, 0.19–1.25) but not statistically significant in patients with setons
My take: This study indicates that seton placement may not be needed in patients who are starting anti-TNF therapy with fistulizing disease, especially if there is not an abscess present.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This was a nationwide Israeli study with 15,111 patients with UC, of whom 2322 (15%) received biologics, with a median follow-up of 7.0 years. The dataset includes ~98% of the Israeli population; “the accuracy of medication data is high, as the Israeli health care system provides medications almost free of charge through the HMOs, and the electronic dispensing of drugs contributes to reliable and precise data.”
Key findings:
After 5 years of treatment, 43% of the patients with UC sustained their first biologic
The durability rate was similar between pediatric-onset and adults after 1 and 5 years from initiation of treatment (72% and 43% vs 71% and 43%, respectively)
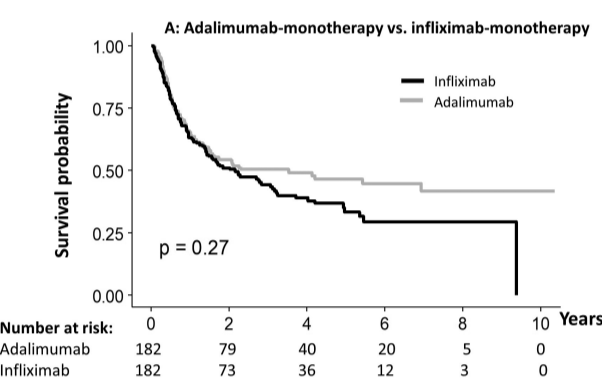
Durability of adalimumab vs infliximab after 1 or 5 years was similar, whether prescribed as monotherapy (65%/46% vs 63%/33%, respectively) or combotherapy (78%/56% vs 91%/58%, respectively)
Durability of infliximab at 1 yr and 5 yrs was higher as combotherapy (85%/50%) vs monotherapy (69%/42%; , P = .007), while it was similar for adalimumab (80%/52% vs 74%/52%)
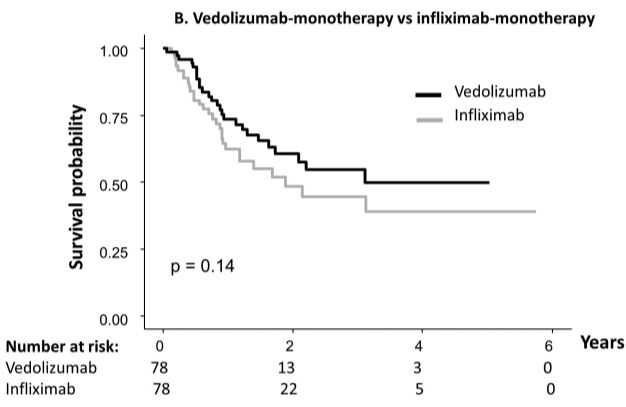
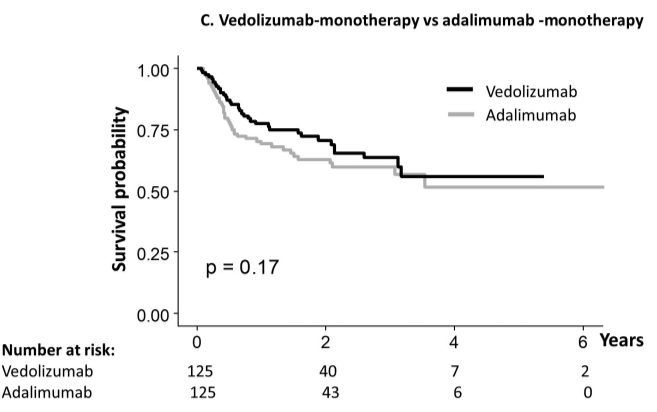
The durability rate was similar for vedolizumab monotherapy at 1 yr and 5 yrs (77%/56%) compared with adalimumab monotherapy (69%/52%), and infliximab monotherapy (73%/55% vs 62%/44%). However, combotherapy of antitumor necrosis factors (TNFs) had longer durability than vedolizumab (85%/50% vs 75%/43%), respectively;
My take: When looking at the durability plots, the three main biologics in this study, infliximab, adalimumab and vedolizumab, performed similarly. Whether therapeutic drug monitoring would influence theses results is not clear. It is interesting that a recent study in the pediatric population found that combination therapy was important for adalimumab and not infliximab (see: Why Do Children Taking Adalimumab Benefit from Methotrexate Dual Therapy?)
Also, from AGA Today (3/20/25): FDA Approves Guselkumab To Treat Patients With Crohn’s Disease
HCPlive (3/20, Campbell) reports the FDA on Thursday announced the approval of “guselkumab (Tremfya) for the treatment of adults with moderately to severely active Crohn disease.” The announcement from Johnson and Johnson claims the “approval is based on data from multiple phase 3 trials, including the GALAXI trials, which found guselkumab outperformed ustekinumab (Stelara) for multiple endoscopic endpoints. The agent now boasts indications for moderately to severely active Crohn disease and moderately to severely active ulcerative colitis (UC).” This is the fourth indication for guselkumab in the US
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Recently, Dr. Maria Oliva-Hemker gave our group an excellent update on Crohn’s disease therapies. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
Key points:
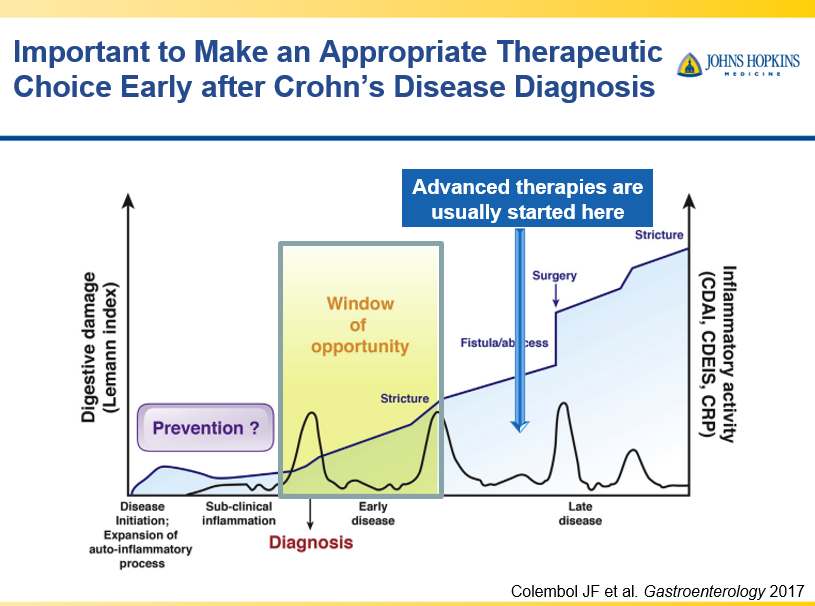
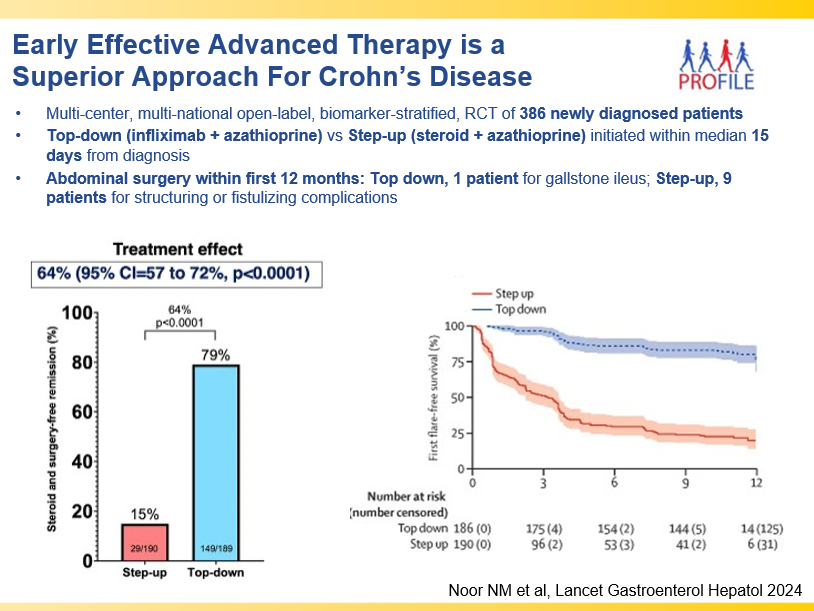
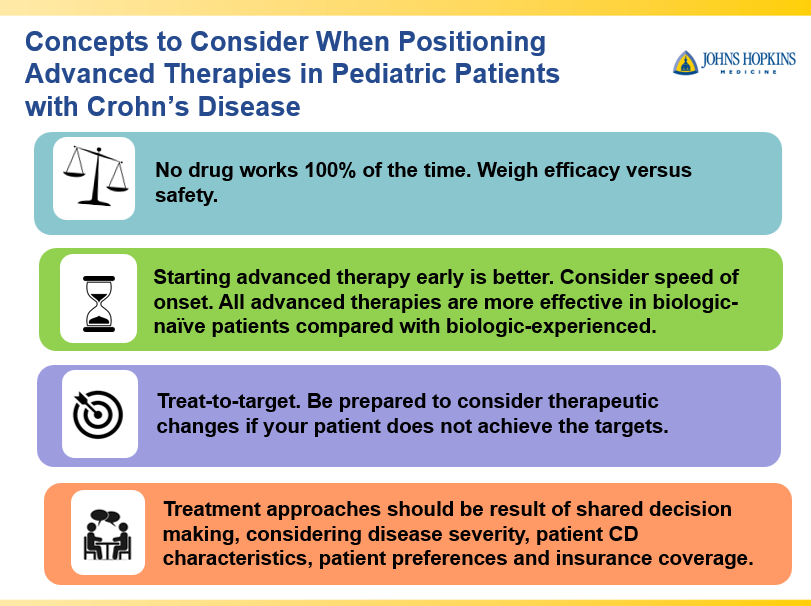
Early advanced therapy results in better outcomes (see The PROFILE study results below as one example)
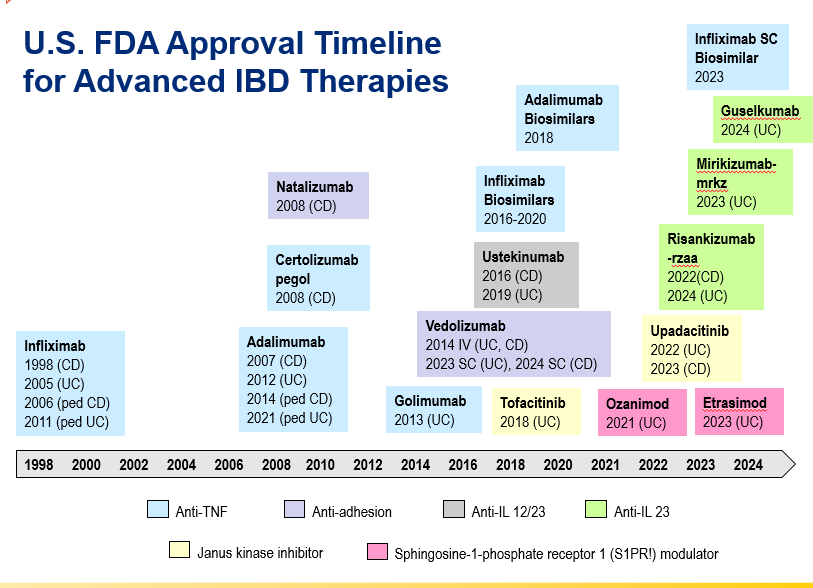
Anti-TNFs are the only therapy with a specific FDA pediatric indication. Medications can take 8-10 years after use in adults for pediatric labeling
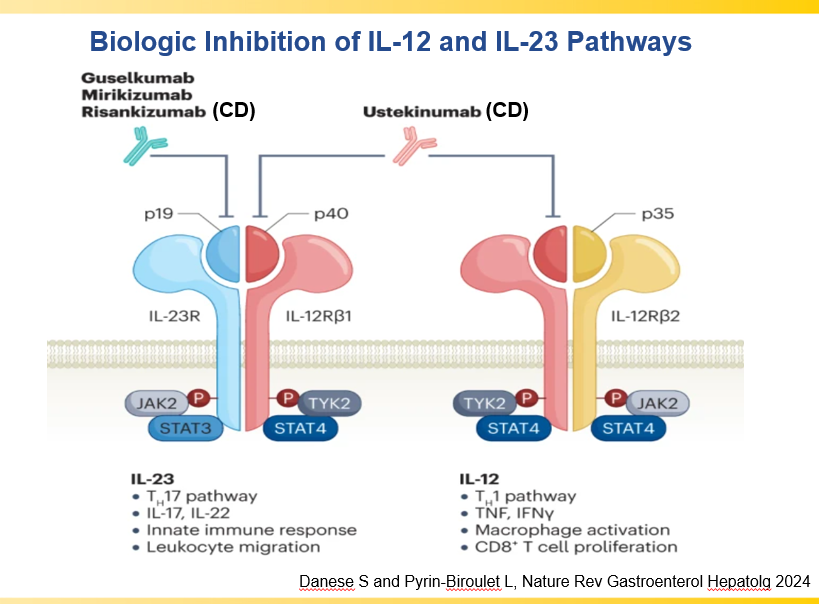
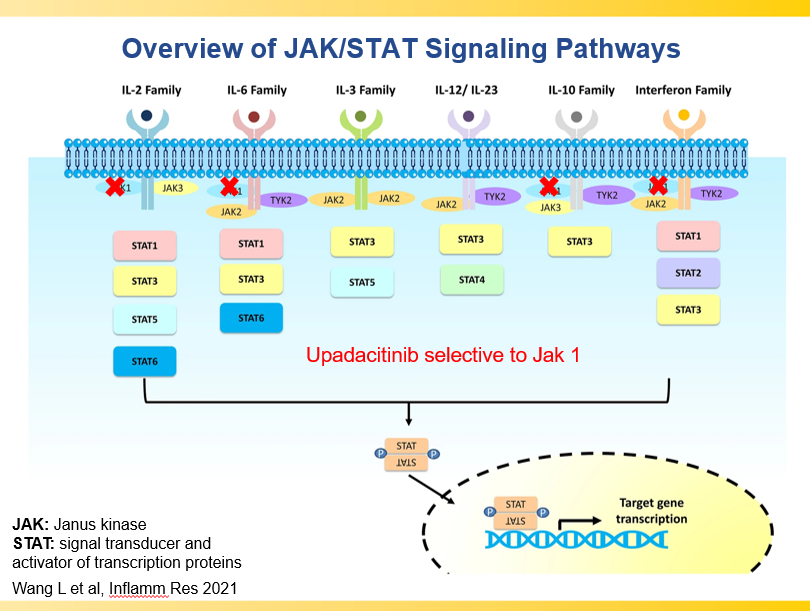
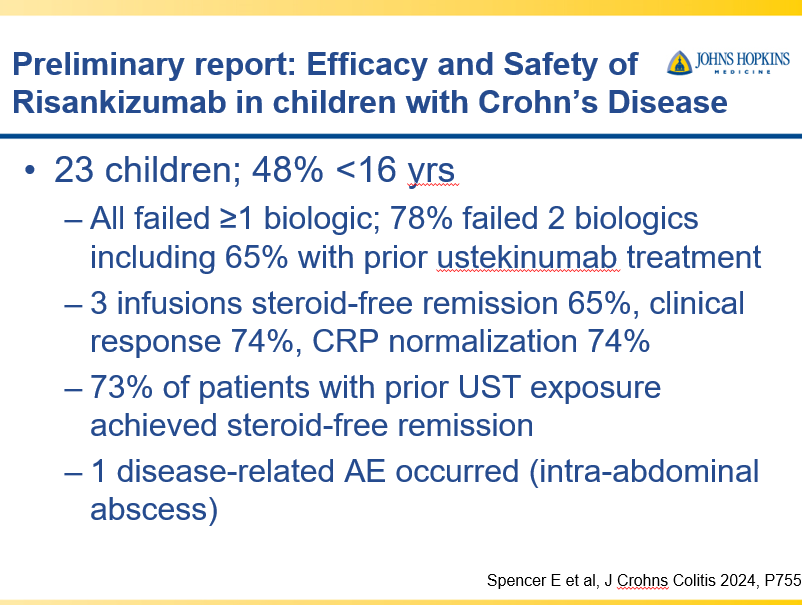
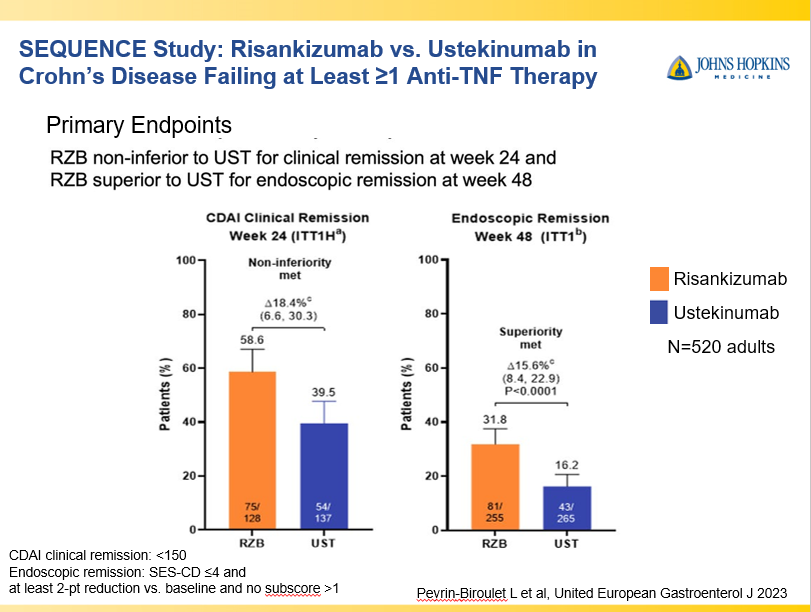
IL-23 specific agents (like risankizumab) are more effective than ustekinumab that target both IL-23/IL-12
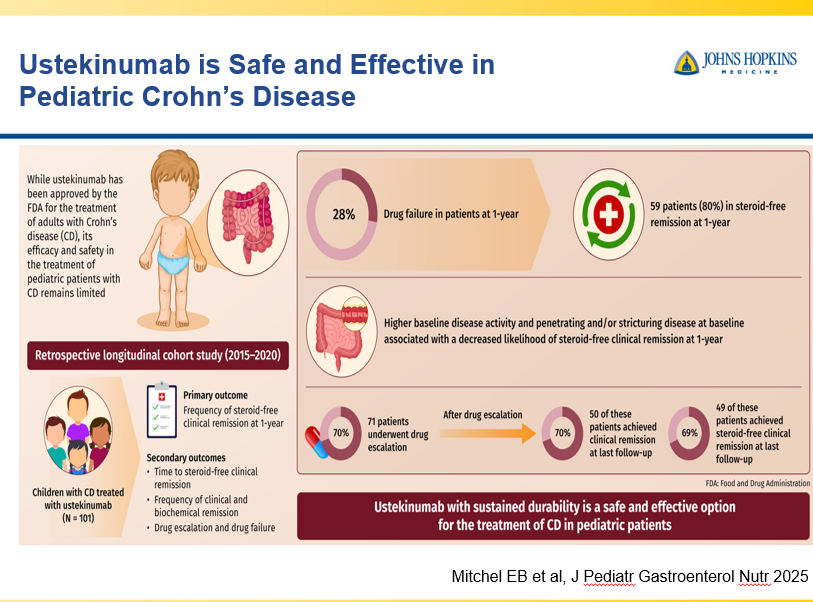
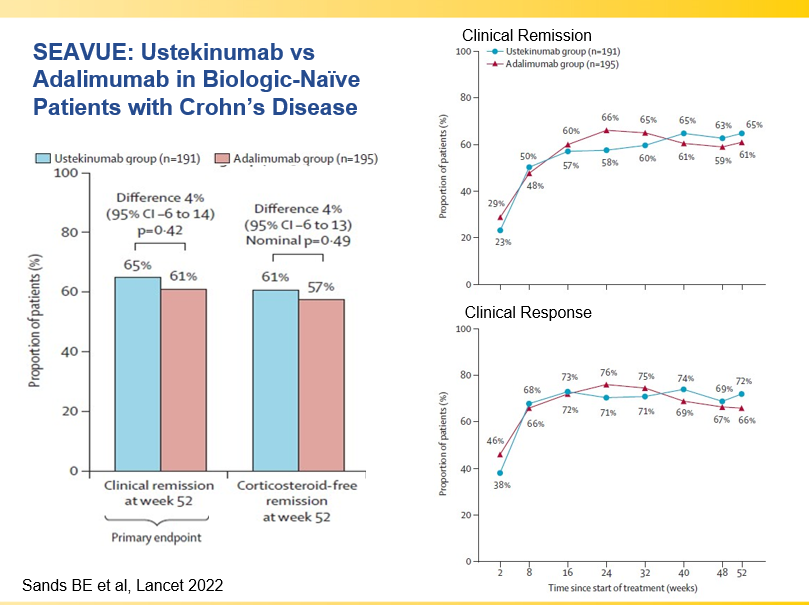
Recent studies show that ustekinumab is effective in children. Also, in patients who respond to ustekinumab, there is good durability
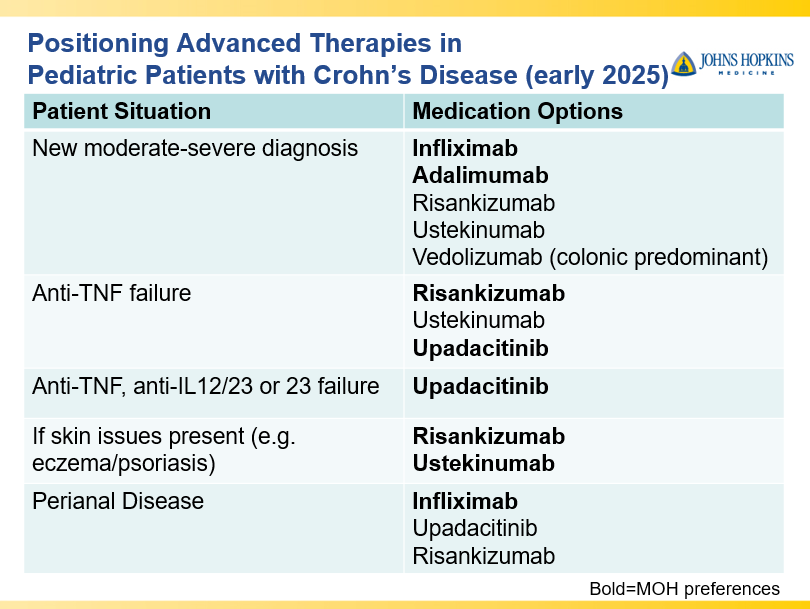
Infliximab is a top-line therapy in Crohn’s disease
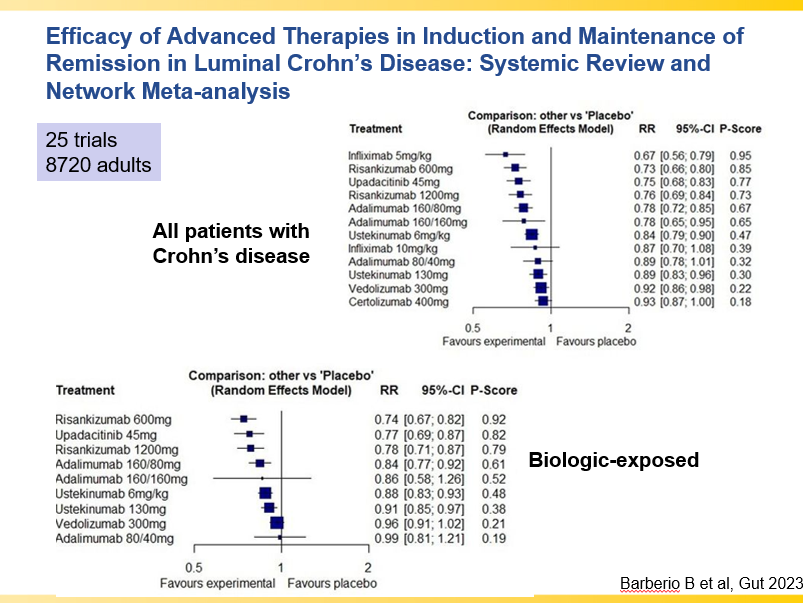
Risankizumab is a top-line therapy in both biologic-naive and biologic-exposed patients with Crohn’s disease. Higher maintenance doses may capture more patients.
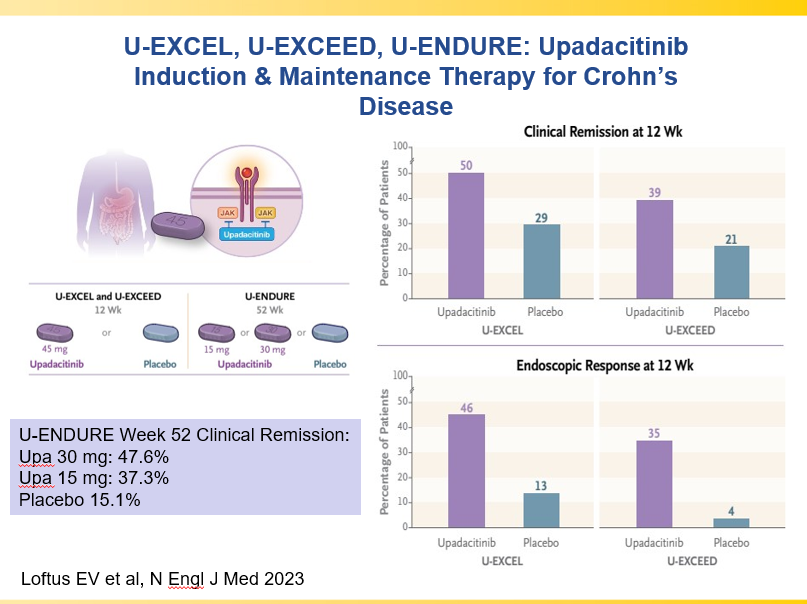
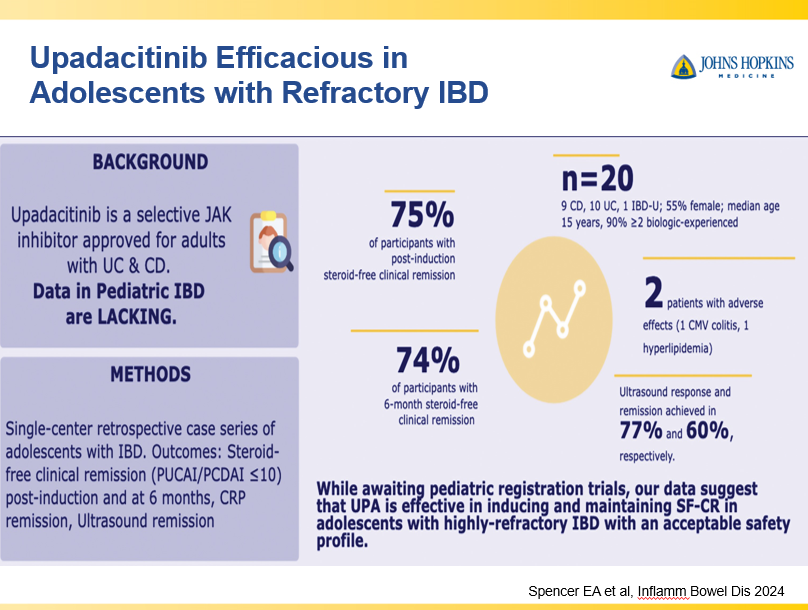
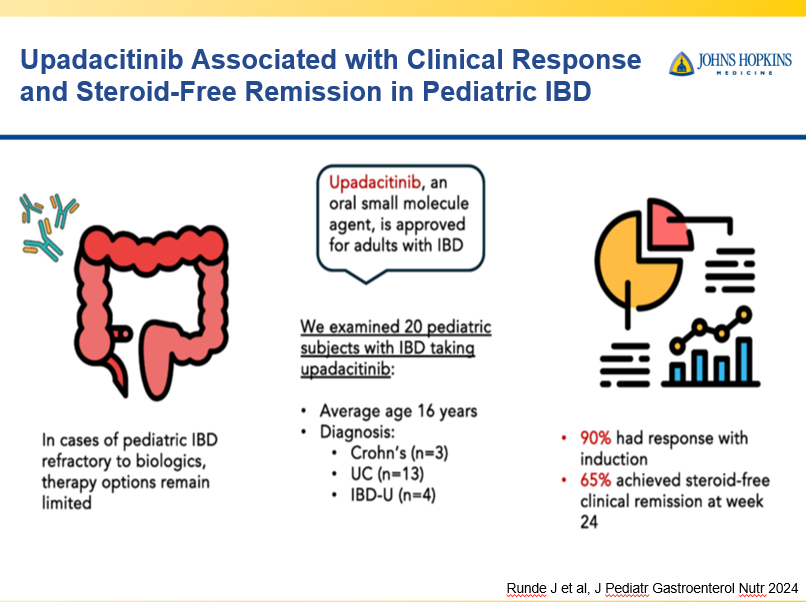
Upadacitinib is a very good therapy in patients with prior advanced therapies with either Crohn’s or ulcerative colitis. It also has a rapid onset of action (within 2 weeks)
Vedolizumab is less effective in those who are biologic-exposed. However, patients with predominantly colonic (UC-like) involvement may be better-suited for this therapy
Close monitoring and treat-to-target approaches are recommended. Usually followup scope is undertaken after one year (&/or one year after switching therapy)
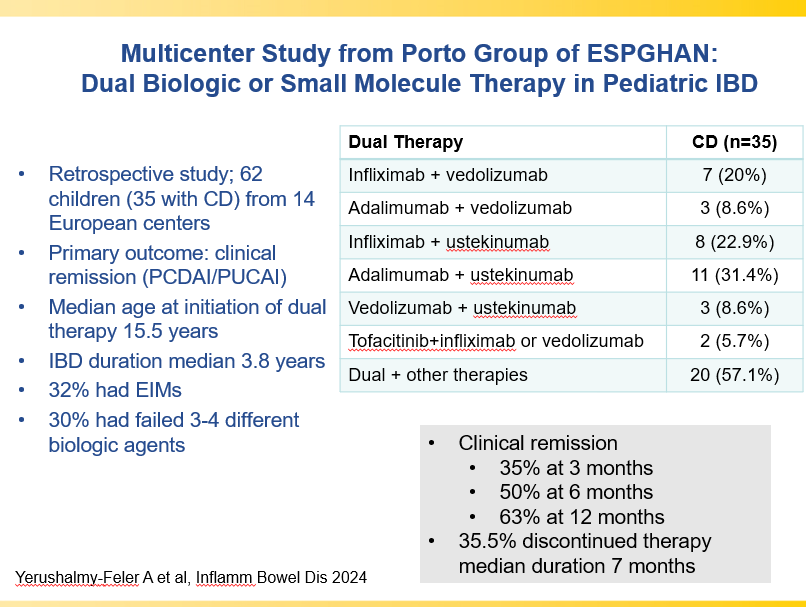
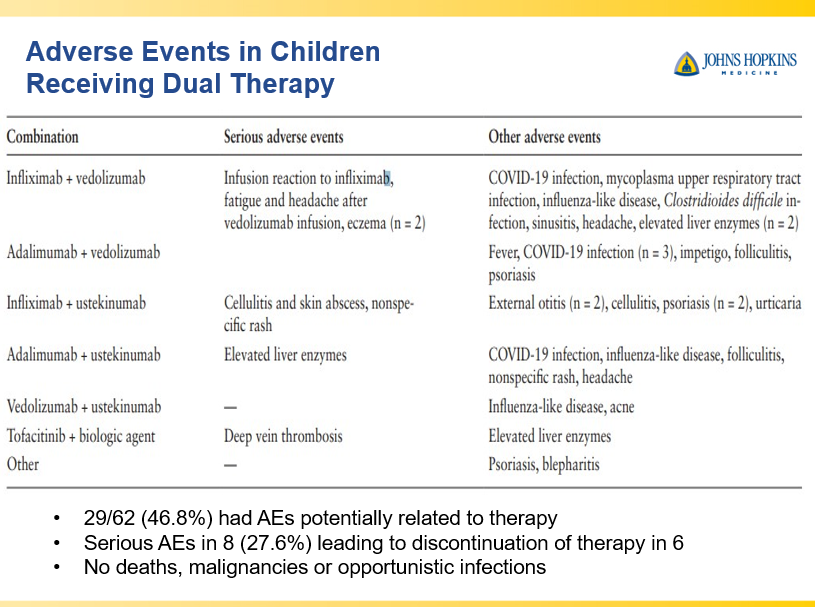
Combination advanced therapies have shown effectiveness but it is unclear which combinations are optimal
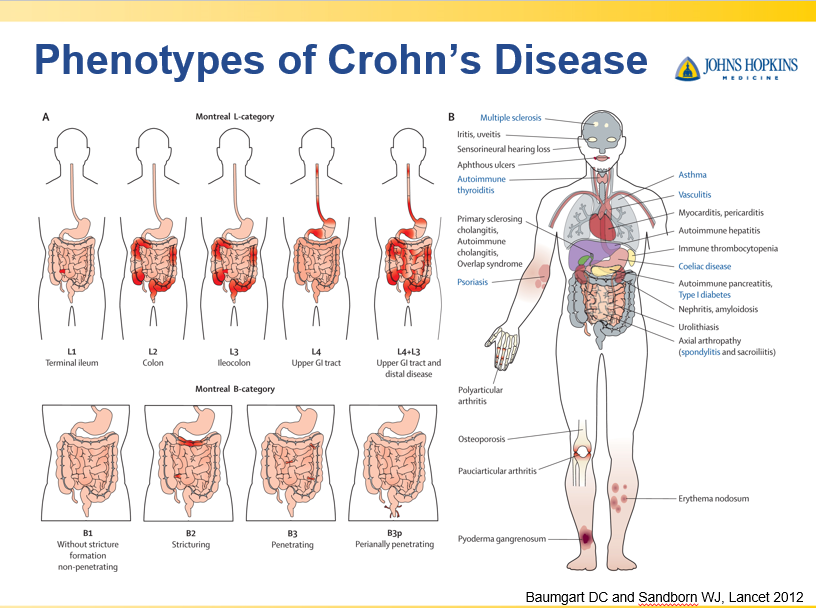
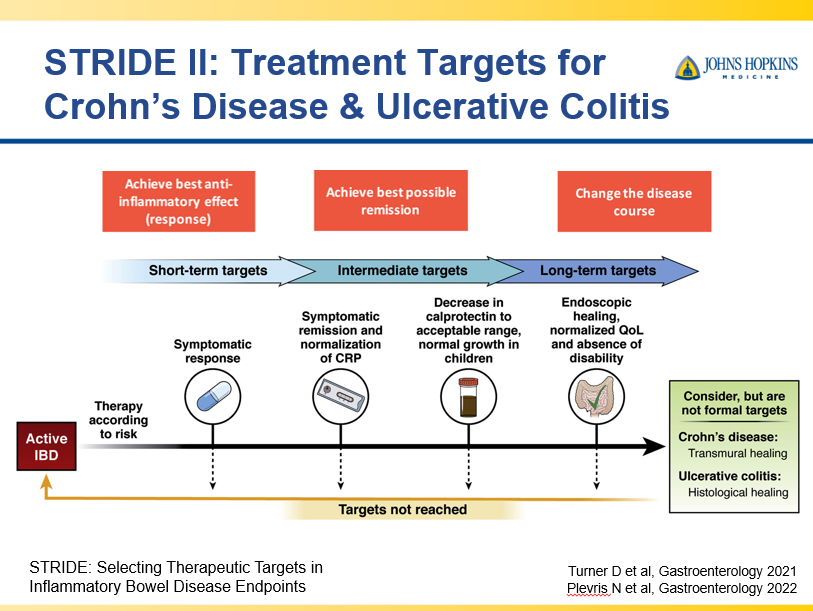
This slide shows the Montreal Classification, an organ-based phenotype, to describe the anatomic extent and behaviors of Crohn’s disease;. The figure on the right illustrates extraintestinal manifestations of IBD. It is expected that disease classification will rely more on a molecular based approach.The STRIDE project which defined goals of treatment was the result of consensus achieved by the International Organization of IBD. The first recommendations came out in 2015 and then these were updated in 2021 to incorporate a pediatric component.The PROFILE study with 386 adults showed how important early effective advanced therapies. Patients receiving infliximab/azathioprine within a median of 15 days from diagnosis had remarkably better outcomes compared to step up treatment with prednisone + azathioprine. The cytokine IL12 and IL23 shown as circles with 2 subunits attaching to their receptors share a p40 subunit (shown in red). Ustekinumab binds to that p40 subunit thereby inhibiting both the IL12 and IL23 pathways. IL23 inhibitor. Risankizumab, Mirkizumab, Guselkumab inhibit only the p19 subunit (shown in blue) and so they only downregulate the IL-23 pathway. Jak inhibitors targets are intracellular in location. Pediatric data: Multicenter 2015-2020; primary outcome was CS-free remission after 1 yr. Prior to use, 50% failed 1 anti TNF and 30% 2 anti TNF. At one year, 59/101 were in steroid free remissionUpadactinib studies: Oral induction dose for UC and CD is 45 mg daily for induction and with reduction in maintenance to 30 mg or 15 mgDue to limited head-to-head studies, network meta analyses provides indirect evidence of comparative effectiveness. It relies on how effective a medication was compared to placebo. One of the problems with these comparisons is that there are different populations in each of these studies.In patients who need speed to reduce symptoms, upadacitinib is favored over IL-23 agents
Though Dr. Oliva-Hemker’s lecture did not focus on ulcerative colitis, she did note that their center has recommended frequent colonoscopies (often yearly) in many of their patients with the combination of ulcerative colitis and PSC. This is due cases of colon cancer in their pediatric cohort.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Congratulations to Dr. Benjamin Gold who is one of the honored heros at this year’s CCFA Take Steps. Also, congratulations to Clara Cann and Lauren Leonard who are being recognized as well.
In the REPREVIO study, a double-blind, randomized, placebo-controlled trial, 80 adults received either vedolizumab (300 mg IV) (n=43) or placebo (n=37) at weeks 0, 8, 16 and 24 following ileocolonic resection and had one or more risk factors for recurrence.
Key findings:
At week 26, the probability of a lower modified Rutgeerts score with vedolizumab versus placebo was 77·8% (95% CI 66·4 to 86·3; p<0·0001).
Severe endoscopic recurrence was observed in ten (23·3%) of 43 patients in the vedolizumab group versus 23 (62·2%) of 37 patients in the placebo group (difference –38·9% [95% CI –56·0 to –17·3]; p=0·0004).
Adverse effects were noted in three patients who received vedolizumab (bilateral tubo-ovarian abscesses, thrombosed hemorrhoids, and pancreatic adenocarcinoma) and two patients who received placebo (intestinal perforation related to Crohn’s disease and severe abdominal pain)
My take: This study shows that vedolizumab is another biologic capable of reducing postoperative recurrence following ileocolonic resection in Crohn’s disease. Infliximab has been shown to reduce recurrence as well (shown in the PREVENT study).
MT Fioretti et al. J Pediatr Gastroenterol Nutr. 2025;80:300–307. A decade of real-world clinical experience with 8-week azithromycin–metronidazole combined therapy in pediatric Crohn’s disease
Methods: This retrospective study over 10 years examined the efficacy of azithromycin-metronidazole for induction treatment in 44 children. All patients were given metronidazole (15–20 mg/kg/day two times daily, maximum of 1000 mg/day) administered daily for 8 weeks and azithromycin (7.5 mg/kg to a maximum of 500 mg/once a day) administered 5 days per week for the first 4 weeks, followed by 3 days per week for the final 4 weeks as per the initial publications.17, 18
Key findings:
After 8 weeks, the overall remission rate was 64%.
Of the 38 patients who completed the CD AZCRO course, 28 patients (74%) entered remission (Group 1) and 10 (26%) did not (Group 2)
After 8 weeks, Group 1 showed improved CRP levels and higher albumin and hemoglobin levels than Group 2. Median FC declined significantly from 650 mcg/g at baseline to 190 mcg/g at Week 8 in Group 1 (p < 0.001).
The authors conclude that “a combination treatment of azithromycin and metronidazole represents an alternative induction therapy for mild to moderate pediatric CD, offering benefits in terms of cost and practicalities compared to EEN and in side effects compared to steroids.”
My take: There are a small number of children with mild Crohn’s disease who could benefit from this induction regimen. An alternative would be the use of a more modest dietary approach (eg. Mediterranean diet)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Twenty-eight studies involving 153,027 patients with IBD were included.
Key findings:
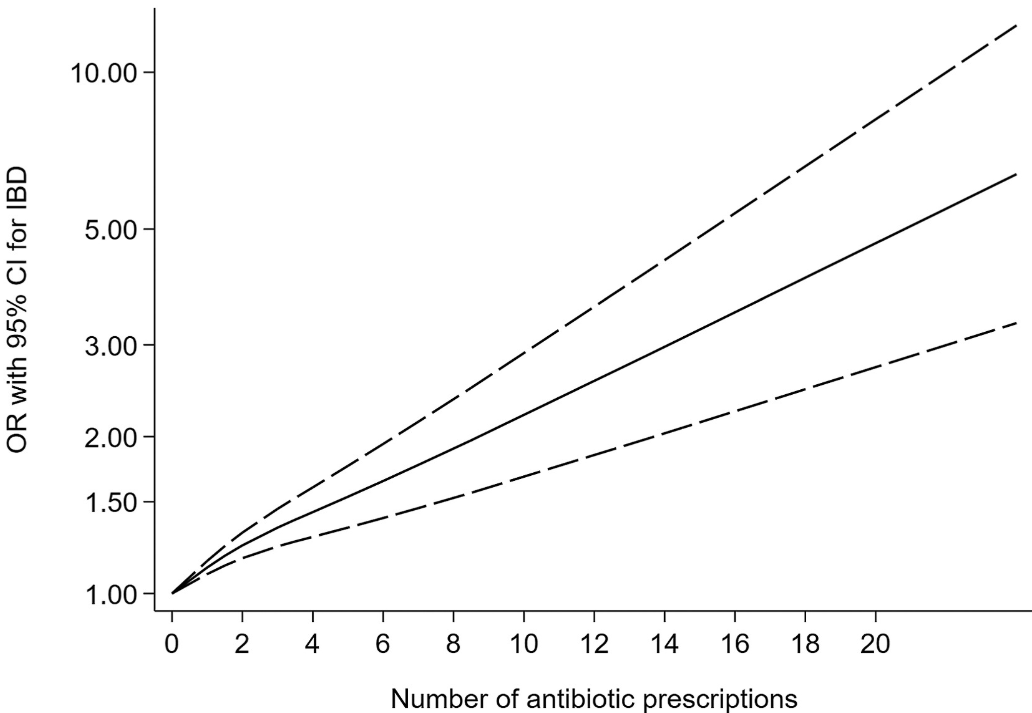
Antibiotic exposure was significantly associated with an increased risk of new-onset IBD for prescription-based studies (pooled OR, 1.41; 95% CI, 1.29–1.53) and for questionnaire-based studies (pooled OR, 1.35; 95% CI, 1.08–1.68). ‘
This association existed for both Crohn’s disease and ulcerative colitis, as well as in children and adults for prescription-based studies.
Some of the limitations:
There was statistical heterogeneity was high in the primary analysis, possibly because of inconsistencies in study design
Most studies included a clear lag time, yet an inadequate lag time still creates the possibility of reverse causality.
The authors could not disentangle the risk of antibiotics from the risk of infection in leading to the development of IBD.
Nonlinear dose-response relationship between antibiotic exposure and risk of new-onset IBD (solid black line and short dash black line represent estimated ORs and corresponding 95% CIs of nonlinear relationship)
My take: This is another study showing an association between antibiotic use and new-onset IBD. While this study does not prove causation, it is another reason for good antibiotic stewardship.
Methods: VIVID-1 was a global phase 3, randomized, double-blind, double-dummy, placebo-controlled and active-controlled, treat-through study which enrolled 1150 patients with moderate-to-severe Crohn’s disease. There were three treatment groups: mirikizumab group, ustekinumab group, and placebo group. In each group, 48-49%were considered “biologic-failures” including 45-46% who were anti-TNF failures.
Key findings:
Discussion points:
Early treatment effect: “Symptomatic improvement was evident as early as week 4 accompanied by a statistically significant reduction in high-sensitivity CRP and faecal calprotectin, and endoscopic response was seen at week 12.”
Compared to ustekinumab: “Mirikizumab reached non-inferiority versus ustekinumab for clinical remission by CDAI at week 52…mirikizumab showed statistically significantly greater improvements from baseline in fecal calprotectin and CRP compared to ustekinumab. In addition, a greater percentage of patients reached the combination endpoint of endoscopic response and clinical remission by CDAI at week 52.”
Comparison across treatment trials: “. At week 52, 45∙4% of patients treated with mirikizumab met the endpoint of clinical remission by CDAI in the treat-through analysis with composite endpoint, 54∙1% met the endpoint in the treat-through analysis, and 64∙3% met the endpoint in the responder analysis. This example, with a range of nearly 20% percentage points depending on analysis type, shows the profound limitations in comparing unadjusted outcomes across phase 3 trials.” The authors note other differences in trial design between VIVID-1 and SEQUENCE (risankizimab) and state “no conclusions on relative efficacy can be drawn.”
My take: This study shows that mirikizumab is effective in adults with moderate-to-severe Crohn’s disease with and without prior biologic treatments. Pediatric studies are underway.
Background: The exposure–response relationship for the intravenous (IV) formulation of infliximab is well established, with multiple studies demonstrating that higher trough concentrations (C-trough) are associated with improved patient outcomes…However, the 2-week cycle of subcutaneous administration showed many-fold higher C-trough than the 8-week cycle of IV-IFX. Direct comparison of C-trough between SC- and IV-IFX is not appropriate because of different bioavailability and concentration–time profile. It is also not appropriate to apply the C-trough thresholds that predict achieving the therapeutic targets for IV.
This was a cross-sectional retrospective study with 124 patients with Crohn’s disease (CD) who had received SC-IFX maintenance therapy for ≥6 months. SC-IFX C-trough was measured immediately before SC-IFX injection. Key findings:
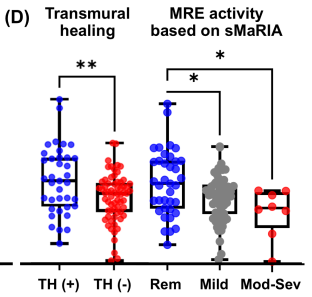
Mucosal healing (MH) was noted in 77.9% (74/95) and transmural healing (TH) in 36.3% (37/102).
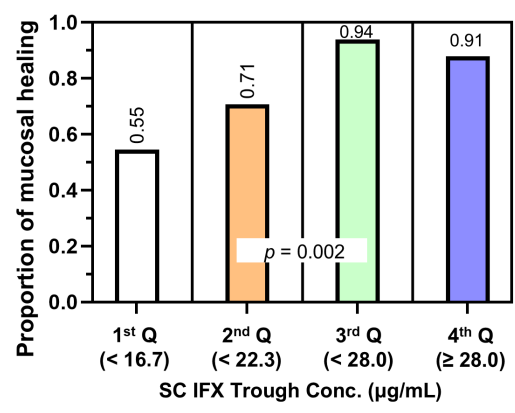
SC-IFX C-trough was significantly higher in patients with MH (24.1 vs.16.9 μg/mL; p=0.001) and TH (26.0 vs. 20.5 μg/mL; p=0.007) than in those without.
Discussion:
Target trough levels: In this study, the authors found that “the C-trough thresholds for clinical remission, biochemical remission, MH and TH were 12, 16, 18 and 30 μg/mL, respectively, based on ROC analysis. The C-trough of SC-IFX increased with the depth of remission.”
Why trough level targets may differ between IV administration and SC: Administration via the IV route results in early and rapid peak concentration followed by a steady decline to trough, whereas administration via the SC route has slower absorption, lower bioavailability, lower peak concentration and smaller differences between peak and trough concentrations.
The authors note that a study by Ye et al (United European Gastroenterology Journal; 2020: 8: 385–386) with 55 patients found that a C-trough >26.6 mcg/mL achieved clinical remission and fecal calprotectin levels <250 mcg/g at week 54 in 79% and 91% respectively compared to 46% and 62% in those with with C-trough <16.4 mcg/g.
These C-trough levels are significantly higher that the median C-trough levels of standard dosing (120 mg biweekly) in a phase 1 dosing RCT which was only 13.3 mcg/mL (S Schreiber et al. Gastroenterology 2018; 154: 1371). The dosing of 180 mg and 240 mg biweekly resulted in C-trough levels of 19.9 mcg/mL and 26.5 mcg/mL respectively.
My take: This study suggests that therapeutic drug monitoring will have different targets with SC-IFX than with IV-SC. SC formulations will offer more convenience. However, more effort will be needed to make sure patients are adherent with therapy in order to achieve optimal outcomes.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.