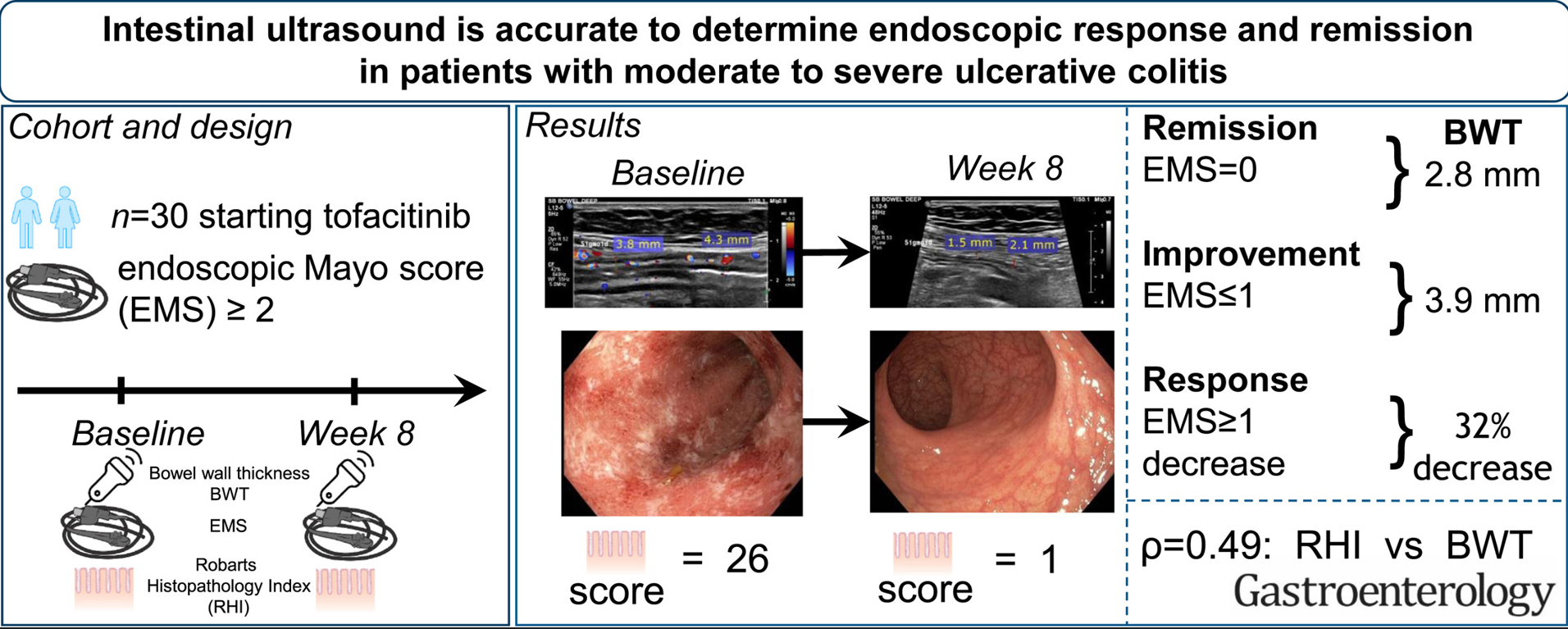
F De Voogd, et al. Gastroenterol 2022; 163: 1569-1581. Intestinal Ultrasound Is Accurate to Determine Endoscopic Response and Remission in Patients With Moderate to Severe Ulcerative Colitis: A Longitudinal Prospective Cohort Study
27 patients with moderate to severe ulcerative colitis (UC) completed followup in this single-center, prospective, longitudinal cohort study. Key findings:
- Bowel wall thickness (BWT) correlated with endoscopic Mayo score. “The most accurate cutoff for BWT was 2.8 mm for endoscopic remission, 3.9 mm for improvement, and a decrease of 32% for response.”
The associated editorial (C Palmela, C Maaster. Gastroenterol 2022; 163: 1485-1487. Open Access! The Use of Intestinal Ultrasound in Ulcerative Colitis-More Than a Mucosal Disease?) details other studies showing the utility of intestinal ultrasound, including the TRUST%UC study which enrolled 253 patients with UC. “. At baseline, 88.5% of patients had increased bowel wall thickness (BWT). Response to therapy could be detected as early as 2 weeks after initiation of therapy, as shown by reduction of abnormal BWT.” In anothre study with severe UC, “BWT reduction of >20% being an excellent predictor of response to intravenous steroids at 48 hours, as shown recently by Ivemark et al.10“
The editorial notes that intestinal ultrasound “is often thought as being operator dependent. Nonetheless, several studies have shown an excellent inter-observer agreement in IUS, especially for the assessment of BWT,7,12 as was also found in this [De Voogd] study.” An additional finding in the De Voogd study was that the “the submucosa was the most thickened layer, and after 8 weeks of therapy it was also the most responsive layer;” thus, UC is not simply a mucosal disease.
My take: This study shows that with more widespread adoption, many UC patients could be followed non-invasively with intestinal ultrasound (and calprotectin).
Related blog post: