TikTok: High Drug Costs and Pharmacy Benefits Managers. Thanks to Anna Kelly for this link.


TikTok: High Drug Costs and Pharmacy Benefits Managers. Thanks to Anna Kelly for this link.
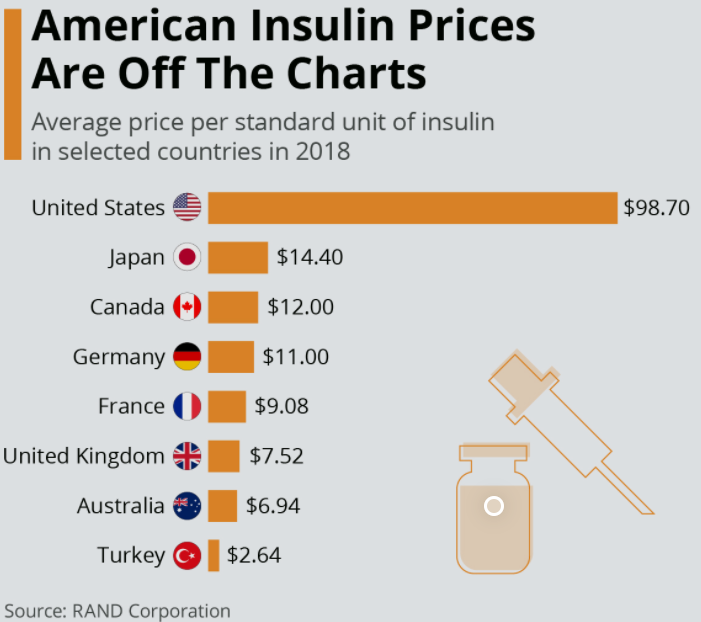
Fortune Dec 2021-Jan 2022: Insulin’s Deadly Cost Thanks to Stan Cohen for sharing article.
Some excerpts/key points:
My take: “The story of insulin is a poster child for everything that’s wrong with a free-market approach to drug availability,” says Arthur Caplan…”It’s almost inexcusable morally.”
Related blog posts:
Day-to-day, I find I am focused (?inundated) on problems that are literally right in front of me. Every once in a while, it is important to look more broadly and try to consider/address the larger issues.
Along those lines, I would recommend a series of important articles on adolescent nutrition published by The Lancet. Thanks to William Balistreri for sharing these references.
1. GC Patton et al. Nourishing our future: the Lancet Series on adolescent nutrition. DOI:https://doi.org/10.1016/S0140-6736(21)02140-1
This is an introduction to the series of articles. “Given these increasingly transnational
dimensions of the ultra-processed food industry, it is timely for WHO, the Food and Agriculture Organization of the UN, and their partners to revisit calls for global regulatory frameworks to assist governments in taking action. Given the speed of nutritional change, there is perhaps no greater immediate threat to the health of adolescents. Equally, tackling adolescent nutrition presents an unparalleled opportunity to interrupt intergenerational cycles of malnutrition and respond to the urgent challenges of planetary change”
2. SA Norris et al. Nutrition in adolescent growth and development. DOI:https://doi.org/10.1016/S0140-6736(21)01590-7
3. LM Neufeld et al. Food choice in transition: adolescent autonomy, agency,
and the food environment. DOI:https://doi.org/10.1016/S0140-6736(21)01687-1
Key points:
4. D Hargreaves et al. Strategies and interventions for healthy adolescent growth,
nutrition, and development. DOI:https://doi.org/10.1016/S0140-6736(21)01593-2
Key Points:
My take: If we truly hope to improve population health, improving diet choices cannot remain the province of only the well-educated wealthy. Adolescence offers a chance to change health trajectories before habits are more rigid and before the development of fixed health consequences.
Related blog posts:

JF Ludvigsson et al. J Pediatr 2021; 238: 66-73. Open Access PDF Serious Infections in Pediatric Inflammatory Bowel Disease 2002-2017—A Nationwide Cohort Study
This study utilized the Swedish nationwide health registry (2002-2017; n = 5767 with IBD) and controls from the general population (n= 58,418). One reason for this study is the increased frequency and changing patterns of immunosuppressive medications that are being used in pediatric IBD. Key findings:
Potential risk factors for infection, besides medications, include malnutrition, chronic inflammation, impaired response to vaccination, and dysregulation of immune responses. A limitation of this study is ascertainment bias as families/patients with underlying disease may be more likely to seek medical attention for otherwise self-limited infections.
My take: This report confirms and quantitates daily clinical practice: children with IBD are more frequently hospitalized due to infections.
Related blog post: Infection or Flareup in IBD: GI PCR Panel Helps
A recent commentary (PJ Zettler et al. NEJM 2021; 385: 2409-2411. A Divisive Ruling on Devices — Genus Medical Technologies v. FDA) highlights another challenge facing the FDA’s role in regulating devices, especially as the definition of devices and medications becomes more murky.
Key points/excerpts:
My take: This commentary shows the difficulties the FDA faces as the judiciary curtails its discretion. While the legislative branch could codify FDA authority, this is unlikely. As such, this will limit FDA oversight in some new medical products. When problems arise, it is likely that the FDA (not the courts) will be blamed despite the fact that their ability to regulate has been undermined.
Related blog posts:


J Uhanova et al. Clin Gastroenterol Hepatol 2021; 19: 2417-2424. Chronic Liver Disease and Metabolic Comorbidities in Healthy Young Males Followed for 65 Years: The Manitoba Follow-up Study
Methods: 3,983 air force men were enrolled in the Manitoba Follow-up Study in 1948. The comprehensive database on results of routine physicals and health encounters was examined for evidence of chronic liver disease (CLD) and metabolic syndrome (MetS).
Key findings:
Discussion –The authors note that the lifetime risk of CLD was much higher in NHANES studies (11.8% to 14.8% prevalence); this is attributed to active surveillance for liver disease in the NHANES study (and different study population). It is also likely that there is a substantially increased risk over the last 65 years due to factors like increasing rates of obesity as well as possibly higher rates of alcohol use and infections.
My take: Among healthy 18 year old males, a substantial number develop chronic liver disease, much of which could be prevented by limiting alcohol intake and maintaining a healthy diet/exercise.
Related blog posts:

KO Hensel et al. J Pediatr 2021; 238: 50-56. Sclerosing Cholangitis in Pediatric Inflammatory Bowel Disease: Early Diagnosis and Management Affect Clinical Outcome
This was a retrospective study of 82 pediatric patients (31% female) with IBD-SC and a mean age at diagnosis of 11.9 ± 2.8 years who were followed up for a mean of 6.8 ± 3.3 years. Tests for SC included immunoglobulins and serology (ANA, ASMA, LKM-1, and SLA). Patients with ASC were maintained on low dose prednisolone (5 mg/day) and azathioprine (up to 2 mg/kg/day).
Key findings:
The discussion notes generally better outcomes in this cohort than in previous studies. The authors note that this may be due to earlier diagnosis (though lead-time bias could be a factor as well). To increase earlier diagnosis, the gastroenterology diagnostic pathway at one institution (CUH) includes mandatory assessment of liver function and a low threshold for performing a liver biopsy (with initial panendoscopy). Diagnosis of ASC was based on the ESPGHAN diagnostic score for AILD (JPGN 2018; 66: 345-360, related post has image with scoring: Aspen Webinar 2021 Part 5 -Autoimmune Liver Disease & PSC). Also, they note that SCOPE score “seemed to overestimate the risk for developing complications.”
My take: In those with IBD and abnormal liver enzymes/GGT, looking for SC/ASC may improve outcomes.
Related blog posts:

PR Farrell et al. J Pediatr 2021; 238: 33-41. Open Access: Cytokine Profile Elevations on Admission Can Determine Risks of Severe Acute Pancreatitis in Children
Methods: In this single center pediatric study, interleukin 6 (IL -6), monocyte chemotactic protein-1 (MCP-1) and CRP were obtained within 48 hours of admission in 66 subjects (20 controls, 36 with mild acute pancreatitis (AP), and 10 with severe AP) in a derivation cohort. and then in a validation cohort with 35 subjects (10 controls, 19 mild AP and 6 severe AP)
Key findings:
The discussion notes a few points:
My take: In clinical practice, both elevated CRP and BUN are associated with a higher risk of progression to severe pancreatitis. The reason why I was interested in this study was the potential for targeting IL-6 to improve outcomes.
Related blog posts:

NPR: New podcast examines wellness trends and beliefs, like what weight means about health. Interview with Aubrey Gordon and Michael Hobbes who co-host the podcast “Maintenance Phase.”
This interview has a lot of useful ‘food for thought.’
Some excerpts:
My take: Diets for weight loss have very low rates of success. Focusing on healthy eating habits (eg. food/beverage composition, eating together) along with encouraging healthy activity levels is likely to be most beneficial for long-term outcomes. .
Related blog posts:

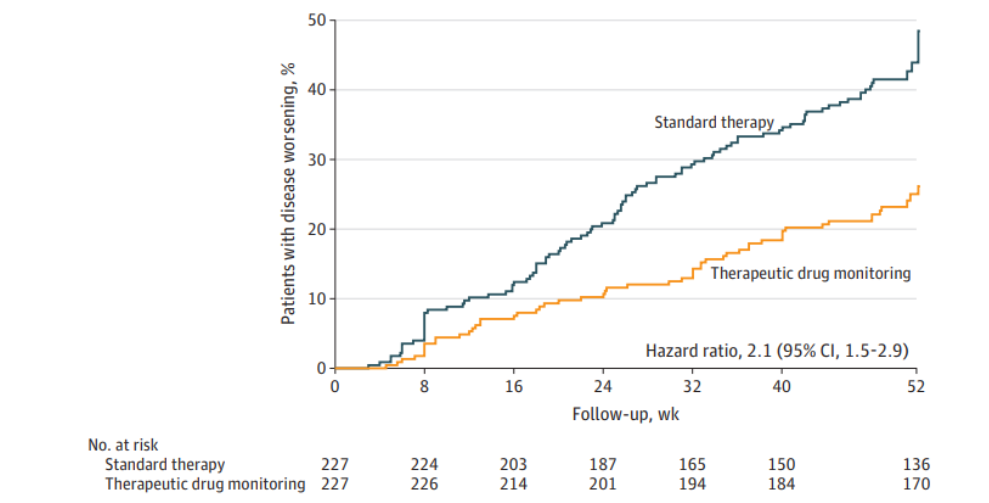
Another recent study showing the benefits of proactive therapeutic drug monitoring (pTDM):
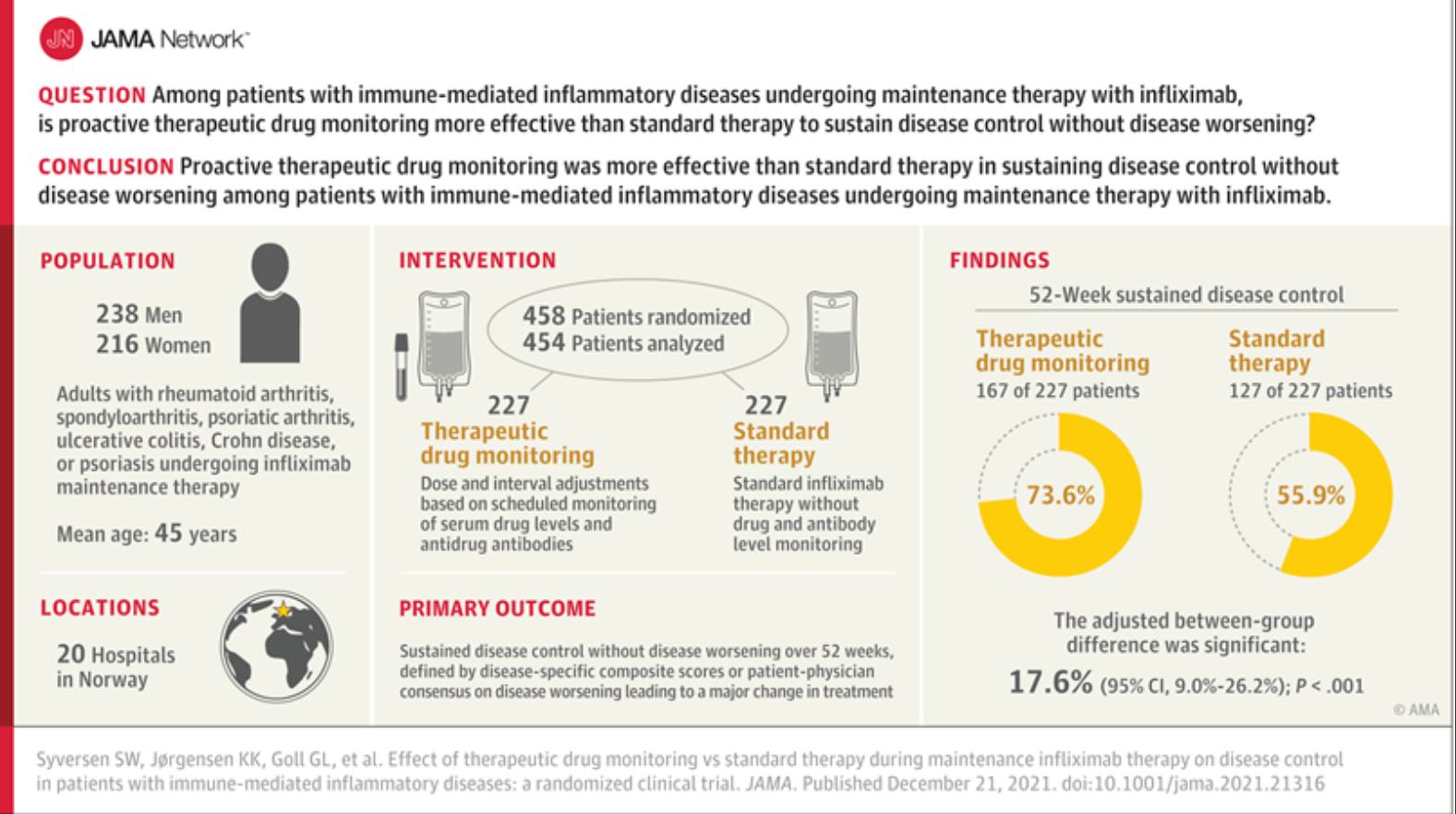
SW Syverson et al. JAMA. 2021;326(23):2375-2384. Effect of Therapeutic Drug Monitoring vs Standard Therapy During Maintenance Infliximab Therapy on Disease Control in Patients With Immune-Mediated Inflammatory Diseases (The article is only 10 pages; however, the supplementary material (which I did not read) is an additional 258 pages.) Thanks to Ben Gold for sharing article reference. Also, this study was reviewed in Healio Gastro: Link: Therapeutic drug monitoring sustains disease control during infliximab maintenance
Methods: Randomized, parallel-group, open-label clinical trial including 458 adults (mean age, 44.8 years; 49.8% women) with rheumatoid arthritis, spondyloarthritis, psoriatic arthritis, ulcerative colitis (n=81), Crohn disease (n=66), or psoriasis undergoing maintenance therapy with infliximab in 20 Norwegian hospital
Key finding:
Some limitations of this study:
My take: This study supports recent expert guidance (see blog post below) on the benefit of pTDM as part of evidence-based care. It is likely that pTDM is even more important in children/teens due to growth.
Related blog posts:
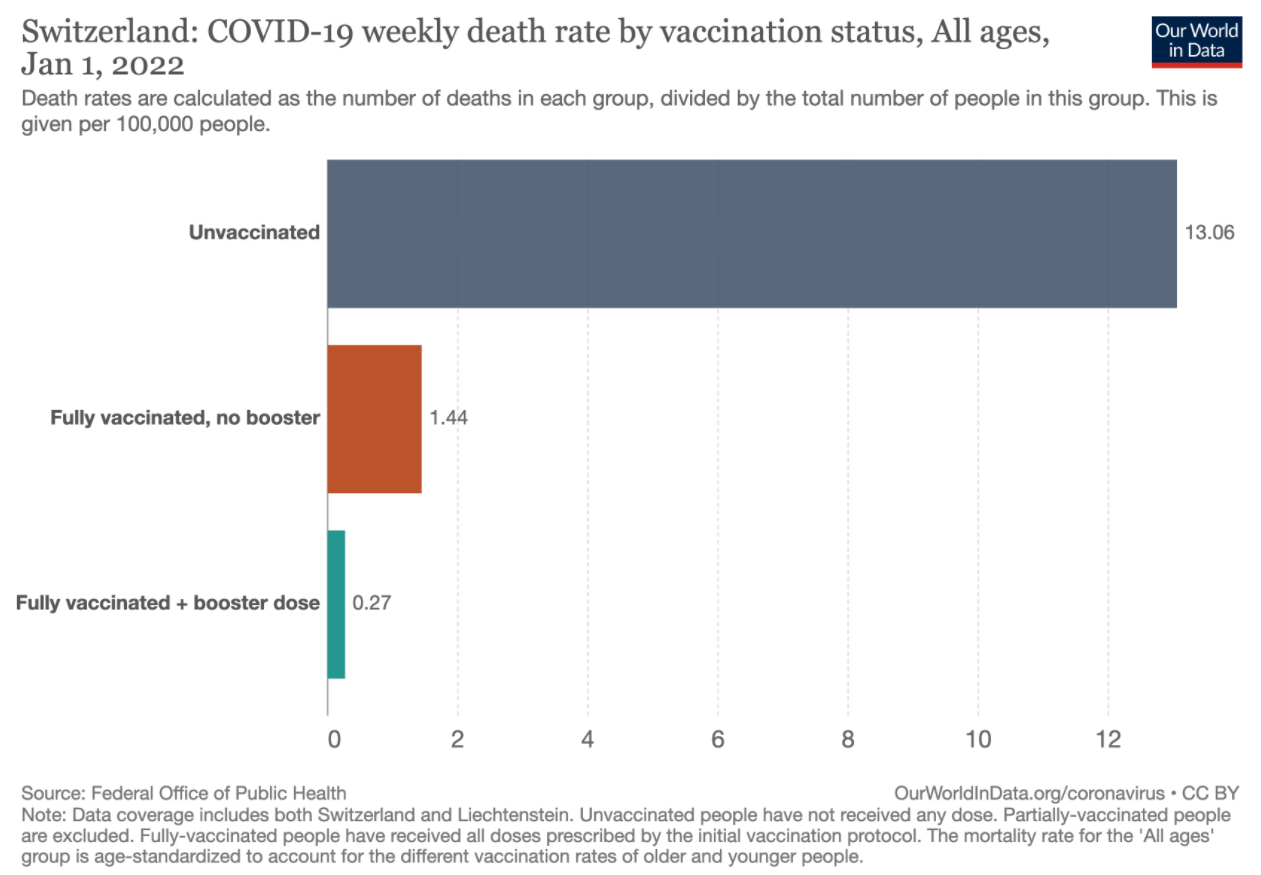
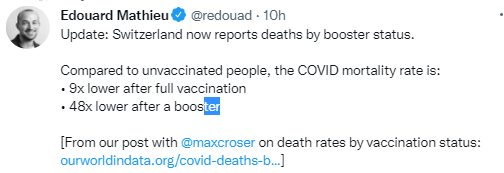
Also data from Switzerland: